Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
The effect of the correction of metabolic acidosis
on nitrogen and potassium balance of patients
with chronic renal failure13
NJ Papadoyannakis,
Cf Stefanidis,
and
M McGeown
KEY WORDS
nitrogen,
urea
Chronic
renal
nitrogen
appearance,
failure,
sodium
bicarbonate,
glomerular
filtration
rate
chloride,
blood
urea
Methods
Introduction
There
is considerable
evidence
that
chronic
renal
failure
(CRF)
is a catabolic
illness (1 , 2) and the waste products
from
endogenous
protein
can contribute
to the
uremic
syndrome.
Excessive
protein
intake
can exacerbate
uremic
symptoms,
because
it will increase
urea production
(3). The
same effect
on urea production
has been
described
in uremic
animals
with metabolic
acidosis
(4).
It has been described
since 193 1 that sodium
bicarbonate
(SB) supplementation
is
beneficial
in many patients
with CRF (5). In
addition
it has been shown that administration of SB results in a significant
decrease
of
urea production
(6). However,
it has never
been established
whether
this is the result of
the increase
of the extracellular
volume
or
of the correction
of metabolic
acidosis.
To
distinguish
the effect ofthe
above factors we
analyzed
the results
of nitrogen
and potassium balance
studies
performed
before and
during
periods
of supplementation
with SB
and sodium
chloride
(SC).
The American
Journal ofClinical
Nutrition
40:
© 1984 American
Society for Clinical
Nutrition
sodium
SEPTEMBER
Two hundred
nitrogen
and potassium
balance
studies were carried out in six nondialyzed
patients
aged 25
to 65 yr. Clinical
and laboratory
data ofthe
patients
at
the beginning
ofthe
study are summarized
in Table 1.
During
the study patients
were hospitalized
and were
weighed
daily under standard
conditions.
Calorie,
protein,
and potassium
intakes
were calculated by the same dietitian
from standard
tables
(7) and
did not differ significantly
during
the control
and the
supplementation
periods
(Table
2). Each patient
was
treated
with alternate
courses
of the same amount
(0.7
to 1.2 mEq/kg/day)
ofSC and SB of9.8 ± 0.8 and 9.3
± 0.6 days, respectively.
Protein
nitrogen
in the urine and feces was measured
by the Kjeldahl
method
(8). Protein
in the urine was
estimated
by the Biuret method
and plasma
bicarbonate, blood urea nitrogen (BUN), plasma potassium,
and
serum and urine creatinine
were measured
by conventional methods.
Nitrogen
balance
and urea
nitrogen
appearance
‘From the Divisions
ofNephrology,
Hospital,
Athens,
Greece
and Belfast
Belfast, Northern
Ireland
2
Presented
in part
at the
Athens General
City Hospital,
III Congress
on
Nutrition
and
Metabolism
in Renal Disease.
3Address
reprint
requests
to: Ni Papadoyannakis,
Division
of Nephrology,
Athens-General
Hospital,
Cholargos,
Athens, Greece.
Received May 31, 1983.
Accepted
for publication
April 10, 1984.
1984,
pp
623-627.
Printed
in USA
623
Downloaded from ajcn.nutrition.org at PENNSYLVANIA STATE UNIV PATERNO LIBRARY on March 5, 2016
ABSTRACT
Nitrogen
and potassium
balance
studies
were conducted
in six nondialyzed
uremic
patients.
Each patient
was investigated
before and after supplementation
with sodium
bicarbonate
and sodium chloride.
Every period ofthe study lasted longer than 1 wk. Each patient
had the same calorie and protein
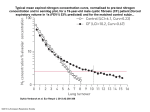
intake during the whole study. Urea nitrogen
appearance
was
correlated
with protein
intake for the assessment
of the compliance
of patients
with their diets.
There was a significant
decrease
of blood urea nitrogen
(p = 0.014) of 36% during
bicarbonate
supplementation
and both metabolic
balance
studies
improved
significantly
(p = 0.0005
and
0.0096).
However,
there was no significant
improvement
during sodium
chloride
administration
indicating
that the effect ofbicarbonate
was the result ofthe correction
ofmetabolic
acidosis and
not of the expansion
of the extracellular
volume.
Am J C/in Nuir 1984;40:623.-627.
