Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
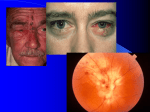
Case Challenge Chest Pain in a 17-Year-Old Girl with Chickenpox Abdenasser Drighil, MD; Ayoub El hammiri, MD; and Fatima Belmourida, MD A 17-year-old girl presented with a 7-day history of pruritic vesicular rash (Figure 1), chest pain, and general malaise. In the preceding 2 weeks, her 9-year-old sister had contracted a similar rash that was diagnosed clinically as “chicken pox” (ie, varicellazoster virus [VZV]). Initial treatment included salicylates and topical treatment. The patient had experienced no major illness prior to these symptoms. There was no relevant family history of heart disease. On admission, the physical examination revealed a typical VZV rash. The cardiac examination was benign except for a heart rate of 105 beats/minute. The patient was afebrile, and her blood pressure was 125/60 mm Hg. The lungs were clear to auscultation, the first and second heart sounds were normal, there were no murmurs, clicks, or rubs, and the liver was not enlarged. An electrocardiogram confirmed sinus tachycardia (105 beats/minute) and revealed an upwardly concave ST-segment elevation in leads V3-V6, II, and aVF (Figure 2); these abnormalities returned to normal 5 days later. Laboratory investigation showed an elevated creatine kinase (CK) of 194 U/L with a CK myocardial band concentration of 39 U/L. Other elevations included troponin I at 2.99 mcg/L, lactate dehydrogenase at 359 U/L, and C-reactive protein at 8 mg/L. Her white cell count was 10,110/mm3 with 47% neutrophils, 43% lymphocytes, and 6.2% monocytes. Fibrinogen was 5.5 g/L, and creatinine, blood urea nitrogen, and hepatic transaminase levels were all normal. An enzyme-linked immunosorbent assay was positive for VZV with elevated immunoglobulin M and immunoglobulin G (5.3 and 1.9 mUI/mL, respectively). Serologic studies for hepatitis B and C and HIV were negative. Two-dimensional echocardiography revealed left ventricular (LV) apical, inferolateral, and inferoseptal hypokinesis, but with a normal global LV ejection fraction of 58%. There was trivial mitral regurgitation and a small pericardial effusion. Figure 1. Vesicular rash on the nose and cheek area. Abdenasser Drighil, MD, is a Professor. Ayoub El hammiri, MD, is a Resident. Fatima Belmourida, MD, is a Resident. All authors are affiliated with the Department of Cardiology at Ibn Rochd University Hospital. Address hammiri, correspondence MD, Department to Ayoub of Cardiology, El Ibn Rochd University Hospital, 1er Quartier des hôpitaux, Casablanca, Morocco; email: [email protected]. Disclosure: The authors have no relevant financial relationships to disclose. doi: 10.3928/00904481-20150910-05 Figure 2. Electrocardiogram showing sinus tachycardia and upwardly concave ST-segment elevation in leads V3, V4, V5, V6, DII, and aVF. For diagnosis, see page 364 Editor’s note: Each month, this department features a discussion of an unusual diagnosis. A description and images are presented, followed by the diagnosis and an explanation of how the diagnosis was determined. As always, your comments are welcome via email at [email protected]. continued on page 364 PEDIATRIC ANNALS • Vol. 44, No. 9, 2015 359 Case Challenge continued from page 359 Diagnosis: Varicella Myocarditis Delayed reperfusion imaging by magnetic resonance imaging with gadolinium injection showed inferoseptal LV hypokinesies with minimal pericardial effusion (Figure 3), consistent with a diagnosis of varicella myocarditis. The patient was treated with acyclovir (10 mg/kg/day intravenously) for the first 48 hours, then acyclovir (30 mg/kg per day orally) and a nonsteroidal antiinflammatory agent (diclofenac 50 mg 3 times daily) for 8 days, and then atenolol (50 mg daily) and ramipril (2.5 mg daily) after the diagnosis of varicella myocarditis. CK returned to normal by the fifth day. Arrhythmias were not observed at any time. During 3 months of followup, LV systolic function as assessed by echocardiography increased to 65%. DISCUSSION VZV or common chickenpox is a highly contagious disease that usually runs a benign course, but in the neonatal period and in immunocompromised patients, rare and serious complications A may be encountered,1 including the development of cardiomyopathy with subsequent heart failure. In adults, VZV myocarditis with associated arrhythmias is less well documented. VZV myocarditis in adults as well as in children may be associated with severe complications, including progressive heart