Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
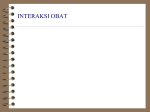
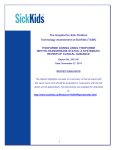
Research Article For reprint orders, please contact: [email protected] Are patients with intermediate TPMT activity at increased risk of myelosuppression when taking thiopurine medications? Thiopurine S-methyltransferase (TPMT) metabolizes thiopurine medications, including azathioprine and 6-mercaptopurine. Absent TPMT activity (i.e., in individuals homozygous for a variant TPMT allele) is associated with an increased risk of myelosuppression in patients taking thiopurine drugs. However, it is not clear if there is also an increased risk for patients with intermediate TPMT activity (i.e., in individuals heterozygous for a variant TPMT allele). Aims: To quantify the increased risk of myelosuppression for patients with intermediate TPMT activity. Materials & methods: A systematic review identified published studies, up to 29 September 2008, that explored the relationship between TMPT and hematological adverse drug reactions to thiopurines. Following a critical appraisal of the quality of published studies, a metaanalysis calculated the odds ratio of myelosuppression for patients with intermediate TPMT activity compared with wild-type. Results: A total of 67 studies were identified, the majority retrospective cohort in design. Patients with two TPMT variant alleles who are TPMT deficient have a substantial increase in their risk of myelotoxicity (86% of deficient patients developed myelosuppression). The increase in odds ratio of developing leukopenia for patients with intermediate TPMT activity or one TPMT variant allele compared with wild-type was 4.19 (95% CI: 3.20–5.48). Conclusion: This meta-analysis suggests that individuals with both intermediate and absent TPMT activity have an increased risk of developing thiopurine-induced myelosuppression, compared with individuals with normal activity. However, there is significant variability in the quality of the reported studies and large prospective studies to clarify the size of the effect of TPMT variant alleles on the risk of myelosuppression should be conducted. Accurate risk assessments will provide important data to inform clinical guidelines. KEYWORDS: adverse drug reaction n azathioprine n myelosuppression n pharmacogenetics n pharmacogenomics n thiopurine n TPMT Deficiency of the drug-metabolism enzyme thiopurine S-methyltransferase (TPMT) was first described nearly 30 years ago [1] . Approximately one in 300 individuals were found to be deficient in the enzyme, with a further one in ten having intermediate activity. Subsequent studies established a close correlation between red blood cell TPMT activity and 6-thioguanine nucleotide levels in patients treated with thiopurine medications [2] . Nearly 10 years after its initial description, a relationship between absent TPMT activity and thiopurine-induced myelotoxicity was established [3] . Numerous case reports supported the association between profound neutropenia and TPMT deficiency in individuals treated with standard doses of thiopurine drugs [4–6] . Although these were only isolated reports, the use of azathioprine and 6-mercaptopurine to treat a growing number of conditions, including inflammatory bowel disease, rheumatoid arthritis, systemic lupus, immunobullous disease, generalized eczematous disorders and acute lymphoblastic leukemia, meant that not identifying TPMT deficiency could have wide implications. TPMT deficiency is generally associated with early and more severe myelo toxicity [7] . Conversely, high TPMT activity may be associated with a poor response to treatment, with patients requiring higher doses to achieve a therapeutic effect [8] . Thiopurine S-methyltransferase activity can be analyzed either through an enzyme assay (conversion of 6-mercaptopurine to radiolabeled 6-methyl mercaptopurine in red cell lysate) or by analysis of common genetic polymorphisms (e.g., TPMT*2, TPMT*3A or TPMT*3C ). Measurement of TPMT activity using either the phenotypic or genetic test was adopted by some clinicians prior to azathioprine use [9,10] . Uptake of TPMT testing in the UK and across Europe was initially slow, as reservations regarding sensitivity and specificity, cost, test availability, turnaround time and results interpretation outweighed the evidence of clinical utility [11,12] . TPMT deficiency only accounts for a quarter of all cases of myelosuppression on thiopurine treatment [13] , and a number of other adverse reactions associated with thiopurine use, 10.2217/PGS.09.155 © 2010 Future Medicine Ltd Pharmacogenomics (2010) 11(2), 177–188 Jenny E Higgs1, Katherine Payne2, Chris Roberts2 & William G Newman1,3† Author for correspondence: Central Manchester & Manchester Children’s University Hospitals NHS Trust, Manchester Royal Infirmary, Manchester, UK 2 Health Methodology Research Group, The University of Manchester, Manchester, UK 3 Department of Medical Genetics, St Mary’s Hospital, Manchester Academic Health Sciences Centre (MAHSC), The University of Manchester, Manchester, M13 9WL, UK Tel.: +44 161 276 6264 Fax: 44 161 276 6145 william.newman@ manchester.ac.uk † 1 part of ISSN 1462-2416 177 Research Article Higgs, Payne, Roberts & Newman including allergic reactions, hepatotoxicity, pancreatitis, nausea and vomiting, cannot be predicted by TPMT testing. A review has been carried out defining the risk of myelosuppression for patients on thiopurine medication for inflammatory bowel disease [7] . This review does not address whether there is an increased risk of myelosuppression associated with intermediate TPMT enzyme activity. An early study by Black et al. identified that five out of six individuals who stopped azathioprine owing to leukopenia were heterozygous for a TPMT variant [14] . Other studies have also indicated an increased risk in individuals with intermediate TPMT activity [15,16] , which is counterbalanced by increased efficacy in this subset [15] . Guidelines drawn up by the British Society of Gastroenterology regarding the use of azathioprine and the related monitoring of patients have not necessarily advocated TPMT testing [17] . However, recent guidelines in rheumatology and dermatology have been more forthright in recommending TPMT testing as part of the management of patients who are due to commence azathioprine therapy [18,19] . This has mirrored an exponential increase in the uptake of TPMT testing in the UK [12] . These recommendations were made based on “evidence obtained from expert committee reports or opinions, and/or clinical experience of respected authorities… [with] an absence of directly applicable studies of good quality” [18] . Although numerous small studies have been carried out testing TPMT activity and/or genotype, the effect of intermediate TPMT activity on thiopurine-induced myelosuppression is uncertain. There is an unmet need for a systematic review of the risks of myelosuppression associated with intermediate TPMT activity, and we present a meta-analysis of the published literature. Materials & methods The primary aim of this systematic review was to identify all studies that observed hematological adverse reactions to a thiopurine medication and tested for TPMT activity or genotype. This was to allow assessment of the quality of the studies and their contribution to the evidence base for TPMT testing. The secondary aim was to quantify the level of any increased risk of myelosuppression as a result of intermediate TPMT activity. The systematic review was conducted by