Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
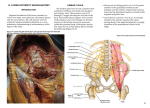
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BANGALORE. ANNEXURE II PROFORMA FOR REGISTRATION OF SUBJECT FOR DISSERTATION 6. Brief Resume of the intended work : 6.1 Need for the study : Neurology is one important branch of medicine, which is dependent on an accurate knowledge of anatomy as a basis for the diagnosis and localization of neural disturbances. The nerve supply to lower limbs is derived from lumbar and sacral plexuses. The lumbar plexus as a whole shows many variations in the composition and formation. Segmental distribution of both the motor and sensory fibres of lumbar nerve roots is important in the localization of lesions of lumbar spine for the orthopedic surgeon and is also relevant in this study. Regional anaesthesia of the inguinal region used in patients undergoing surgical manipulation of the inguinal canal, spermatic cord and testes. Lumbosacral trunk compression at the pelvic brim by the foetal head or mid pelvic forceps causes maternal obstetric paralysis. Compression of femoral nerve by surgical retractor blades and angulation of femoral nerve under the inguinal ligament during prolonged lithotomy position causes postnatal maternal complications. Hence, the present study is undertaken to study the lumbar plexus and its variations in human adults, the precise knowledge of which is essential to the physicians, surgeons, orthopedic surgeons, anaesthesiologist and gynaecologists for physiological, surgical and anaesthetic applications. 6.2 Review of literature : The lumbar plexus lies within the substance of the posterior part of psoas major, anterior to the transverse process of the lumbar vertebra. It is formed by the first three and most of the fourth lumbar ventral rami. The fourth is often termed the nervusfurcalis, being divided between the lumbar and sacral 1 plexuses. The first lumbar ventral ramus, joined by a branch from the twelth thoracic ventral ramus bifurcates and the upper and larger part divides again into iliohypogastric and ilioinguinal nerves. The smaller lower part unites with a branch from the second lumbar ventral ramus to form the genitofemoral nerve. The remainder of the second, third and part of the fourth lumbar ventral rami join the plexus and divide into ventral and dorsal branches. Ventral branches of the second to fourth rami join to form the obturator nerve. The main dorsal branches of the second to fourth rami join to form femoral nerve. Small branches from the dorsal branches of the second and third rami join to form the lateral femoral cutaneous nerve. The accessory obturator nerve, when it exists, arises from the third and fourth ventral branches.1 The lumbar plexus may being as high as the 11th thoracic ventral ramus (prefixed variety) or as low as the first lumbar (post fixed variety). Extreme cases like nervus furcalis with L3, L4 (pre fixed) or L5 (post fixed); obturator with L1, 2,3 (pre fixed) or L2, 3,4,5 (post fixed) and femoral with T12, L1, L2 (pre fixed) or L2, 3,4,5 (post fixed) have been observed. The commonest variation is towards the post fixed variety and some evidence exists that vertebral anomalies are often associated.2 In one study of 64 lumbar plexuses. 47 were formed by four spinal nerves, 14 by five and 3 plexuses by six spinal nerves. The plexus is frequently asymmetric bilaterally. Range of variations include lateral femoral cutaneous with L1, 2 (pre fixed) or L3, 4 (post fixed); femoral with T12-L4 (pre fixed) or L1 – L5 (post fixed): obturator with L1-L4 (pre fixed) or L2-L5 (post fixed); and furcal with L3,4 (pre fixed) or L4, 5 (post fixed).3 A case of complex bilateral variation in lumbar plexus has been reported . On the left side the plexus was postfixed and located posterior to thepsoas major muscle. The femoral nerve was formed by the union of anterior rami of the second, third, fourth and fifth lumbar spinal nerves. On the right side, the 2 lumbar plexus was prefixed. The lateral cutaneous nerve of the thigh was formed by the union of the anterior rami of the first and second lumbar spinal nerves. The femoral nerve formed by branches from the first, second, third and fifth lumbar spinal nerves while the obturator nerve was formed by the union of the first second and third lumbar spinal nerves.4 The origins, courses and relations of lateral femoral cutaneous nerves were examined bilaterally in 28 cadavers, and the variations were observed in two. On the right side of one cadaver, the ventral rami of the first and second lumbar spinal nerves were united and then this nerve was divided into four branches. From medial to lateral, these branches were the obturator nerve, the femoral nerve, the medially located and laterally located lateral femoral cutaneous nerves. On the left side of another cadaver, there were three lateral femoral cutanoeus nerves. All these nerves pierced the psoas major muscle anterolaterally.5 Multiple variations of the nerves arising from the lumbar plexus were found on the right side of a 35 year old female cadaver. Lateral femoral cutaneous nerve arising from the femoral nerve, double ilioinguinal nerves, and an accessory nerve branch joining to the genital branch of the genitofemoral nerve.6 6.3 Objectives of the study : 1. To study variations in formation and branches of lumbar plexus in South Indian (Karnataka) cadavers. 7. Material and methods : 7.1 Source of data : Adult human cadaver belonging to both the sexes procured from the Department of Anatomy, J.J.M. Medical College, Davangere. 7.2. Method of collection of data (including sampling procedure if any): 3 1. Dissection method. 2. Collection of data material by the other workers in this field. 3. Sample size 30. 7.3 Does the study require any investigations or interventions to be conducted on patients or other humans or animals? If so, please describe briefly. No. 7.4. Has ethical clearance been obtained from your institution in case of 7.3? No. 8. References : 1. Standring S. Gray’s anatomy. The anatomical basis of clinical practice. 39th Edn., London : Elsevier Churchill Livingstone; 2005. p.1124. 2. Romanes GJ. Cunningham’s text book of anatomy. 12th edn., Oxford : Oxford University Press; 1981. p.791. 3. Bergman Ra, Thompson SA, Afifi AK, Saadeh FA. Compendium of human anatomic variation. Germany : Urban and Schwarzenberg BaltimoreMunich; 1988. p.143. 4. Erbil KM, Onderoglu S, Baser R. Unusual branching in lumbar plexus : Case report. Okajimas Folia Anat Jpn 1999 May; 76(1): 55-9. 5. Erbil KM, Sargon FM, Sen F, Ozturk H, Tascioglu B, Yener N, et al. Examination of the variations of lateral femoral cutaneous nerves : report of two cases. Anat Sci Int 2002 Dec; 77(4): 247-9. 6. Uzmansel D, Aktekin M, Kara A. Multiple variations of the nerves arising from the lumbar plexus : Neuroanatomy 2006; 5: 37-39. 4