failure as well as malignant arrhythmias and sudden death.2 Lorber et al.3 found that the typical time course for discovery of cardiac involvement was 2 weeks or longer after the onset of a typical skin rash. Limited information is available regarding the subclinical myocardial insult in the course of VZV infection. It can only be assumed that were it looked for, more cases of covert mild cardiac involvement might be found compared to those with frank overt signs and symptoms of cardiac decompensation.4 When detected, cardiac involvement commonly includes only nonspecific T wave changes on the electrocardiogram.2 This suggests the possibility that subclinical myocarditis may be present in most cases of acute VZV infection and that it can be diagnosed in a more comprehensive cardiac diagnostic examination after the appearance of the typical rash. B Figure 3. Cardiac magnetic resonance imaging. (A) Four-chambers slice highlighting uptake contrast at lateral and posterior wall after injection of gadolinium (arrow). (B) Cardiac short-axis cut highlighting uptake contrast at lateral wall after injection of gadolinium (arrow). 364 The treatment of acute VZV myocarditis is largely supportive, but because of the rarity of this disease, there are no generally accepted therapeutic guidelines. This includes the use of acyclovir, an inhibitor of herpesvirus DNA replication. Because of the rarity of VZV myocarditis, there are no data to support its effectiveness. Acyclovir is the drug most commonly used in the treatment of immunocompetent adults with VZV. One small prospective and several retrospective reports suggest clinical benefits,5,6 and most experts recommend its use in adults with VZV complications.7 Given its minimal toxicity, acyclovir seems warranted in the setting of acute symptomatic VZV myocarditis. Acyclovir is useful against VZV for preventing dissemination in immunocompromised children, and in shortening the duration of fever and skin manifestations when given orally within 24 hours of the development of the rash.8 We speculate that acyclovir may be beneficial in VZV myocarditis if presentation occurs during the stage of viral replication within the myocardium. This is more likely early in the course of the illness, when new skin lesions are still appearing. Steroids have been used experimentally in patients with myocarditis;9 However, there have been no controlled studies supporting their effectiveness in infectious myocarditis associated with VZV. Similarly, immunosuppression has not been shown to prevent long-term cardiac morbidity, and its use remains controversial. CONCLUSION VZV myocarditis is infrequently diagnosed. We suspect that clinical manifestations would be found more often if a comprehensive diagnostic investigation were undertaken after the appearance of the characteristic rash, and Copyright © SLACK Incorporated Case Challenge especially if the presentation included complaints of chest pain. Primary care and emergency department medical providers should be aware of the potential for cardiac involvement in patients who present with common VZV infection. REFERENCES 1. Feldman S, Hughes WT, Daniel CB. Varicella in children with cancer: seventy-seven cases. Pediatrics. 1975;56:388-397. 2. Fiddler GI, Campbell RW, Pottage A, God- PEDIATRIC ANNALS • Vol. 44, No. 9, 2015 man MJ. Varicella myocarditis presenting with unusual ventricular arrhythmias. Br Heart J. 1977;39:1150-1153. 3. Lorber A, Zonk Z, Maisuls E, Dembo L, Palant A, Iancu TC. The scale of myocardial involvement in varicella myocarditis. Int J Cardiol. 1988;20:257-262. 4. Kajalainen J, Viitasalo M, Kalq VR, Heikkila J. 24-hour electrocardiographic recordings in mild acute infectious myocarditis. Ann Clin Res. 1984;16:34-39. 5. Al-Nakib W, Al-Kandari S, El-Khalik D, ElShirbiny AM. A randomised controlled study of intravenous acyclovir (Zovirax) against placebo in adults with chicken pox. Infect Dis. 1983;6:49-56. 6. Feder HM Jr. Treatment of adult chickenpox with oral acyclovir. Arch Intern Med. 1990;150:2061-2065. 7. Straus SE, Ostrove JM, Inchauspe G, et al. Varicella-zoster virus infections: biology, natural history, treatment, and prevention. Ann Intern Med. 1988;108:221-237. 8. Balfour HH Jr, Kelly JM, Suarez CS. Acyclovir treatment of varicella in otherwise healthy children. J Pediatr. 1990;116:633839. 9. Chan KY, Iwahara M, Benson LN, Wilson GJ, Freedom RM. Immunosuppressive therapy in the management of acute myocarditis in children: a clinical trial. J Am Coll Cardiol. 1991;17:458-460. 365