following the guidelines described by Cochrane to identify published studies [101] . The focus of the review was to explore the relationship between TPMT and hematological adverse drug reactions to azathioprine in published literature. For the 178 Pharmacogenomics (2010) 11(2) purpose of this review, the definitions shown in Table 1 were adopted for the key adverse drug reactions and descriptors of the level of TPMT activity. It should be noted that the studies used different methods for testing TPMT activity and, therefore, reported their results in different units. Search strategy Searches strategies were designed for OVID MEDLINE, EMBASE, Cumulative Index to Nursing and Allied Health Literature (CINAHL), The Cochrane library, Web of Knowledge, and PsycINFO using appropriate MeSH headings (Online Supplementary Appendix 1; www.futuremedicine. com/doi/suppl/10.2217/pgs.09.155/suppl_file/ suppl_material.xls). The search was run from 1978 to 29 September 2008. This start year was selected because this was the year that the TPMT enzyme was identified [19] . The key words in the search strategy included terms relevant to TPMT and thiopurines, for example, ‘azathioprine’ or ‘6-mercaptopurine’, and hematological events. In addition, references in review articles and the bibliographies of identified studies were examined for further potentially relevant studies. Although reviews were not included in the systematic review, their references were checked for relevant studies. Study selection Abstracts were checked for relevance to the topic of the review against predefined inclusion and exclusion criteria independently by two reviewers (JE Higgs and WG Newman). Disagreements were resolved by discussion with a third party, if necessary. Full text articles of the relevant abstracts were then obtained and assessed for relevance by two reviewers (JE Higgs and WG Newman). Inclusion criteria The following inclusion criteria were used for this review: all primary studies of patients on a thiopurine medication that tested for TPMT, either the genotype or phenotype, and reported cases of hematological adverse reactions. The search was not limited to a specific disease or condition. Expert opinion supported by a preliminary literature review indicated that there was likely to be very few randomized, controlled trials (RCTs) on this topic; therefore, any study design was included in the review. A second set of inclusion criteria were then used to assess whether the identified studies would be included in the subsequent meta-analysis. Two criteria were used: availability of data on the number of cases of myelosuppression for each level of TPMT activity; and adequate study quality. future science group TPMT activity & myelosuppression when taking thiopurine medications Research Article Table 1. Hematological definitions. Hematological term Definition Myelosuppression/myelotoxicity/ bone marrow suppression Myelotoxicity* Severe myelotoxicity* A decrease in bone marrow activity Leukopenia Neutropenia‡ Thrombocytopenia§ TPMT activity definitions¶ High/normal TPMT activity Intermediate TPMT activity Low TPMT activity Mild leukopenia: leukocyte count of between 3 and 4 × 109 /l Severe leukopenia: leukocyte count of <2.5–2 × 109 /l or leukopenia requiring hospitalization A decrease in the number of white blood cells (leukocytes) Definitions in the literature reviewed ranged from a leukocyte count of <1x109 /l to <4 × 109 /l A decrease in the number of neutrophils, defined in the literature reviewed as a neutrophil count of <1 × 109 /l to <2.5 × 109 /l A decrease in the number of platelets, defined as <100 × 109 /l >13.7 units/mlRBC Between 5 and 13.7 units/mlRBC <5 units/mlRBC *Definitions from [7]. ‡ Reported by eight studies [24,25,27,29,30,73,74,75]. § Reported by two studies [25,76]. ¶ There was variation in the units used. The most commonly used range is shown [26,29,31,32,77,78]. RBC: Red blood cell; TMPT: Thiopurine S-methyltransferase. Exclusion criteria Studies were excluded if they did not test TPMT genotype or phenotype (e.g., TPMT metabolite monitoring) or did not report hematological adverse reactions. This study focused on primary studies and excluded all reviews. Case studies were excluded as they provided limited new data. Studies published in only abstract form were excluded as they did not provide enough information regarding results and study quality. Non‑English and nonhuman articles were excluded. A study was excluded from the meta-analysis if the sample included only patients that had been selected for TPMT testing because they had experienced a hematological adverse drug reaction. This is because it is not possible to calculate an odds ratio of myelosuppression using data from these studies. Quality-assessment strategy All studies were quality assessed using published guidelines specifically designed to assess the quality of pharmacogenetic studies ( Online Supplementary Table 1; www.futuremedicine.com/ doi/suppl/10.2217/pgs.09.155/suppl_file/suppl_ material.xls) [20] . Data-extraction strategy The key purpose of the data-extraction strategy was to summarize the studies in terms of their design. To conduct the meta-analysis and calculate the odds ratio for the risk of myelosuppression in TPMT heterozygotes or intermediate activity, the following data were extracted; number future science group of patients that were wild-type for TPMT with and without a hematological event; and TPMT heterozygous or intermediate activity with and without a hematological event. If this information was not reported explicitly in the study, it was excluded from the meta-analysis. Data analysis The data from the systematic review and the assessment of study quality were reported as a narrative review. The number of patients with and without TPMT heterozygosity and/or intermediate activity and with and without myelosuppression was tabulated (Online Supplementary Table 2; www.futuremedicine.com/doi/suppl/10.2217/ pgs.09.155/suppl_file/suppl_material.xls). In some categories, there were no patients, and these were labeled ‘zero-cells’. A meta-analysis using the Mantel Haenszel (MH) pooled odds ratio without the zero-cell correction was used to quantify the risk of myelosuppression in TPMT heterozygotes or intermediate activity [21,22] . Two sensitivity analyses were carried out to compare estimates of the odds ratio by including and then excluding zero-cells and study design, classified as case–control prospective cohort and retrospective cohort. Between-study heterogeneity was investigated by estimation of the I2 statistic, the betweenstudy variance t2, and a c2 test of heterogeneity. The heterogeneity statistic I2 is interpreted as the percentage of variability due to heterogeneity between studies rather than sampling error. High I2 values indicate increasing heterogeneity. Rucker www.futuremedicine.com 179 Research Article Higgs, Payne, Roberts & Newman et al. show that I2 increases with the number of patients included in the meta-analysis and suggest using estimates of heterogeneity variance t2 ; therefore, t2 was calculated in addition to I2 [23] . A number needed to test (NNT) was estimated from the pooled odds ratio and the proportion of subjects in the control group suffering an event [102] . This was assumed to be 7% using data from the current study ( Online Supplementary Table 2; www.futuremedicine.com/ doi/suppl/10.2217/pgs.09.155/suppl_file/suppl_ material.xls) and Gisbert and Gomollon [7] . Results Study selection The search strategy identified 725 studies. 