Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
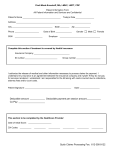
Hartsville Physical Therapy & Rehabilitation Center Our Federal Tax ID#: 200839150 Our NPI#: 1427087113 INSURANCE VERIFICATION FORM Date: ________________________________ Calling to check physical therapy benefits for: Patient: ________________________________________________ Ins ID#: ___________________________________ DOB: ____________________________ Group#: _________________________________ Diagnosis/Description: _____________________________________________________________________ Spoke to? ____________________________________________ Call reference #: ______________________ Effective Benefit Period of Policy: ____________________________ to _____________________________ Is there a deductible? No Yes If yes, how much? ________________________________________ How much of the individual deductible has been met? ____________________________ How much of the family deductible has been met? Is there an out-of-pocket maximum? No Yes ____________________________ If yes, how much? ________________________________ How much of the out-of-pocket max has been met? ____________________________ What percentage does insurance pay? _________________ Copay amount? _____________________ Are there limitations for physical therapy? No Yes If yes: Number of visits insurance pays per year? Max dollar amount insurance pays per year? ___________________ PT only PT,OT,ST ___________________ Other limitations? ______________________________________________________________ Does physical therapy need preauthorization? No Yes Preauth. #: ________________________________ Electronic payer id# for Emdeon Clearinghouse? _____________________________ Special Instructions/Notes: ____________________________________________________________________ ___________________________________________________________________________________________ Verified by: _____________________________________________ Initial: ________________________