624
PAPADOYANNAKIS
TABLE
Summary
AL
1
ofclinical
and
Patient
laboratory
Age
WI
F
F
F
F
M
F
58
29
61
25
32
65
kg
55
55
73
49
68
58
45±7.4
chronic
p yeloneph
ritis;
TABLE
2
Nutritional
characteristics
Patient
ofpatients
Sex
±SEM
. CP,
data
rn//mini!.
g/day
ntEq/day
days
2002
2180
2495
2532
2200
2522
69
64
31
49
30
39
50
50
65
49
59
50
47±6.8
54±2.7
of
41
33
32
32
25
37
33±2.2
TABLE
3
Mean values of body wt (BW), BUN, urinary area
nitrogen
(UUN),
and UNA during SB and SC periods
BW
BUN
UUN
UNA
Patient
SB
SC
kg
I
2
3
4
5
6
57
57
74
52
70
59
p
>0.05
SB
SC
55
58
74
51
70
60
45
12
76
41
62
79
=0.007
SB
SC
SB
g/day
mg/dl
64
15
99
53
95
98
9.1
10.8
4.6
8.0
3.9
5.7
=0.037
SC
g/day
10.3
14.9
5.7
8.7
4.8
6.6
73 m2
mg/d!
76
17
119
60
132
111
86±18
Serum
HCO
mEq/L
15.3
16.8
14.0
14.9
15.0
19.0
15.8±0.7
stic kidneys.
Results
kca//day
2322±92
; PK, polycy
patients
Duration
study
I
2
3
4
5
6
11.4
18.8
4.1
14.9
3.4
4.7
9.5±2.6
nep hrocalcinosis
Potassium
intake
intake
study
BUN
CP
NC
PK
CP
CP
CP
Protein intake
Calorie
ofthe
Diagncsis
60±3.7
NC,
ofthe
at the beginning
8.6
9.8
4.2
6.9
3.8
5.1
11.4
15.6
6.3
9.1
5.9
7.1
=0.005
(UNA)
were measured
every day during
the various
periods
of the study
and their average
values
were
compared
after the 3rd day of each supplementation
period. UNA was calculated
as described
by Grodstein
et al (9). Nitrogen
and potassium
balance
studies were
calculated
as described
by Kopple
and Coburn
(10).
Nitrogen
and potassium
were measured
in vomited
food, in feces, and in urine. Glomerular
filtration
rate
(GFR) was estimated
from the mean of urea and creatinine
clearance.
The protocol
of this study was approved
by the human
subjects
committee
of our hospital.
The “Student’s”
paired test was used to compare
the
changes
of the parameters
of each patient.
All values
were expressed
as mean ± SEM.
Results
were considered statistically
significant
for p < 0.05.
The
24-h volume
of the urine
and the
weights
of patients
increased
significantly during their supplementation
with SB
and SC (p = 0.005 and 0.004,
respectively).
We noticed
a direct correlation
of the above
parameters
(r = 0.95, p = 0.03). GFR did
not increase
significantly
during
the period
of SB and SC supplementation
and there
was no significant
difference
of the average
GFR values between
the two periods.
Plasma
bicarbonate
increased
from
15.8
± 0.7 mEq/L
during
the control
period
to
23.4 ± 1 .2 mEq/L
at the SB period
(p =
0.0006).
Serum potassium
mean values were
in the normal
range
and did not change
significantly
during
the various
periods
of
the study. BUN decreased
significantly
during the SB period
(p = 0.014) and increased
again significantly
during
the SC period (Table 3).
UNA was directly
correlated
with nitrogen
intake
during
the control
(r = 0.91,
p =
0.0 1 1), SB (r = 0.97, p = 0.00 1), and SC
period
(r = 0.89, p = 0.017).
There
was a
decrease
of UNA during
the SB period
(p =
0.002) and then UNA increased
significantly
during
SC supplementation
(Table
3).
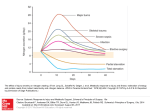
There
was a significant
increase
of the
mean values ofboth
nitrogen
and potassium
balance
during
the SB period
(p = 0.0005
and 0.0096,
Fig 1). However,
there was no
significant
change during
the SC period.
The
major
change
accounting
for the improvement
of nitrogen
balance
was the decrease
in UNA rather
than changes
in fecal nitrogen or nonurea
nitrogen.
body
Downloaded from ajcn.nutrition.org at PENNSYLVANIA STATE UNIV PATERNO LIBRARY on March 5, 2016
1
2
3
4
5
6
x±SEM
ET
NITROGEN
Patient
AND
POTASSIUM
BALANCE
2
I
STUDIES
3
IN
UREMIA
625
5
4
6
6#{149}
Nitrogen
balance
(gr/24
hrs)
cu;
40
30
Potassium
balance
(mEq/24
0
20
#{149}
bra)
10
FIG
1. Mean
values
of nitrogen
and
iid1
potassium
balance
Discussion
There
has been a rapid accumulation
of
evidence
indicating
that malnutrition
is a
frequent
and important
problem
of patients
with CRF (1, 2). Poor food intake
and the
removal
ofnutrients
with dialysis are usually
responsible
for this problem
(1 1). In addition
there are experimental
studies
stating
that
there
is a decrease
of protein
synthesis
in
uremia
(12) and an increase
of urea production was described
in chronic
uremic
rats
with metabolic
acidosis
(4).