67 studies were selected for inclusion in the systematic review. Figure 1 summarizes reasons for exclusion from the systematic review. The list of excluded studies is available from the corresponding author on request. A further two studies were identified by searching the references of review articles [24,25], which were e-publications ahead of print and, therefore, not in the OVID/EMBASE databases at the time of searching (29 September 2008). O nline Supplementary Tables 3 & 4 & R eference L ist (www.futuremedicine.com/doi/suppl/10.2217/ pgs.09.155/suppl_file/suppl_material.xls)����� summarize the main characteristics of the studies included. Sample sizes ranged from 19 to 667 patients. The systematic review and meta-analysis included two case–control trials, 11 cohort prospective studies and 34 cohort retrospective studies. Included in the systematic review, but not the meta-analysis were two RCTs, two case–control trials, five cohort prospective studies and 11 cohort retrospective studies. The follow-up time of the studies varied from 4 weeks to 14 years (mean: 2.5 years; median: 6 months). Thiopurine drugs and doses varied between and within studies. Azathioprine was used in the majority of studies (n = 52), and 6-mercaptopurine was used in 15 studies. There was a consistent relationship between very low or absent TPMT activity or carriage of two TPMT variant alleles and myelosuppression. Of the 43 patients identified with two TPMT variant alleles or low/absent TPMT activity (Online Supplementary Table 4; www.futuremedicine. com/doi/suppl/10.2217/pgs.09.155/suppl_file/ suppl_material.xls), 37 (86%) patients developed severe myelosuppression. Most studies had sample sizes of fewer than 100 patients. The two largest prospective studies, with sample sizes of 394 [26] and 207 [24] , both concluded that intermediate TPMT activity was 180 Pharmacogenomics (2010) 11(2) a risk factor for myelosuppression. Gisbert et al. reported that inflammatory bowel disease patients with intermediate TPMT activity had four-times more chance of developing myelosuppression than individuals with normal TPMT activity [26] . Ansari et al. followed 207 inflammatory bowel disease patients, who were started on 2 mg/kg of azathioprine, for 6 months [24] . They reported that TPMT heterozygotes were more likely to suffer from gastric intolerance and myelosuppression than wild-type patients. In the 67 studies, 655 cases of myelosuppression were reported. It was possible to assign a phenotype or genotype to 492 of these; 37 (7.5%) were TPMT variant homozygotes, compound heterozygotes or had low TPMT activity; 118 (24%) were TPMT variant heterozygotes or had intermediate activity; and 337 (68.5%) were wild-type or had high/normal TPMT activity. A number of studies specifically selected myelosuppressed patients, which explains the higher frequencies of low and intermediate TPMT activity patients than reported in population studies [1] . These studies were excluded from the meta-analysis but not the systematic review. Importantly, different ranges of white cell counts were used to define leukopenia, varying from 1 × 109/l to less than 4 × 109/l (Table 1) , while 17 (25%) studies did not define leukopenia. Two RCTs have been carried out that measured TPMT and based the dose of azathioprine on the TPMT activity. However, Meggitt et al. compared azathioprine-adjusted doses with no azathioprine; therefore, it is not possible to determine if reducing the dose of azathioprine for patients with intermediate TPMT activity reduces the risk of myelosuppression [27] . The other RCT, while it did compare patients on standard doses and doses based on TPMT activity, had a sample size of only 29, and only one case of myelosuppression occurred [28] . Neither study could be used in the meta-analysis: Meggitt et al. did not provide the phenotypes for each patient [27] , and no intermediate-activity patients were present in the trial by Sayani et al. [28] . Meta-analysis A total of 47 studies were used in the metaanalysis [14,24,25,27,29–72] . Of the 20 studies excluded from the meta-analysis, this was generally because it was not possible to combine the data in a meta-analysis, as either all patients in the study were myelosuppressed, or the raw data required to calculate an odds ratio was not provided [3,13,15,16,26–28,31,73–84] . No studies were excluded because of poor methodological quality. future science group TPMT activity & myelosuppression when taking thiopurine medications Research Article Number of potentially relevant articles identified: 1122 from electronic search Duplicates: 397 Number of potentially relevant articles after removing duplicates: 725 Number of articles remaining: 103 Number of articles excluded: 622 Not relevant to TPMT testing: 69 No comparison of TPMT test result with hematological adverse drug reactiosn to thiopurine treatment: 127 Not in English: 7 Nonhuman: 15 Review article, case report, letter, editorial or not full text: 404 Full text retrieved Identified through searching bibliographies: 2 Number of articles remaining: 65 Number of articles excluded: 38 No TPMT testing: 6 No comparison of TPMT test result with hematological adverse drug reactions to thiopurine treatment: 24 Same patients as in a previous study: 4 Not in English: 2 Comment/editorial material, case study: 2 Total articles for systematic review: 67 Number of articles excluded from meta-analysis: 20 All patients in the study myelosuppressed: 2 Data required to calculate an odds ratio not provided: 18 Total articles for meta-analysis: 47 Figure 1. Study selection. TPMT: Thiopurine S-methyltransferase. Two (4%) of the 47 studies included in the meta-analysis were case–control designs (150 patients), 11 (23%) studies were prospective cohort studies (834 patients), and the remaining 34 studies (72%) were retrospective cohorts (3322 patients). Ten studies had no cases of myelosuppression among TPMT variant heterozygotes/ intermediate-activity subjects. In all studies, some wild-type subjects were event free (i.e., there were no myelosuppression cases). Sensitivity analysis demonstrated that the odds ratio is similar for each study design, whether zero-cells are included or not (Table 2) . The summary odds ratio for leukopenia in intermediate TPMT activity or hetero zygote TPMT variant allele patients compared with wild-type was 4.19 (95% CI: 3.20–5.48). A c2 test of heterogeneity suggested there was heterogeneity between studies (p = 0.001) and the I2 was 44.2%, which also indicated that the studies were heterogeneous. Pooling studies with an I2 of less than 50% has been suggested as acceptable, as values of greater than 50% indicate substantial heterogeneity [101] . The magnitude of I2 statistic may be inflated by the large number of patients future science group included in this meta-analysis (n = 4306) [23] . The number of studies that cross one, indicating no statistically significant difference, on the Forest plot is 27 out of 47. However, most of the studies show an effect in the same direction (Figure 2) . Gisbert and Gomollon carried out a metaanalysis that estimated the incidence of myelo suppression to be 7% [7] . The data from the current study also estimate the frequency of myelosuppression in patients with normal TPMT activity to be 7% ( Online Supplementary Table 2; www.futuremedicine.com/doi/suppl/10.2217/ pgs.09.155/suppl_file/suppl_material.xls). If 7% is used as the baseline risk in order to calculate the NNT to detect one patient at risk of leukopenia, the NNT is six. Quality assessment Quality-assessment tables are shown in full in