Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug design wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Environmental impact of pharmaceuticals and personal care products wikipedia , lookup
Drug interaction wikipedia , lookup
Theralizumab wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
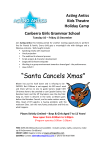
A-688 Lefamulin (BC-3781) The Pharmacokinetics of Lefamulin (BC-3781) in the Pulmonary Epithelial Lining Fluid in Healthy Subjects OH OH O S O M. Zeitlinger1, D.B. Strickmann2, W.W. Wicha2, R. Schwameis1, B. Burian1, M. Müller1, W.T. Prince2 1 Medical University of Vienna, Austria; 2 Nabriva Therapeutics AG, Vienna, Austria Nabriva Therapeutics AG Leberstrasse 20 A-1110 Vienna, Austria www.nabriva.com +43-1-74093-0 [email protected] H H2N O ABSTRACT Background: Lefamulin (BC-3781) is an investigational semisynthetic pleuromutilin derivative inhibiting ribosomal protein synthesis. Lefamulin is entering Phase 3 clinical development with a spectrum of activity suitable for treating respiratory tract infections including multidrug resistant S. pneumoniae, atypical respiratory pathogens and S. aureus (MRSA and MSSA). Since knowledge of the pharmacokinetics (PK) at the site of infection is crucial in the development of antibiotics, for the treatment of respiratory tract infections such as community- and hospital-acquired bacterial pneumonia (CABP & HABP) drug penetration into the pulmonary epithelial lining fluid (ELF) is a pre-requisite. The present study examines the PK of lefamulin in the ELF in comparison to the plasma. Methods: A single dose of 150 mg lefamulin was administered intravenously (i.v.) over 1 hour to 12 healthy male subjects. Bronchoalveolar lavage (BAL) was used to obtain ELF samples 1, 2, 4 and 8 hours after dosing and the urea dilution method was employed to correct for the dilution factor. Drug levels in plasma and ELF were subsequently quantified by LC-MS/MS analysis. Results: After a single i.v. dose of 150 mg lefamulin the mean area under the concentration-time curve (AUC0-12h) was 6022 ± 1365 ng·h/mL for the total and 782.9 177.5 ng·h/mL for the calculated free concentration in plasma. For ELF the AUC0-12h calculated from extrapolated C12h was 4489 ng·h/mL, resulting in an AUC0-12h ratio of lefamulin in ELF compared to free drug in plasma of 5.7. Approximately 1 h after end of infusion the lefamulin levels in ELF approached the total plasma levels with elimination from ELF following the same time course as for plasma. Lefamulin was safe and well tolerated and there were no clinically relevant changes in laboratory values. Conclusions: After a single i.v. dose of lefamulin exposure levels in ELF were comparable to total plasma levels and considerably exceeded free plasma levels. The individual lefamulin concentration levels in ELF equilibrated with the plasma rapidly after the end of infusion. The exposure levels seen in the ELF are encouraging for the use of lefamulin in the treatment of respiratory tract infections and will be used for target attainment analysis. INTRODUCTION Lefamulin (BC-3781) is an investigational semi-synthetic pleuromutilin derivative. Pleuromutilin antimicrobial agents inhibit protein synthesis through interaction with the 50S ribosomal subunit and cross resistance with other antimicrobial classes is uncommon. Lefamulin has demonstrated potent antimicrobial activity against Gram-positive cocci and Gram-negative pathogens relevant for community-acquired bacterial pneumonia and for bacterial skin and skin structure infections. Since lefamulin is being developed for the treatment of serious bacterial pneumonia caused by Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Mycoplasma spp., Chlamydophila pneumoniae, Legionella pneumophila, and INTRODUCTION (cont‘d) METHODS (cont‘d) Staphylococcus aureus, including drug resistant strains such as MRSA, it is important to investigate the penetration of lefamulin into the tissues at the site of infection. This study (NAB-BC-3781-1005) was undertaken to investigate the penetration of lefamulin into the ELF to support the treatment of patients with community-acquired pneumonia (CABP) with intravenous and oral dosing formulations. Lefamulin concentrations were determined in the plasma and ELF. saline and ELF was collected. Since BAL yields just a portion of ELF with the rest being saline, the dilution of ELF must be determined to translate measured drug concentrations in BAL to drug concentrations in ELF. For ELF dilution assessment in BAL the urea dilution method was used. The use of urea to quantify the amount of recovered ELF is based on the observation that urea freely diffuses through several body compartments including ELF. Hence, if the concentration of urea in plasma and BAL is known, the volume of recovered ELF can be calculated and consequently also the concentration of lefamulin in ELF.[2] Concentrations of lefamulin in BAL samples were corrected for the procedure related dilution of ELF by saline as follows: c(lefamulin in ELF)corr = METHODS c(lefamulin in BAL)measured/[c(urea in BAL)/c(urea in plasma)] Study population: 12 healthy male subjects aged between 18 and 55 years with no relevant medical history. Subjects underwent a screening visit including physical examination, body weight, vital signs, laboratory tests, 12-lead electrocardiography and 24 hours Holter monitoring. Subjects had to be of normal weight (BMI 1928 kg/m2 inclusive) and satisfy all the inclusion and exclusion criteria. Volunteers received standardized meals on study days and were instructed to avoid coffee, tea and any other food containing xanthines (i.e. coke, chocolate, etc.), alcohol and grapefruit juice during the entire study period. Study procedures: In the morning of the study day a peripheral venous catheter was inserted in the arm. 150 mg lefamulin in 400 mL 0.9 % saline were administered over 60 min using an infusion pump. Afterwards, subjects fasted until midday or two hours after BAL procedure, whichever was later. Lefamulin concentrations in plasma were determined at 0.5, 1, 1.25, 1.5, 2, 3, 4, 6, 8, 12, 16, and 24 h after dosing. At 1, 2, 4, or 8 h after drug administration BAL was performed to determine lefamulin concentrations in ELF. BAL was performed by an experienced professional of the Division of Pulmology, as previously described.