Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
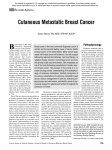
Case Report Bilateral Hypoglossal Nerve Palsy Due to Breast Cancer Skull Base Metastases Jennifer M. Matro, MD, Rohit Walia, MD, Kathryn Tumelty, CRNP, Tara Morrison, MD, and Lori J. Goldstein, MD Abstract Despite advances in endocrine therapy and chemotherapy, metastatic disease ultimately develops in about 30% of women diagnosed with early-stage breast cancer. Critical locations of bone metastases may result in specific symptoms. Metastases to the calvarium have the potential to cause cranial nerve palsies. While there have been isolated case reports of unilateral cranial nerve XII palsy, bilateral hypoglossal nerve palsy has never been reported. We report the first known case of bilateral hypoglossal nerve palsy in a 49-year-old woman with estrogen receptor– positive/progesterone receptor–positive, HER2/ neu-negative metastatic breast cancer. The patient underwent palliative radiation therapy with near complete resolution of symptoms. When a patient with metastatic cancer develops unusual neurological symptoms, a high index of suspicion for skull base disease must be maintained, and local therapy can improve quality of life. Introduction Despite advances in endocrine therapy and chemotherapy, metastatic disease ultimately develops in about 30% of women diagnosed with early-stage breast cancer.1 The most common sites of metastasis, beyond regional lymph nodes, are bone, lungs, liver, and brain.2 Critical locations of bone metastases may result in specific symptoms. Metastases to the calvarium have the potential to cause cranial nerve palsies. The most common cranial nerves affected in metastatic breast cancer are V and VII, although there have been isolated case reports of unilateral cranial nerve XII palsy. We report the first known case of bilateral hypoglossal nerve palsy in a 49-year-old woman with estrogen receptor–positive/progesterone receptor–positive (ER+/PR+), HER2/neu-negative metastatic breast cancer. fuse bone metastases 2 years prior. She had not responded to first-line hormonal therapy with tamoxifen and zoledronic acid, and so was switched to albumin-bound paclitaxel and bevacizumab with zoledronic acid. Bevacizumab was discontinued due to proteinuria and hypertension 4 months prior to her current presentation, at which time she was receiving only albuminbound paclitaxel and zoledronic acid. The patient had developed the sensation of a swollen tongue approximately 1 week prior and was treated with fluconazole, dexamethasone, and nystatin for presumed thrush. She returned with persistent tongue swelling and dysarthria. She denied dysphagia. On examination, the uvula was midline, and the tongue was flaccid and not edematous. Gag reflex was intact. Cranial nerves II through XI were intact, but the patient was unable to protrude and laterally move her tongue in either direction, indicating bilateral hypoglossal nerve palsy. The remainder of her neurological exam was normal. The patient was admitted to the hospital for expedited workup and management. figure 1. MRI T2 Axial Image Showing Metastatic Disease Involving the Bilateral Basiocciput Case Report A 49-year-old woman with stage IV, pT4 pN1 cM1, ER+/PR+, HER2/neu-negative breast cancer presented with subacute onset of a swollen tongue and difficulty speaking. The patient had been diagnosed with de novo stage IV breast cancer with dif- 22 www.ajho.com Hypoglossal canals november 2014 Bil ateral Hypoglossal Nerve Palsy Due to Breast Cancer Skull Base Metastases Practical Application • Management of patients with metastatic cancer requires a multidisciplinary team approach. • Clinicians must maintain a high index of suspicion in patients with metastatic cancer that atypical symptoms may be related to malignancy. • Selection of the optimal imaging study will aid in diagnosis. • Recognition of abnormal cranial nerve examination findings [AUTHORS: SHOULD MAKE COMPLETE SENTENCE TO BE PARALLEL WITH OTHERS.] The patient had been taking prochloperazine for chemotherapy-induced nausea. To rule out a dystonic reaction to compazine, benztropine was administered without relief of symptoms. An MRI of the brain with and without gadolinium subsequently revealed extensive calvarial metastases involving the skull base, including the clivus, bilateral occipital condyles, and C1 vertebra. Tumor was thought to be compressing the hypoglossal nerves as they traversed the hypoglossal canals at the skull base bilaterally. Figure 1 includes a T2 axial image showing metastatic disease involving the left and right basiocciput. Figure 2 shows a coronal post-contrast view of the hypoglossal canals, and Figure 3 demonstrates the skull base metastases on bone scan. The patient underwent neurosurgical evaluation to ensure stability of the C1/C2 junction and superior cervical spine, which was intact. She subsequently received radiation therapy to the clivus, C1 vertebral body, and adjacent skull base. Prescribed dosage was 3000 cGy in 10 fractions delivered with opposed lateral fields with 6 MV photons. On follow-up approximately 1 month later, the patient reported improved speech and was able to eat all foods. On examination, she was able to protrude the tongue but with persistent deviation to the right. Unfortunately, the patient had rapidly progressive disease, most markedly in the liver and mediastinum. Two weeks after followup, she developed a malignant pericardial effusion and expired due to multisystem organ failure. Discussion Metastatic disease is found in 5% of women at the time of breast cancer