Online Supplementary Tables 1, 5–7 (��������������� www.futuremedicine.com/doi/suppl/10.2217/pgs.09.155/suppl_ file/suppl_material.xls). The majority of studies described their aims, outcomes and interventions, as well as patient characteristics. www.futuremedicine.com 181 Research Article Higgs, Payne, Roberts & Newman Table 2. Sensitivity analyses. Study design Case–control Prospective cohort studies Prospective cohort studies* Retrospective cohort studies Retrospective cohort studies* Overall Mantel Haenszel odds ratio 95% CI 13.27 4.30 3.37 4.07 3.99 4.19 1.64–107.69 2.53–7.29 1.90–6.01 2.97–5.58 2.73–5.82 3.20–5.48 p-value Studies (n) Variance t I2 (%) p-value 0.016 <0.0001 <0.0001 <0.0001 <0.0001 <0.0001 1.48 0.94 0.91 0.64 0.95 56.4 48.6 43.1 43.2 44.2 0.011 0.049 0.005 0.024 0.001 2 11 9 34 19 47 Heterogeneity 2 *Excluding studies with a zero cell. The recruited patients and study sites were representative of the patient population and normal treatment facilities. Randomization and blinding of patients was carried out by the two RCTs only, although more studies blinded assessors (14 out of 67, 21%). Compliance was considered adequate by all studies, although only two studies formally measured compliance [74,53] . The reporting of results was variable, and 30 out of 67 (45%) studies did not give their full results and used averages or gave statistics without presenting raw data. When used, p-values were often rounded up (17 out of 57 cases [30%]), rather than reported as absolute values. The quality of the pharmacogenetic study design was assessed using the Jorgensen and Williamson criteria [20] . The reporting of methods and Hardy–Weinberg equilibrium (HWE) could be improved. The lack of power calculations (45 out of 67 [67%] cases) reflects that the majority of retrospective, cohort studies did not perform a power calculation. Most studies that performed a genetic test (n = 48) carried out a literature review (81%) that included reasons for choosing the SNPs genotyped (30 out of 48 [63%]). In all cases, they selected the common SNPs associated with low TPMT enzyme activity based on the current literature. The mode of inheritance of TPMT was explicitly stated in 45 (67%) out of 67 studies. None of the studies described a sample size calculation or a priori defined the power to detect effect sizes or checked for the presence of population stratification. Two of the four case–control studies clearly defined the patient groups, but none genotyped the cases and controls in mixed batches. The genotype and/or phenotype tests were described by 57 of the 67 (85%) studies. Quality-control measures were described by only six (9%) studies, and of these, four reported their findings. Independent checking of results was not described by any study. Blinding of assessors was described by 14 (21%) studies. 182 Pharmacogenomics (2010) 11(2) Two of the studies reported on noncompliance, and each withdrew those patients whose TPMT metabolite levels indicated nonadherence with the prescribed dose and medication [74,52] . Of the 48 studies carrying out a genotype test, only five (10%) checked for HWE. Two of the studies reported using the c2 test to measure HWE and one study used a software package [103] . The remaining two studies did not report the method used. None of the studies found deviation from HWE, but none of the studies reported the statistical results or the p-values. One study reported these details as online supplementary data. Outcomes were justified and fully reported by all the studies. The outcomes were defined in 51 (76%) of the studies. Missing data were not mentioned by any of the studies reviewed. A relatively small number of SNPs were investigated; therefore, missing data should be minimal. Five additional quality assessment questions were asked that were specific to TPMT testing (Online Supplementary Tables 6 & 7; www.futuremedicine.com/doi/suppl/10.2217/pgs.09.155/ suppl_file/suppl_material.xls). The follow-up of the patients was 3 months (which is considered to be long enough to identify the majority of patients who will suffer a hematological adverse drug reaction to thiopurines [7]) or longer in 62 (93%) of the 67 studies. If using the phenotype test, patients should be tested before thiopurine use and at least 3 months after any blood transfusion. This was achieved by ten (27%) out of 37 of the studies, reflecting that the majority were retrospective in design. High, intermediate and low TPMT phenotypic activity was defined by 27 (73%) out of 37 studies. Several areas of heterogeneity have been explored with sensitivity analysis (e.g., ethnicity, disease studied, azathioprine rather than other thiopurine drug, leukopenia definition, if the study stated the mode of inheritance and defined outcomes, personnel blinding and number of alleles tested). Where more than five studies were combined, the odds ratio was between 3 and 9.1, future science group future science group www.futuremedicine.com Myelosuppression more likely with reduced TPMT activity Figure 2. Forest plot showing the odds ratio of myelosuppression for each study, separated by study design. OR: Odds ratio; TPMT: Thiopurine S-methyltransferase. Myelosuppression less likely with reduced TPMT activity 4.19 (3.20–5.48) Overall (I2 = 44.2%; p = 0.001) 12442 3.77 (0.15–95.82) 10.56 (0.61–183.37) 0.31 (0.01–7.05) 0.22 (0.01–4.15) 35.00 (1.63–750.31) 1.97 (0.08–49.80) 1.44 (0.42–4.95) 16.50 (0.86–315.19) 3.68 (1.08–12.50) 21.00 (0.74–598.29) 7.73 (1.24–48.39) 82.80 (8.27–828.68) 0.99 (0.28–3.47) 45.89 (2.02–1044.21) 8.60 (0.38–193.86) 1.92 (0.34–10.85) 19.00 (0.62–583.38) 3.46 (0.58–20.82) 0.85 (0.04–16.55) 3.51 (0.62–19.93) 7.47 (2.03–27.47) 9.46 (1.07–83.37) 3.00 (0.08–111.78) 43.00 (3.86–478.64) 88.20 (3.60–2160.37) 14.67 (1.00–215.31) 35.00 (6.36–192.63) 0.71 (0.04–14.15) 1.62 (0.07–35.63) 27.53 (1.28–592.93) 30.07 (0.97–932.78) 203.00 (7.60–5424.16) 0.88 (0.10–7.50) 4.31 (1.06–17.55) 4.07 (2.97–5.58) Cohort, retrospective Ando et al. (2001) Ansari et al. (2002) Bezier et al. (2008) Breen et al. (2005) Chocair et al. (1992) Corominas et al. (2003) Czaja et al. (2006) De Ridder et al. (2006) Fabre et al. (2004) Formea et al. (2004) Heckmann et al. (2005) Hibi et al. (2003) Hindorf et al. (2006b) Ishioka et al. (1999) Joji et al. (2003) Jun et al. (2005) Kader et al. (2000) Langley et al. (2002) McLeod et al. (1999) Naughton et al. (1999) Pandya et al. (2002) Schedel et al. (2006) Schutz et al. (1995) Schwab et al. (2002) Sebbag et al. (2000) Snow et al. (1995) Song et al. (2006) Stocco et al. (2005) Stocco et al. (2007) Taja-Chayeb et al. (2008) Tamori et al. (2007) Tumer et al. (2007) Winter et al. (2007) Zelinkova et al. (2006) Subtotal (I2 = 43.1%; p = 0.005) 1 33.21 (5.90–186.87) 451.00 (16.35–12441.78) 19.00 (1.15–314.97) 0.86 (0.10–7.60) 4.96 (0.46–53.24) 0.94 (0.16–5.45) 32.00 (1.96–522.76) 1.28 (0.23–7.19) 3.80 (1.16–12.46) 3.43 (0.19, 62.12) 3.89 (0.11–143.60) 4.30 (2.53–7.29) Cohort, prospective Ansari et al. (2008) Black et al. (1998) Derijks et al. (2004) Dubinsky et al. (2000) Gisbert et al. (2006a) Hawwa et al. (2008) Herrlinger et al. (2003) Hindorf et al. (2006a) Kurzawski et al. (2005) Stolk et al. (1998) Zhang et al. (2006) Subtotal (I2 = 56.4%; p = 0.011) 8.0 × 10 -5 36.60 (1.37–978.57) 4.52 (0.15–132.83) 13.27 (1.63–107.69) OR (95% CI) Case–control Gearry et al. (2003) Reuther et al. (2004) Subtotal (I2 = 0.0%; p = 0.385) ID Study 100.00 1.11 0.40 4.25 7.16 0.36 1.02 10.09 0.26 5.04 0.28 1.11 0.29 11.74 0.28 0.80 3.80 0.22 2.27 2.39 2.31 3.25 1.58 0.63 0.21 0.19 0.51 0.50 2.73 