[1] Each volunteer underwent only one BAL and time points were randomized between the subjects in order to obtain three samples per time point. Local anesthesia of the pharynx and the nasal passages was provided by applying 2% lidocain spray as an aersosol and application of 2% lidocain gel to the nose. Additionally, the tip of the bronchoscope was coated with lidocain gel. Subsequently, subjects were sedated intravenously with 2-10 mg midazolam. During the entire procedure vital signs, ECG, frequent blood pressure and O2 saturation monitoring was performed. Oxygen was delivered by nasal cannula up to 10 L/min as needed to maintain adequate oxygenation (O2 saturation >90%). A bronchoscope was inserted through nose and pharynx until the larynx was seen and vocal cords were anaesthetized by application of 1 mL 2% lidocain in triplicate. The trachea was passed and after inspection of the tracheobronchial tree the bronchoscope was guided to the right or left lower lobe and wedged at segments B8-B10. Afterwards, 3 aliquots of 20 mL saline were infused and subsequently retrieved gently by suction. The first aliquot was discarded, while the two other aliquots were mixed, prepared for analysis and consecutively snap frozen at -80º C. During BAL the bronchoalveolar tree was rinsed with 54th Plasma and BAL samples were analyzed for lefamulin concentrations using a validated and a partially validated LC-MS/MS method, respectively. The LLOQ was 1 ng/mL in both methods. RESULTS (cont‘d) Table 1. Mean pharmacokinetic parameters of lefamulin following a single oral dose of 150 mg AUC0-12 [ng·h/mL] Cmax [ng/mL] Plasma total 6022 ±1365 2576 ±492 7.0 ± 1.1 NA Plasma free* 783 ±178 335 ±64 7.0 ± 1.1 NA 4489 932 NA 5.7 ELF t1/2 [h] Penetration rate * For plasma a free fraction of 13 % was used in the calculations. Figure 1. Unbound concentration – time profiles of lefamulin in plasma and ELF CONCLUSIONS PK parameters were calculated using a computer software package (SAS 9.1.3; SAS Institute,USA). Cmax, tmax, t½, AUC0-8h, and AUC0-12h were calculated from non-fitted data by employing the trapezoidal rule. For AUC0-inf, individual extrapolation based on the last observed concentration and the elimination constant kel was performed. Additionally, the apparent volume of distribution (Vd) was calculated for plasma. In ELF, tmax, Cmax, and AUC0-8h were calculated. In addition, to determine AUC0-12h in ELF C12h was calculated as well. C12h was estimated by use of the formula (C = C0h · e kel · t), where C represents the concentration at a defined time point, C0h is the last concentration measured, kel is the elimination rate constant and t is the time between the measurement of C0h and the defined time point. • Lefamulin was safe and well tolerated • Lefamulin showed rapid penetration into ELF after a single 150 mg one hour intravenous infusion • Therapeutic exposure levels of lefamulin in the lung are expected to be reached within the first day of treatment and are similar to the levels reached in blood plasma • Elimination from ELF followed the same time course as for plasma • The exposure levels seen in the ELF are encouraging for the use of lefamulin in the treatment of respiratory tract infections and will be used for target attainment analysis RESULTS • All subjects completed the study according to the protocol. • Lefamulin was safe and well tolerated. No serious adverse events were reported and all observed adverse events resolved spontaneously. There were no clinically relevant changes in laboratory values. • The mean area under the concentration-time curve (AUC0-12h) was 6022 ± 1365 ng·h/mL for the total and 783 178 ng·h/mL for the calculated free concentration in plasma following a single i.v. dose of 150 mg lefamulin. • Mean PK parameters are presented in Table 1. • AUC0-12h in the ELF was 4489 ng·h/mL, similar to the exposure of total drug in the blood plasma. • As shown in Figure 1 after an intravenous dose of 150 mg of lefamulin equilibration between the ELF and the total fraction in plasma occurred quickly. Thereafter, free concentration time profiles in ELF and plasma closely resemble each other, indicating very fast exchange of lefamulin within central compartment and interstitium. This finding is supported with the results from a QWBA study in rats where the concentrations measured in the majority of tissues, including the lung were high compared to the amounts measured in the circulating blood.[3]. • The penetration ratio of lefamulin into ELF compared to free drug in plasma was 5.7 (Table 1). • Approximately 1 h after end of infusion the lefamulin levels in ELF reached equilibrium with the total plasma levels. • Elimination from ELF followed the same time course as for plasma with a similar t1/2. • A high volume of distribution of 215 L reflected the fast and good penetration into tissues. Interscience Conference on Antimicrobial Agents and Chemotherapy, September 5-9, 2014 | Washington, DC REFERENCES [1] Kikuchi J, Yamazaki K, Kikuchi E, Ishizaka A, Nishimura M. Pharmacokinetics of gatifloxacin after a single oral dose in healthy young adult subjects and adult patients with chronic bronchitis, with a comparison of drug concentrations obtained by bronchoscopic microsampling and bronchoalveolar lavage. Clin Ther 2007; 29(1): p. 123-30. [2] Rennard SI, Basset G, Lecossier D, et al. Estimation of volume of epithelial lining fluid recovered by lavage using urea as marker of dilution. J Applied Physiol 1986; 60(2): p. 532-8. [3] Wicha WW, Ivezic-Schoenfeld Z, Novak R. Pharmacokinetic, Mass Balance and Tissue Distribution of [14C]-BC-3781 in Non-pigmented Rats. Poster P909. 2010. 20th ECCMID, Vienna, Austria.