Some authors
suggest
that it is not necessary to correct
plasma
bicarbonate
of more
than 15 mEq/L
(1 3). In contrast
a significant
improvement
of both nitrogen
and potassium
balance
was achieved
in this study
when
plasma
bicarbonate
was
increased
from 15.8 ± 0.7 to 23.4 ± 1.2 mEcijL.
All
of our patients
had a normal
arterial
blood
pressure
before and after SB and SC administration
and no one developed
edema.
Obviously
SB should
not be given in hypertensive patients.
The correction
of metabolic
acidosis
in
children
is very important,
because
it might
normalize
their
growth
impairment.
This
was documented
with children
with type 1
renal tubular
acidosis
(14-17)
and in premature
infants
on high-protein
diets
(18,
studies
during
Control
Sodium
period
bicarbonate
period
IW
cii
control
and
SB supplementation.
19). The mechanism
responsible
for the poor
growth
of such patients
is not well established.
Further
studies
to investigate
the effeet of metabolic
acidosis
on protein
metabolism would be of interest.
Whether
correction
of metabolic
acidosis
affects the activity
of liver enzymes
responsible for protein
synthesis
remains
an open
problem.
It has been described
by HoppeSeyler et al (20) that in acute renal failure
there is an increase
of urea production
possibly related
to the increase
ofthe
activity
of
urea cycle enzymes
(20). However,
such a
mechanism
was not documented
in the
uremic
patients
of Tizianello
et al (21).
There
is experimental
evidence
that metabolic
acidosis
stimulates
protein
breakdown
in muscle
tissue and the amino
acid
nitrogen
with probably
some carbon
skeletons are channeled
into glutamine.
Then
glutamine
could be taken up by the kidney
for ammonia
production
(22). Thus it appears that muscle
supplies
the extra glutamine that is taken
up by the kidney
during
metabolic
acidosis.
However,
others
report
that metabolic
acidosis
does not affect glutamine
release (23). In addition,
the increase
in glutamine
release
during
acidosis
might
not be the result
of protein
degradation
if
the carbons
of glutamine
are derived
from
other amino
acids. In fact, in the study of
Downloaded from ajcn.nutrition.org at PENNSYLVANIA STATE UNIV PATERNO LIBRARY on March 5, 2016
13
::
Jij
626
PAPADOYANNAKIS
References
1. Kopple
JD. Abnormal
metabolism
in uremia.
amino
Kidney
acid and protein
Int 1978;14:340.
AL
2. Holliday
MA, Chantler
tional factors in children
Kidney
mt
CA. Metabolic
and nutriwith kidney insufficiency.
1978;l4:306.
3. Johnson
WJ, Hagge WH, Waggoner
RD, Dinapoli
RD, Rosevear
JW. Effects of urea loading
in patients with far-advanced
renal failure.
Mayo Clin
Proc l972;47:21.
4. Simon
D, Luke RG. Rate of rise of blood
urea
nitrogen
in acute renal failure:
effect of acidosis.
Proc Soc Exp Biol Med 1976;137:1073.
5. Lyon DM, Dunlop
DM, Stewart
CP. The alkaline
treatment
of chronic
nephritis.
Lancet
l931;2:
1009.
6. Blom Van Assendelft
PM, Dorhout
Mees EJ. Urea
metabolism
in patients
with chronic
renal failure:
influence
of sodium
bicarbonate
or sodium
chloride administration.
Metabolism
1970;l9:1053.
7. McCance
AA, Widdowson
EM. The composition
of foods. Medical
Research
Council
special report
series no 297. H.M.S.O.,
1960; London:
HMSO
8. Henry JB. Nitrogen
analysis.
In: Davidson
J, Henry
JB, ed. Todd-Sandford
clinical
diagnosis
by laboratory
methods.
15th ed. Philadelphia,
PA: WB
Saunders.
9. Grodstein
GP, Blumenkrantz
MJ, Kopple JD. Nutritional
and metabolic
response
to catabolic
stress
in uremia.
Am J Clin Nutr l976;33:141
1.
10. Kopple
JD, Coburn
JW. Metabolic
studies of low
protein diets in uremia.
I. Nitrogen
and potassium.
Medicine
1973;52:583.