1.27 0.44 0.08 0.06 4.43 2.92 73.99 0.64 0.05 0.40 4.35 0.87 6.18 0.26 5.17 5.92 1.01 0.51 25.36 0.18 0.47 0.65 Weight (%) TPMT activity & myelosuppression when taking thiopurine medications Research Article 183 Research Article Higgs, Payne, Roberts & Newman with increased variability when fewer studies were combined (Online Supplementary Table 8; www.futuremedicine.com/doi/suppl/10.2217/pgs.09.155/ suppl_file/suppl_material.xls). The I2 value is not reduced by grouping the studies in this way, remaining 40–50%. Publication bias was explored using a funnel plot. This shows evidence of publication bias, in that small studies that do not show an increased rate of myelosuppression in patients with inter mediate TPMT activity are under-represented (Online Supplementary Figure 1; www.futuremedicine. com/doi/suppl/10.2217/pgs.09.155/suppl_file/ suppl_material.xls). Discussion This study provides systematically collated evidence that low and/or absent TPMT activity results in severe myelosuppression in individuals treated with standard doses of thiopurines. It has been this association that has driven forward the adoption of TPMT testing into clinical practice to identify individuals deficient in TPMT and avoid this serious adverse drug reaction. More controversial has been the relationship between thiopurine-associated hematological adverse reactions in individuals with intermediate enzyme activity. Our meta-analysis demonstrates a fourfold raised risk of leukopenia in patients with one TPMT variant or intermediate activity. Owing to the heterogeneity of the studies used in the metaanalysis, the raised odds ratio should be interpreted with caution. The range of white cell counts used to define leukopenia varied. Importantly, the increased risk was of mild leukopenia rather than severe leukopenia, neutropenia or infection. Furthermore, lymphopenia is a normal response to thiopurine immunosuppression [66] . Individuals with higher levels of thiopurine active metabolites are more likely to be lymphopenic [85] , and individuals with intermediate TPMT activity have raised levels of active metabolites [86] . Therefore, modest leukopenia may reflect effective treatment with thiopurines, rather than a clinically relevant adverse event. Some authors have argued that identification of individuals with intermediate TPMT activity would allow reduced doses of thiopurine to achieve effective immunosuppression, and careful early monitoring to reduce the likelihood of myelosuppression [87] . Whether knowledge of TPMT status and the potential for improved care for patients with intermediate TPMT activity is cost effective has not been established. A key challenge for this study was how to identify studies that included descriptions of TPMT-associated adverse drug reactions because 184 Pharmacogenomics (2010) 11(2) a variety of different terms were used to refer to ADRs and myelosuppression. To address this issue, the search terms were made as comprehensive as possible, and many words for adverse drug reaction and myelosuppression were used in the search strategy (Online Supplementary A ppendix 1; www.futuremedicine.com/doi/suppl/10.2217/ pgs.09.155/suppl_file/suppl_material.xls). There are a number of sources of methodo logical and clinical heterogeneity in the studies selected for this review, which may account for the statistical heterogeneity. Most of the studies were small, and, in theory, combining their data should give a more precise result. Although the varying quality of methods and reporting of the studies contributes to methodological hetero geneity, the studies included in the meta-analysis were of a similar methodological standard without obvious factors that would lead to an exaggerated or reduced measure of the effect of TPMT activity on myelosuppression. Important sources of clinical heterogeneity include the definitions of leukopenia, length of follow-up, TPMT testing methods, specific thiopurine drug and dose. Gisbert and Gomollon showed that bone marrow suppression can occur at any time after commencing treatment [7] . Although it occurs most commonly within the first few months, studies with shorter follow-up time may miss some cases of myelosuppression and underestimate the effect of TPMT status, reducing the measured effect of TPMT activity. Side effects, including nausea, may cause patients to discontinue thiopurine treatment before myelosuppression occurs, again reducing the effect of TPMT activity. However, there is no evidence that patients who suffer from other side effects have an increased incidence of myelosuppression. The number of alleles tested varied between studies. Some studies sequenced TPMT and were, therefore, likely to detect all functional TPMT variants, while others tested for the three most common variant alleles only, which may lead to underestimation of the effect of TPMT on myelosuppression. Conversely, myelosuppression has a number of causes that are independent of TPMT in individuals taking thiopurines; that is, other immunosuppressants, viral (e.g., cytomegalovirus) and antithymocyte globulin in transplant patients, the underlying disease and idiosyncratic reactions [13] . There are several sources of variability associated with the tests used for TPMT activity. The studies used a number of different phenotypic tests, and consequently, the units for TPMT activity varied between studies; therefore, future science group TPMT activity & myelosuppression when taking thiopurine medications direct comparison of values is not possible and patients are allocated into high-, intermediateand low-activity groups in order to compare the studies. This classification is set at an arbitrary cutoff point defined by the individual studies, because the concordance between the genetic and phenotypic tests for TPMT is not 100% [88] . Although some studies found perfect concordance when carrying out genetic and phenotype tests [15,30,89] , many did not [16,33,52,53,71,90] . The concordance was as low as 77% in one study [33] . In addition, TPMT activity ranges differ between ethnic groups; notably, people of Afro-Caribbean ethnicity have lower TPMT activity than Caucasians and South Asians [91] . Variation in test methods and definitions will alter the sensitivity and specificity of TPMT testing in clinical practice. Although higher doses of azathioprine have not been shown to increase the incidence of myelosuppression [7] , this has not been analyzed specifically in patients with intermediate TPMT activity, and dose may be more important in this group, as intermediate TPMT activity may increase sensitivity to lower doses of thiopurines. Four studies excluded thiopurines or used a reduced thiopurine dose for low- or intermediateactivity/TPMT variant patients [29,27,41,53] . This may lead to less cases of myelosuppression than if standard doses had been used and therefore under-estimates of the odds ratio produced by the meta-analysis. A funnel plot indicated the presence of publication bias (Online Supplementary Figure 1; www.futuremedicine.com/doi/suppl/10.2217/pgs.09.155/ suppl_file/suppl_material.xls). However, analysis of the use of funnel plots suggests that there may be other reasons for this effect in addition to publication bias; for example, inherent differences in the design of small and large studies [92] . Conclusion Many studies have been conducted on the relationship between TPMT and hematological adverse reactions. This systematic review and Research Article meta-analysis supports the association between low-activity TPMT and a high risk of