Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
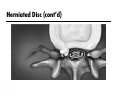
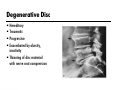
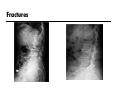
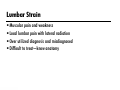
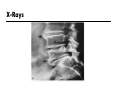
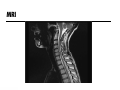
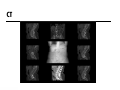
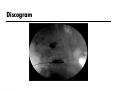
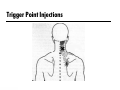
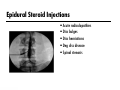
Differential Diagnosis of Low Back Pain Arnold J. Weil, MD, MBA Non-Surgical Orthopaedics, P.C. Atlanta, GA Objectives Identify primary pain generators that contribute to low back pain Discuss the routine evaluation of low back pain Identify common causes of low back pain Introduction to Low Back Pain LBP very disabling and accounts for over 50% of Workers’ Comp costs 80-$100 billion per year Affects up to 85% of adults Leading cause of disability ages 19-45 In 2010 in the United States there were over 15 million office visits to physicians for low back pain, second only to the common cold as a symptomatic reason for a physician visit 75% of costs due to 5% of patients 95% of all LBP is non-surgical Risk Factors Smoking Obesity Older age Gender Strenuous or sedentary work Job satisfaction Psychological factors (anxiety, depression, etc) The Natural History of Back Pain By 6 weeks – 65% of patients have recovered By 12 weeks – 85% of patients are improved After 12 weeks – Recovery is less likely After 26 weeks – Fewer than half ever return to work After 104 weeks – Likelihood of returning to work is virtually nil The Evolving Approach Towards Back Pain Then Prolonged bed rest Absence from work Sedating medications Physical modalities Passive patient Routine diagnostic testing Aggressive surgical approaches Now Minimal or no bed rest Rapid return to work Sedation not desired Active rehabilitation Active patient participation Look for the red flags first Aggressive non-surgical treatment Lumbar Anatomy Bones/joints Muscles Discs Ligaments Nerve roots Lumbar Spine Low Back Pain Multiple anatomic sources No standard methods for categorizing, diagnosing, or treating pain syndromes Treatment protocols varied • Rest, exercise • Physical therapy • Spinal manipulation • Oral medications • Injection therapies • Surgery/other Sources of Low Back Pain Discs Bone/joint Muscles/ligaments Nerve roots Inflammatory History Evidence of systemic disease Evidence of neurologic compromise Social or psychological issues Risk factors Mechanism of injury Red flags (neoplasms, cauda equina, etc) Causes of Low Back Pain Hereditary disorders Degenerative disorders Traumatic injuries Soft tissue/muscle injuries Insidious onset Other Common Disorders of the Spine Herniated disc Degenerative disc Facet arthropathy Sacroiliac joint dysfunction Lumbar strain Fibromyalgia Arthritis Common Symptoms Associated With Back Pain Low back discomfort Sciatica/leg pain Muscle spasms Hip, buttock, or groin pain Numbness or tingling into the extremity Motor weakness Other “unusual” symptoms Herniated Disc Bulging/protruding Herniated Ruptured Extruded fragment Herniated Disc (cont’d) Herniated Disc (cont’d) Herniated Disc Symptoms Symptoms commonly involve back pain Radiation into the extremities Associated with muscle spasm Treatment is non-surgical Degenerative Disc Hereditary Traumatic Progressive Exacerbated by obesity, inactivity Thinning of disc material with nerve root compression Symptoms of Degenerative Disc Disease Symptoms are centrally located May involve buttock or proximal leg pain Associated with facet syndrome Non-surgical Fractures Sacroiliac Joint Dysfunction Localized pain in the SI joint Common in women and with trauma Conservative treatment Lumbar Strain Muscular pain and weakness Local lumbar pain with lateral radiation Over utilized diagnosis and misdiagnosed Difficult to treat—know anatomy Musculoskeletal Pain Soft Tissue Injuries Sprains and strains –strain = stretching injury to muscle • trapezius, rhomboids –sprain = injury to ligament • capsular injury connecting lumbar facet joint and vertebrae Piriformis syndrome Myofascial pain Nerve Injuries Sciatic nerve injury Peripheral nerve injuries Nerve root injuries Distal nerve injuries Fibromyalgia Chronic pain syndrome Non-specific complaints Non-specific objective findings Usually overlying back pain Arthritis Osteoarthritis Rheumatoid arthritis Seronegative spondyloarthropathies Autoimmune diseases Other Disorders Associated With Back Pain Hip Piriformis Hamstring Pelvic or abdominal mass Gynecological (adhesions, fibroids, endometriosis) Other Spine Entities Meningioma Destructive/lytic lesions Physical Examination Observation & palpation/tenderness Range of motion Straight leg raise Neurological exam Evaluation for malignancy Non-organic or Waddell’s signs Psychological assessment Diagnostic Studies X-rays MRI CT EMG/NCS Discography X-Rays MRI CT EMG/NCS Discogram Treatment Medications Therapies Alternative medicine Injections Medications Anti-inflammatory medications Muscle relaxants Analgesics Neuropathic medications Topical medications Therapy Physical therapy Massage therapy Chiropractic therapy Injections Trigger point injections Botulinum toxin type A injections Epidural steroid injections Joint injections Facet injections Trigger Point Injections Botulinum Toxin Type A Injections Epidural Steroid Injections Acute radiculopathies Disc bulges Disc herniations Deg disc disease Spinal stenosis Intra-articular Injections Facet Injections Radiofrequency Lesioning Percutaneous Disc Decompression IntraDiscal ElectroThermal Therapy (IDET) Spinal Cord Stimulation Trial SCS for 1 to 2 weeks If > 50 % pain relief may benefit from permanent implant Dual electrodes available for bilateral extremity coverage or complex pain patterns Surgical Treatment Discectomy Fusion Disc decompression Fracture stabilization Summary Back pain is 2nd most common reason for MD visit Focused history and examination Variety of causes for low back pain Physician must identify and treat the cause Conservative treatment Surgery is the last option References Schwarzer, A.C., Aprill, C.N., Derby, R., Fortin, J., Kine, G., and Bogduk, N. Clinical features of patients with pain stemming from the lumbar zygapophyseal joints(Is the lumbar facet syndrome a clinical entity?). Spine. 1994; 19: 1132–1137 Saal, J.S. General principles of diagnostic testing as related to painful lumbar spine disorders: a critical appraisal of current diagnostic techniques. Spine. 2002; 27: 2538–2545 Schwarzer, A.C., Aprill, C.N., and Bogduk, N. The sacroiliac joint in chronic low back pain. Spine. 1995; 20: 31–37 Slipman, C.W., Lipetz, J.S., Plastaras, C.T. et al. Fluoroscopically guided therapeutic sacroiliac joint injections for sacroiliac joint syndrome. Am J Phys Med Rehabil. 2001; 80: 425–432 Slipman, C.W. and Chow, D.W. Therapeutic spinal corticosteroid injections for the management of radiculopathies. Phys Med Rehabil Clin N Am. 2002; 13: 697–711 Schwarzer, A.C., Wang, S.C., Bogduk, N., McNaught, P.J., and Laurent, R. Prevalence and clinical features of lumbar zygapophysial joint pain: a study in an Australian population with chronic low back pain. Ann Rheum Dis. 1995; 54: 100–106 Braddom's Physical Medicine and Rehabilitation