diagnosis. For those women with early-stage breast cancer, about 30% will ultimately develop distant metastases.1 Cranial nerve palsies are rare complications of metastatic cancer, occurring in less than 10% of patients with brain metastases.2 However, cranial nerves may be compromised due to bone metastases without intracranial lesions. Metastases to the skull base, which occurs in 4% of patients with cancer, with breast cancer being the most common primary site,3 may cause compression of and damage to cranial nerves as they exit the skull through the basal foramina. The most frequently affected cranial nerves in women with metastatic breast cancer are V and VII, with 70% and 60% of patients, respectively, having involve- VOL. 10, NO. 5 ment of these nerves.4 Several English-language case reports have been published describing unilateral hypoglossal nerve palsy due to skull base metastasis, but no reports have documented bilateral involvement.4-8 In the case series by Hall et al,4 only 4 of 10 patients had involvement of cranial nerve XII, 1 with isolated hypoglossal palsy and all with unilateral involvement. Greenberg et al8 performed a retrospective analysis of 43 patients with metastases to the skull base. Nine of 43 patients had involvement of the occipital condyle, and all 9 patients had unilateral 12th nerve palsy. Metastases at the basilar part of the occipital bone (basiocciput) and bilateral occipital condyles were likely the cause of our patient’s symptoms. figure 2. Coronal Post-Contrast Image Showing Skull Base Metastases Involving the Bilateral Hypoglossal Canals Jugular tubercles Hypoglossal canals Our case represents the first report of bilateral hypoglossal nerve palsy due to skull base bone metastases. The diagnosis was made by MRI imaging, the imaging study of choice for skull base involvement, although bone scan with SPECT could be used for this purpose.9 While the average survival time for patients with cranial nerve palsy due to skull base metastasis can be up to 2 years, those with intracranial metastases have a median survival ranging from 5.6 to 14.4 months, depending on number of lesions, performance status, hormone and HER2 receptor status, and response to systemic treatment.10,11 Despite a significant clinical improvement following local radiotherapy, our patient ultimately died from her cancer due to systemic progression 3 months after her symptoms developed. This case indicates that when a patient with metastatic cancer develops unusual neurological symptoms, a high index of suspicion for skull base disease must be maintained, especially in THE AMERICAN JOURNAL OF HEMATOLOGY/ONCOLOGY 23 Case Report figure 3. Bone Scan Demonstrating Bilateral Skull Base Metastases (white arrows) RT. LAT LT. LAT Series Description: Wholebody Radiopharmaceutical 1: 910.2 MBq (24.60 mCi) MDP Energy Window Group 1: 99m Technetium WB Technique: 1PS Scan Velocity: 2.00 mm/sec Table Traverse: 0.00 mm Table Height: 0.00 mm the absence of intracranial lesions. Aggressive local therapy can lead to near-complete resolution of symptoms and improvement in quality of life for patients with an otherwise significantly limited life expectancy. 5. Pavithran K, Doval DC, Hukku S, Jena A. Isolated hypoglossal nerve palsy due to skull base metastasis from breast cancer. Australas Radiol. 2001;45:534-535. 6. Endo K, Okano R, Kuroda Y, et al. Renal cell carcinoma with skull base metastasis preceded by paraneoplastic signs in a chronic hemodialysis patient. Int Med. 2001;40(9):924-930. 7. Shiraishi T, Yanagida H, Takada K, Yasuhara Y. Unusual cranial metastasis from hepatoma presenting as isolated unilateral hypoglossal nerve paresis. Neurol Med Chir. 1992;32:166-168. 8. Greenberg HS, Deck MDF, Vikram B, et al. Metastasis to the base of the skull: clinical findings in 43 patients. Neurology. 1981;31:530-537. 9. Fukumoto M, Osaki Y, Yoshida D, et al. Dual-isotope SPECT diagnosis of a skull-base metastasis causing isolated unilateral hypoglossal nerve palsy. Ann Nuc Med. 1998;12(4):213-216. 10. Melisko ME, Moore DH, Sneed PK, et al. Brain metastases in breast cancer: clinical and pathologic characteristics associated with improvements in survival. J Neurooncol. 2008;88(3):359-365. 11. Lee SS, Ahn JH, Kim MK, et al. Brain metastases in breast cancer: prognostic factors and management. Breast Cancer Res Treat. 2008;111(3):523-530. Affiliations: Jennifer M. Matro, MD, is from the Abramson Cancer Center, University of Pennsylvania, Philadelphia; Rohit Walia, MD, is from the Fox Chase Cancer Center, Department of Diagnostic Imaging, Philadelphia, PA; and Kathryn Tumelty, CRNP, Tara Morrison, MD, and Lori J. Goldstein, MD, are from the Fox Chase Cancer Center, Department of Medical Oncology. Disclosures: TK Address correspondence to: Lori J. Goldstein, MD, 333 Cottman Avenue, Philadelphia, PA 19111; phone: 215-728-2985; fax: 215-728-2880; email: [email protected] References 1. Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2008. National Cancer Institute. http://seer. cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the SEER web site, 2011. Accessed September 19, 2014. 2. Carty NJ, Foggitt A, Hamilton CR, Royle GT, Taylor I. Patterns of clinical metastasis in breast cancer: an analysis of 100 patients. Eur J Surg Onc. 1995;21:607-608. 3. Laigle-Donadey F, Taillibert S, Martin-Duverneuil N, et al. Skull-base metastases. J Neurooncol. 2005;75(1):63-69. 4. Hall SM, Buzdar AU, Blumenscheine GR. Cranial nerve palsies in metastatic breast cancer due to osseous metastasis without intracranial involvement. Cancer. 1983;52:180-184. 24 www.ajho.com november 2014