myelosuppression in individuals treated with standard doses of thiopurines. Individuals who are hetero zygous for TPMT variant alleles or patients with intermediate TPMT activity had a fourfold increased risk of leukopenia compared with wild-type. However, the clinical significance of moderate leukopenia is more difficult to interpret owing to the heterogeneity between studies. We recommend that further retrospective studies are unnecessary and unlikely to add to the evidence base. Prospective studies that evaluate the cost–effectiveness and utility of the test would be valuable. However, the use of TPMT testing has been accepted, and the test is cheap and routinely carried out. This study highlights that the increased risk of myelosuppression for intermediate-activity patients, while present, is low and should not preclude the use of thiopurine medications. Acknowledgements Thanks to Yenal Dundar, Specialty Registrar in Psychiatry, and Brian H Willis for comments on the search strategies. Financial & competing interests disclosure William G Newman’s group is supported through funding by the NIHR Manchester Biomedical Research Centre, MAHSC and through the Department of Health Pharmacogenetics Initiative (TARGET study) Ref. PHGX09A. Katherine Payne is funded by an RCUK aca� demic fellowship. �������������������������������������� The authors have no other relevant affili� ���� ations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. Ethical conduct of research The authors state that they have obtained appropriate insti tutional review board approval or have followed the princi ples outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved. Executive summary Patients with absent thiopurine S-methyltransferase (TPMT) activity have an increased risk of becoming profoundly myelosuppressed if given standard doses of thiopurine medications; for example, azathioprine. Patients with intermediate TPMT activity (or one variant allele) also have an increased risk of myelosuppression following standard thiopurine treatment; however, this is substantially less than homozygote/absent-activity individuals. The increased risk of leukopenia for individuals with intermediate TPMT activity compared with wild-type treated with thiopurines is fourfold. Mild leukopenia may reflect response to treatment rather than an adverse event. Prospective studies with well-defined and clinically significant end points (e.g., neutropenia and neutropenic sepsis) are required to accurately assess the increased risk for intermediate-activity patients. future science group www.futuremedicine.com 185 Research Article Higgs, Payne, Roberts & Newman Bibliography 11 Papers of special note have been highlighted as: n of interest nn of considerable interest 1 2 Weinshilboum RM, Sladek SL: Mercaptopurine pharmacogenetics: monogenic inheritance of erythrocyte thiopurine methyltransferase activity. Am. J. Hum. Genet. 32(5), 651–662 (1980). Lennard L, van Loon JA, Lilleyman JS, Weinshilboum RM: Thiopurine pharmacogenetics in leukemia: correlation of erythrocyte thiopurine methyltransferase activity and 6-thioguanine nucleotide concentrations. Clin. Pharmacol. Ther. 41(1), 18–25 (1987). 3 Lennard L, van Loon JA, Weinshilboum RM: Pharmacogenetics of acute azathioprine toxicity: relationship to thiopurine methyltransferase genetic polymorphism. Clin. Pharmacol.Ther. 46(2), 149–154 (1989). 4 Lennard L, Gibson BE, Nicole T, Lilleyman JS: Congenital thiopurine methyltransferase deficiency and 6-mercaptopurine toxicity during treatment for acute lymphoblastic leukaemia. Arch. Dis. Child. 69, 577–579 (1993). 5 6 7 nn 8 9 10 Kerstens PJ, Stolk JN, De Abreu RA et al.: Azathioprine-related bone marrow toxicity and low activities of purine enzymes in patients with rheumatoid arthritis. Arthritis Rheum. 38(1), 142–145 (1995). Leipold G, Schütz E, Haas JP, Oellerich M: Azathioprine-induced severe pancytopenia due to a homozygous two-point mutation of the thiopurine methyltransferase gene in a patient with juvenile HLA-B27-associated spondylarthritis. Arthritis Rheum. 40, 1896–1898 (1997). Gisbert JP, Gomollon F: Thiopurine-induced myelotoxicity in patients with inflammatory bowel disease: a review. Am. J. Gastroenterol. 103(7), 1783–1800 (2008). Systematic review and meta-analysis of the incidence of thiopurine-induced myelotoxicity, infection and risk of death in inflammatory bowel disease patients. Dubinsky MC, Yang H, Hassard PV et al.: 6-MP metabolite profiles provide a biochemical explanation for 6-MP resistance in patients with inflammatory bowel disease. Gastroenterology 122, 904–915 (2002). Tan BB, Lear JT, Gawkrodger DJ, English JS: Azathioprine in dermatology: a survey of current practice in the U.K. Br. J. Dermatol. 136, 351–355 (1997). Holme SA, Duley JA, Sanderson J, Routledge PA, Anstey AV: Erythrocyte thiopurine methyl transferase assessment prior to azathioprine use in the UK. Q JM 95, 439–444 (2002). 186 de Boer NK, Mulder CJ, van Bodegraven AA: Impracticalities of thiopurine S-methyltransferase determination in daily inflammatory bowel disease practice. Aliment. Pharmacol. Ther. 23, 1278–1279 (2006). 23 Rücker G, Schwarzer G, Carpenter JR, Schumacher M: Undue reliance on I2 in assessing heterogeneity may mislead. BMC Med. Res. Method. 8, 79 (2008). 24 Ansari A, Arenas M, Greenfield S et al.: Prospective evaluation of the pharmacogenetics of azathioprine in the treatment of inflammatory bowel disease. Aliment. Pharmacol. Ther. 28(8), 973–983 (2008). 12 Newman W, Payne K: Removing barriers to a clinical pharmacogenetics service. Personalized Med. 5(5), 471–480 (2008). 13 Colombel JF, Ferrari N, Debuysere H et al.: 14 15 16 17 18 19 Genotypic analysis of thiopurine S-methyltransferase in patients with Crohn’s disease and severe myelosuppression during azathioprine therapy. Gastroenterology 118(6), 1025–1030 (2000). 25 Hawwa AF, Millership JS, Collier PS et al.: Black AJ, McLeod HL, Capell HA et al.: Thiopurine methyltransferase genotype predicts therapy-limiting severe toxicity from azathioprine. Ann. Intern. Med. 129(9), 716–718 (1998). 26 Gisbert JP, Nino P, Rodrigo L, Cara C, Relling MV, Hancock ML, Rivera GK et al.: Mercaptopurine therapy intolerance and heterozygosity at the thiopurine S-methyltransferase gene locus. J. Natl. Cancer Inst. 91, 2001–2008 (1999). Evans WE, Hon YY, Bomgaars L et al.: Preponderance of thiopurine S-methyltransferase deficiency and heterozygosity among patients intolerant to mercaptopurine or azathioprine. J. Clin. Oncol. 19(8), 2293–2301 (2001). Carter MJ, Lobo AJ, Travis SP, IBD Section BSoG: Guidelines for the management of inflammatory bowel disease in adults. Gut 53, V1–V16 (2004). Chakravarty K, McDonald H, Pullar T et al.: BSR/BHPR guideline for diseasemodifying anti-rheumatic drug (DMARD) therapy in consultation with the British Association of Dermatologists. Rheumatology (Oxford) 47, 924–925 (2008). Weinshilboum RM, Raymond FA, Pazmino PA: Human erythrocyte thiopurine methyltransferase: radiochemical microassay and biochemical properties. Clin. Chim. Acta. 85(3), 323–333 (1978). Pharmacogenomic studies of the anticancer and immunosuppressive thiopurines mercaptopurine and azathioprine. Br. J. Clin. Pharmacol. 66(4), 517–528 (2008). Guijarro LG: Thiopurine methyltransferase (TPMT) activity and adverse effects of azathioprine in inflammatory bowel disease: long-term follow-up study of 394 patients. Am. J. Gastroenterol. 101(12), 2769–2776 (2006). 27 Meggitt SJ, Gray JC, Reynolds NJ: Azathioprine dosed by thiopurine methyltransferase activity for moderate-tosevere atopic eczema: a double-blind, randomized controlled trial. Lancet 367, 839–846 (2006). 