1 1. Kopple
JD, Swenseid
ME, Shinaberger
JH, Umegawa CM. The free and bound
amino
acids removed by hemodialysis.
Trans Am Soc Artif Internal Organs
l973;19:309.
12. Grossman
SB, Shafritz
DA. Influence
of chronic
renal failure on protein
synthesis
and albumin
metabolism
in rat liver. J Clin Invest 1977;59:869.
13. Shwartz
WB, Relman
AS. Effects
of electrolyte
disorder
on renal structure
and function.
N Engl J
Med 1967;276:283.
14. Nash MA, Torrado
AD, Grefer I, Spitzer A, Edelmann CM Jr. Renal tubular
acidosis in infants and
children.
J Pediatr
1972;80:738.
15. Stickler GB, Bergen BJ. A review: short stature
in
renal disease.
Pediatr
Res 1973;7:978.
16. McSherry
E, Morris RC Jr. Correction
of impaired
growth
in children
with classic renal tubular
acidosis (CRTA)
by sustained
correction
of acidosis.
Clin Res l973;21:700.
17. McSherry
E. Acidosis
and growth
in nonumeric
renal disease.
Kidney
Int 1978;14:349.
18. Heally CE. Acidosis
and failure to thrive in infants
fed nutramigen.
Pediatrics
1972;49:910.
19. Radde
IC, Chance
OW, Bailey K, O’Brien
J, Dar
GM, Sheepers
J. Growth
and mineral
metabolism
in very low birthweight
infants.
Pediatric
Res
1975;9:564.
20. Hoppe-Seyler
G, Maier KP, Schollmeyer
P, Frohlich J, Talke H, Gerok
W. Studies
on urea cycle
enzymes
in rat liver during
uremia.
Eur J Clin
Invest l975;5:15.
21. Tizianello
A, De Ferrari G, Garibotto
G, Gurreri
G, Bruzzone
M. Cerebral
and hepatic
urea synthe
Downloaded from ajcn.nutrition.org at PENNSYLVANIA STATE UNIV PATERNO LIBRARY on March 5, 2016
Schrock
et al (22), there was no change
in
the release
of tyrosine,
phenylalanine,
or
lysine (amino
acids which
are neither
synthesized
nor degraded
by muscle)
during
acidosis.
The improvement
of nitrogen
balance in our study and the decrease
of urea
nitrogen
appearance
during
the correction
of metabolic
acidosis
was possibly
the result
of increased
protein
synthesis
or decreased
protein
breakdown.
Although
it seems
unlikely that muscle
protein
degradation
is altered substantially
in acidosis.
It is more difficult
to explain
the improvement
of potassium
balance.
Our patients
were normokalemic
during all study periods.
However,
a potassium
deficiency
during
the
control
period cannot
be excluded.
This deficiency
was possibly
corrected
by the reversal of acidosis.
We found a significant
decrease
of BUN
during
SB supplementation
(36%,
p =
0.0 14). A less pronounced
drop
of BUN
(19%, p < 0.05) was described
by Blom Van
Assendelft
and Dorhout
Mees (6). Unfortunately
there was no information
about
the
protein,
calorie intake,
or UNA of their patients.
The different
effect of SB in their
study was possibly
the result of dietitic
differences
and/or
the amount
of SB that was
given. Recent
protein
intake can be assessed
by UNA which gives an estimation
of total
nitrogen
output.
In all periods
of our study
UNA
correlated
directly
with nitrogen
intake indicating
acceptable
compliance
of patients with their diets.
All patients
were in good hydration
during
the control
period
of the study and this was
possibly
the reason
that their GFR was not
raised significantly
after SB and SC supplementation.
In addition
there was no significant difference
in GFR or significant
change
of body weight
between
the two periods.
Therefore
the improvement
of nitrogen
balance during
the SB period
was mainly
the
result ofthe
correction
of metabolic
acidosis
and not ofthe
expansion
ofthe
extracellular
volume.
a
ET
NITROGEN
22.
AND
POTASSIUM
sis in patients with chronic
renal insufficiency.
Proc
Eur Dial Trans Assoc l978;l5:500.
Schrock
H, Cha CM, Goldstein
L. Glutamine
release from hindlimb
and uptake by kidney
in the
acutely acidotic
rat. Biochem
J 1980;188:557.
BALANCE
23.
STUDIES
IN
UREMIA
627
Lemieux
G, Watford
M, Vinay
P, Gougoux
A.
Metabolic
changes
in skeletal
muscle
during
chronic
metabolic
acidosis.
Int J Biochem
1980;
12:75.
Downloaded from ajcn.nutrition.org at PENNSYLVANIA STATE UNIV PATERNO LIBRARY on March 5, 2016