28 Sayani FA, Prosser C, Bailey RJ, Jacobs P, Fedorak RN: Thiopurine methyltransferase enzyme activity determination before treatment of inflammatory bowel disease with azathioprine: effect on cost and adverse events. Can. J. Gastroenterol. 19(3), 147–151 (2005). n 29 Gisbert JP, Luna M, Mate J et al.: Choice of azathioprine or 6-mercaptopurine dose based on thiopurine methyltransferase (TPMT) activity to avoid myelosuppression. A prospective study. Hepatogastroenterology. 53(69), 399–404 (2006). 30 Ansari A, Hassan C, Duley J et al.: 20 Jorgensen AL, Williamson PR: Thiopurine methyltransferase activity and the use of azathioprine in inflammatory bowel disease. Aliment. Pharmacol. Ther. 16(10), 1743–1750 (2002). Methodological quality of pharmacogenetic studies: Issues of concern. Stat. Med. 27, 6547–6569 (2008). 21 Bradburn M, Deeks J, Berlin J, Localio A: Much ado about nothing: a comparison of the performance of meta-analytical methods with rare events. Stat. Med. 26, 53–77 (2007). 22 Sweeting MJ, Sutton AJ, Lambert PC: What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparce data. Stat. Med. 23, 1351–1375 (2004). Pharmacogenomics (2010) 11(2) Although this study has a sample size of only 29, it is the only randomized, controlled trial reported to date that compares the effect of either determining thiopurine S-methyltransferase status prior to starting thiopurine treatment. 31 Langley PG, Underhill J, Tredger JM, Norris S, McFarlane IG: Thiopurine methyltransferase phenotype and genotype in relation to azathioprine therapy in autoimmune hepatitis. J. Hepatol. 37(4), 441–447 (2002). 32 Snow JL, Gibson LE: The role of genetic variation in thiopurine methyltransferase activity and the efficacy and/or side effects of azathioprine therapy in dermatologic patients. Arch. Dermatol. 131(2), 193–197 (1995). future science group TPMT activity & myelosuppression when taking thiopurine medications 33 Winter JW, Gaffney D, Shapiro D et al.: Assessment of thiopurine methyltransferase enzyme activity is superior to genotype in predicting myelosuppression following azathioprine therapy in patients with inflammatory bowel disease. Aliment. Pharmacol.Ther. 25(9), 1069–1077 (2007). 44 Kurzawski M, Dziewanowski K, Gawronska- Szklarz B, Domanski L, Drozdzik M: The impact of thiopurine S-methyltransferase polymorphism on azathioprine-induced myelotoxicity in renal transplant recipients. Ther. Drug. Monit. 27(4), 435–441 (2005). 45 34 Schwab M, Schaffeler E, Marx C et al.: Azathioprine therapy and adverse drug reactions in patients with inflammatory bowel disease: impact of thiopurine S-methyltransferase polymorphism. Pharmacogenetics 12(6), 429–436 (2002). 35 Czaja AJ, Carpenter HA: Thiopurine methyltransferase deficiency and azathioprine intolerance in autoimmune hepatitis. Dig.Dis.Sci. 51(5), 968–975 (2006). 36 De Ridder L, van Dieren JM, van Deventer Azathioprine toxicity and thiopurine methyltransferase genotype in renal transplant patients. Transpl. Proceed. 34(5), 1642–1645 (2002). 37 Derijks LJ, Gilissen LP, Engels LG et al.: 38 Dubinsky MC, Lamothe S, Yang HY et al.: 49 Stolk JN, Boerbooms AMT, De Abreu RA et al.: Reduced thiopurine methyltransferase activity and development of side effects of azathioprine treatment in patients with rheumatoid arthritis. Arthritis Rheum. 41(10), 1858–1866 (1998). Inosine triphosphate pyrophosphatase and thiopurine S-methyltransferase genotypes relationship to azathioprine-induced myelosuppression. Clin. Gastroenterol. Hepatol. 4(1), 44–49 (2006). 51 41 Herrlinger KR, Kreisel W, Schwab M et al.: 42 Jun JB, Cho DY, Kang C, Bae SC: Thiopurine S-methyltransferase polymorphisms and the relationship between the mutant alleles and the adverse effects in systemic lupus erythematosus patients taking azathioprine. Clin. Exp. Rheumatol. 23(6), 873–876 (2005). 43 Kader HA, Wenner WJ Jr, Telega GW, Maller ES, Baldassano RN: Normal thiopurine methyltransferase levels do not eliminate 6-mercaptopurine or azathioprine toxicity in children with inflammatory bowel disease. J. Clin. Gastroenterol. 30(4), 409–413 (2000). future science group 58 Formea CM, Myers-Huentelman H, Wu R et al.: Thiopurine S-methyltransferase genotype predicts azathioprine-induced myelotoxicity in kidney transplant recipients. Am. J. Transplant. 4(11), 1810–1817 (2004). 59 Gearry RB, Barclay ML, Burt MJ et al.: Thiopurine S-methyltransferase (TPMT ) genotype does not predict adverse drug reactions to thiopurine drugs in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 18, 395–400 (2003). 60 Ishioka S, Hiyama K, Sato H et al.: Thiopurine methyltransferase genotype and the toxicity of azathioprine in Japanese. Intern. Med. 38(12), 944–947 (1999). 61 50 Zelinkova Z, Derijks LJ, Stokkers PC et al.: 40 Hibi T, Naganuma M, Kitahora T, Kinjyo 6-thioguanine – efficacy and safety in chronic active Crohn’s disease. Aliment. Pharmacol. Ther. 17(4), 503–508 (2003). Is thiopurine methyltransferase genetic polymorphism a major factor for withdrawal of azathioprine in rheumatoid arthritis patients? Rheumatology 42(1), 40–45 (2003). and its clinical implication in renal transplant recipients with azathioprine treatment. J Clin. Pharm. Ther. 31(6), 627–635 (2006). 39 Fabre MA, Jones DC, Bunce M et al.: F, Shimoyama T: Low-dose azathioprine is effective and safe for maintenance of remission in patients with ulcerative colitis. J. Gastroenterol. 38(8), 740–746 (2003). 57 Corominas H, Domenech M, Laiz A et al.: 48 Song DK, Zhao J, Zhang LR: TPMT genotype Pharmacogenomics and metabolite measurement for 6-mercaptopurine therapy in inflammatory bowel disease. Gastroenterology 118(4), 705–713 (2000). The impact of thiopurine S-methyltransferase polymorphisms on azathioprine dose 1 year after renal transplantation. Transpl. Int. 17(9), 531–539 (2004). Cameron JS: The importance of thiopurine methyltransferase activity for the use of azathioprine in transplant recipients. Transplantation 53(5), 1051–1056 (1992). 47 Schedel J, Godde A, Schutz E et al.: Impact of thiopurine methyltransferase activity and 6-thioguanine nucleotide concentrations in patients with chronic inflammatory diseases. Ann. NY Acad. Sci. 1069, 477–491 (2006). 52 Heckmann JM, Lambson EM, Little F, Owen EP: Thiopurine methyltransferase (TPMT) heterozygosity and enzyme activity as predictive tests for the development of azathioprine-related adverse events. J. Neurol. Sci. 231(1–2), 71–80 (2005). Hindorf U, Lindqvist M, Hildebrand H, Fagerberg U, Almer S: Adverse events leading to modification of therapy in a large cohort of patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 24(2), 331–342 (2006). 54 Ando M, Ando Y, Hasegawa Y et al.: Genetic polymorphisms of thiopurine S-methyltransferase and 6-mercaptopurine toxicity in Japanese children with acute lymphoblastic leukaemia. Pharmacogenetics 11(3), 269–273 (2001). www.futuremedicine.com Joji N, Urosevi J, Boji B, Povlovi S: Determination of thiopurine methyltransferase genotype in the patients with inflammatory bowel disease before and during azathioprine therapy. Arch. Gastroenterohepatol. 22(1–2), 5–9 (2003). 62 McLeod HL, Coulthard S, Thomas AE et al.: Analysis of thiopurine methyltransferase variant alleles in childhood acute lymphoblastic leukaemia. Br. J. Haematol. 105(3), 696–700 (1999). 63 Reuther LO, Vainer B, Sonne J, Larsen NE: Thiopurine methyltransferase (TPMT ) genotype distribution in azathioprinetolerant and -intolerant patients with various disorders. The impact of TPMT genotyping in predicting toxicity. Eur. J. Clin. Pharmacol. 59(11), 797–801 (2004). 64 Schutz E, Gummert J, Mohr FW, Armstrong VW, Oellerich M: Azathioprine myelotoxicity related to elevated 6-thioguanine nucleotides in heart transplantation. Transplant Proc. 27(1), 1298–1300 (1995). 53 Hindorf U, Lindqvist M, Peterson C et al.: Pharmacogenetics during standardised initiation of thiopurine treatment in inflammatory bowel disease. Gut 55(10), 1423–1431 (2006). Bezier M, Reguiai Z, Vitry F, Broly F, Bernard P: Thiopurine S-methyltransferase genotypic analysis in autoimmune bullous diseases. Eur. J. Dermatol. 18(5), 512–517 (2008). 56 Chocair PR, Duley JA, Simmonds HA, 46 Pandya B, Thomson W, Poulton K et al.: HJ et al.: Pharmacogenetics of thiopurine therapy in paediatric IBD patients. Aliment. Pharmacol.Ther. 23(8), 1137–1141 (2006). Pharmacokinetics of 6-mercaptopurine in patients with inflammatory bowel disease: implications for therapy. Ther. Drug Monit. 26(3), 311–318 (2004). Naughton MA, Battaglia E, O’Brien S, Walport MJ, Botto M: Identification of thiopurine methyltransferase (TPMT ) polymorphisms cannot predict myelosuppression in systemic lupus erythematosus patients taking azathioprine. Rheumatology (Oxford) 38(7), 640–644 (1999). 55 Research Article 65 Sebbag L, Boucher P, Davelu P et al.: Thiopurine S-methyltransferase gene polymorphism is predictive of azathioprineinduced myelosuppression in heart transplant recipients. Transplantation 69(7), 1524–1527 (2000). 187 Research Article Higgs, Payne, Roberts & Newman 66 Stocco G, Martelossi S, Barabino A et al.: 76 Palmieri O, Latiano A, Bossa F et al.: Glutathione-S-transferase genotypes and the adverse effects of azathioprine in young patients with inflammatory bowel disease. Inflamm. Bowel Dis. 13(1), 57–64 (2007). Sequential evaluation of thiopurine methyltransferase, inosine triphosphate pyrophosphatase, and HPRT1 genes polymorphisms to explain thiopurines’ toxicity and efficacy. Aliment. Pharmacol. Ther. 26(5), 737–745 (2007). 67 Taja-Chayeb L, Vidal-Millan S, Gutierrez O et al.: Thiopurine S-methyltransferase gene (TMPT ) polymorphisms in a Mexican population of healthy individuals and leukemic patients. Med. Oncol. 25(1), 56–62 (2008). 78 Banerjee S, Bishop WP: Evolution of 72 Stocco G, Martelossi S, Barabino A et al.: TPMT genotype and the use of thiopurines in paediatric inflammatory bowel disease. Dig. Liver Dis. 37(12), 940–945 (2005). 73 Marinaki AM, Ansari A, Duley JA et al.: Adverse drug reactions to azathioprine therapy are associated with polymorphism in the gene encoding inosine triphosphate pyrophosphatase (ITPase). Pharmacogenetics 14(3), 181–187 (2004). 74 Rumbo C, Emerick KM, Emre S, Shneider BL: Azathioprine metabolite measurements in the treatment of autoimmune hepatitis in pediatric patients: a preliminary report. J. Pediatr. Gastroenterol. Nutr. 35(3), 391–398 (2002). 75 Campbell S, Kingstone K, Ghosh S: Relevance of thiopurine methyltransferase activity in inflammatory bowel disease patients maintained on low-dose azathioprine. Aliment. Pharmacol. Ther. 16(3), 389–398 (2002). 188 88 Schaeffeler E, Fischer C, Brockmeier D et al.: Comprehensive analysis of thiopurine S-methyltransferase phenotype-genotype correlation in a large population of German-Caucasians and identification of novel TPMT variants. Pharmacogenetics. 14, 407–417 (2004). 79 Dokmanovic L, Urosevic J, Janic D et al.: Analysis of thiopurine S-methyltransferase polymorphism in the population of Serbia and Montenegro and mercaptopurine therapy tolerance in childhood acute lymphoblastic leukemia. Ther. Drug Monit. 28(6), 800–806 (2006). 89 Hindorf U, Peterson C, Almer S: Assessment of thiopurine methyltransferase and metabolite formation during thiopurine therapy: results from a large Swedish patient population. Ther. Drug Monit. 26, 673–678 (2004). 80 Pettersson B, Almer S, Albertioni F, Söderhäll S, Peterson C: Differences between children and adults in thiopurine methyltransferase activity and metabolite formation during thiopurine therapy: possible role of concomitant methotrexate. Ther. Drug Monit. 24, 351–358 (2002). 71 Breen DP, Marinaki AM, Arenas M, Hayes PC: Pharmacogenetic association with adverse drug reactions to azathioprine immunosuppressive therapy following liver transplantation. Liver Transpl. 11(7), 826–833 (2005). Barclay ML: Thiopurine dose in intermediate and normal metabolizers of thiopurine methyltransferase may differ three-fold. Clin. Gastroenterol. Hepatol. 6, 654–660 (2008). thiopurine use in pediatric inflammatory bowel disease in an academic center. J. Pediatr. Gastroenterol. Nutr. 43(3), 324–330 (2006). 70 Zhang B, Xu X, Zeng X, Li D: Correlation of thiopurine methyltransferase activity and 6-thioguanine nucleotide concentration in Han Chinese patients treated with azathioprine 25 to 100 mg: a 1‑year, single-center, prospective study. Curr.Ther Res. 67(4), 270–282 (2006). 87 Gardiner SJ, Gearry RB, Begg EJ, Zhang M, Measurement of thiopurine methyltransferase activity and azathioprine metabolites in patients with inflammatory bowel disease. Gut 49(5), 665–670 (2001). 69 Tumer TB, Ulusoy G, Adali O et al.: The low frequency of defective TPMT alleles in Turkish population: a study on pediatric patients with acute lymphoblastic leukemia. Am. J. Hematol. 82(10), 906–910 (2007). of thiopurine methyltransferase and metabolite formation during thiopurine therapy: results from a large Swedish patient population. Ther. Drug Monit. 26, 673–678 (2004). 77 Lowry PW, Franklin CL, Weaver AL et al.: 68 Tamori A, Shinzaki M, Kosaka S et al.: Thiopurine S-methyltransferase gene polymorphism in Japanese patients with autoimmune liver diseases. Liver Int. 27(1), 95–100 (2007). 86 Hindorf U, Peterson C, Almer S: Assessment 81 Shah JA, Edwards CM, Probert CS: Should azathioprine and 5-aminosalicylates be coprescribed in inflammatory bowel disease?: An audit of adverse events and outcome. Eur. J. Gastroenterol. Hepatol. 20(3), 169–173 (2008). 82 Hindorf U, Lyrenäs E, Nilsson A, Schmiegelow K: Monitoring of long-term thiopurine therapy among adults with inflammatory bowel disease. Scand. J. Gastroenterol. 39(11), 1105–1112 (2004). 83 Lindqvist M, Hindorf U, Almer S et al.: No induction of thiopurine methyltransferase during thiopurine treatment in inflammatory bowel disease. Nucleos. Nucleot. Nucl. Acids. 25(9–11), 1033–1037 (2006). 84 Okada Y, Nakamura K, Kodama T et al.: Thiopurine methyltransferase genotype and phenotype status in Japanese patients with systemic lupus erythematosus. Biol. Pharm. Bull. 28(11), 2117–2119 (2005). 85 Aberra FN, Lichtenstein GR: Review article: 90 Heneghan MA, Allan ML, Bornstein JD, Muir AJ, Tendler DA: Utility of thiopurine methyltransferase genotyping and phenotypeing, and measurement of azathioprine metabolites in the management of patients with autoimmune hepatitis. J. Hepatol. 45, 584–591 (2006). 91 Cooper SC, Ford LT, Berg JD, Lewis MJ: Ethnic variation of thiopurine S-methyltransferase activity: a large, prospective population study. Pharmacogenomics 9(3), 303–309 (2008). 92 Lau J, Ioannidis JP, Terrin N, Schmid CH, Olkin I: The case of the misleading funnel plot. BMJ 333(7568), 597–600 (2006). Websites 101 Arlequin software http://lgb.unige.ch/arlequin 102 Stats direct statistical software www.statsdirect.co.uk/help/miscellaneous/ nnt.htm 103 Higgins JP, Green S: Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1. 2008 www.cochrane-handbook.org monitoring of immunomodulators in inflammatory bowel disease. Aliment. Pharmacol. Ther. 21, 307–319 (2005). Pharmacogenomics (2010) 11(2) future science group