Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Cardiac surgery wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
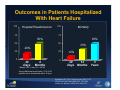
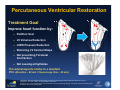
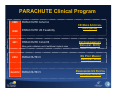
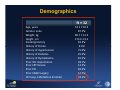
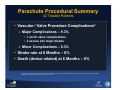
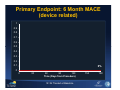
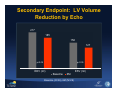
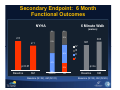
First Report of a Confirmatory (Cohort B) Study of the Parachute Device in Ischemic Dilated Cardiomyopathy Martyn R. Thomas, MD St. Thomas’ Hospital London, United Kingdom Disclosure Statement of Financial Interest I, Martyn Thomas, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation. Outcomes in Patients Hospitalized With Heart Failure 100 Hospital Readmissions 100 Mortality 75 75 50% 50 50% 50 33% 20% 25 25 0 0 30 Days 6 Months 12% 30 12 Days Months Median LOS: 6 days; N = 38,702 Among Medicare beneficiaries, 27% of HF patients are re-hospitalized within 30 days Aghababian RV. Rev Cardiovasc Med 2002; 3:S3 Jong P et al. Arch Intern Med 2002; 162:1689 Jencks and Williams. NEJM 2009; 360:1418 5 Years Percutaneous Ventricular Restoration This image cannot currently be display ed. This image cannot currently be display ed. This image cannot currently be display ed. This image cannot currently be display ed. Treatment Goal Improve heart function by: Partition Scar LV Volumes Reduction This image cannot currently be display ed. This image cannot currently be display ed. LVED Pressure Reduction Restoring LV Conical Shape Not preventing Torsional Contraction Not causing arrhythmias Procedural aspects similar to a standard PCI1,2(Duration – 80 min / Flouroscopy time – 20 min) 1.Nikolsky E, et al: An evaluation of fluoroscopy time and correlation with outcomes after percutaneous coronary intervention. J Invasive Cardiol. 15;99(8):1055-61, April 2007. 2.Varani E, et al: Cost of single-vessel and multivessel coronary drug-eluting stenting: comparison to the DRG funding level. Ital Heart J.;6(1):52-8, January 2005. Parachute Implant The Parachute™ device is comprised of a fluoropolymer (ePTFE) membrane stretched over a nitinol frame Nitinol frame to support torsional contraction and optimize LV outflow ejection Shape was designed to restore conical/longitudinal geometry The device is deployed into the apex of the left ventricle and partitions off noncontractile damaged myocardium to reduce LV volume and optimize performance of contractile, healthy myocardial Size Matrix 65 65s 75 75s 85 85s 95 95s 20cc Balloon CE Mark approval for all sizes. In the U.S., the Parachute system is an investigational device limited by federal law to investigational use only and is not available for sale. 16/14F sheath PARACHUTE Clinical Program 2005 PARACHUTE Cohort A 2008 PARACHUTE US Feasibility 2011 PARACHUTE Cohort B New guide catheters and 6 additional implant sizes 2012 PARACHUTE III Q4 2012 PARACHUTE IV CE MARK APPROVAL DATA (N=39) EU CONFIRMATORY DATA (EST. N=70) EU POST MARKET DATA (EST. N=50) RANDOMIZED US PIVOTAL DATA (EST. N=478) Parachute Technology Development • 2005 Parachute design freeze for CE Mark approval trials. • 2009 Feedback from early experience shows a need to improve the delivery system and offer more implant sizes for anatomy. • 2011 EU Confirmatory trial started to utilize the new catheters and 6 additional implant sizes. Trial Design: EU Cohort B Design • • • • • • DESIGN: Non-randomized, multicenter, observational study PATIENTS: Up to 100 Treated SITES: 20 Key Inclusion • NYHA II-IV • EF 15% - 40% • LV Wall Motion Abnormality Key Exclusion • Clinically significant untreated CAD • Revasc, CRT / ICD, or AMI within 60 days of enrollment • AR or MR > 2+ ANALAYSIS PLAN: Cohort B and PARACHUTE III will be combined to satisfy EU Post Market commitment 64 patients enrolled as of October 2012 Treatment Arm (N=57) Control Arm (N=7) Clinical follow-up at 6 months (N=32) Clinical follow-up at 6 months (N=2) Annually through 5 years EU Post Market Interim Analysis • 32 Treated Patients with 6M Follow-up • Primary Endpoint 6-month follow-up without the occurrence of Major Adverse Cardiac Events (MACE) related to the investigational device. • Secondary Endpoints Change in Left Ventricular Volume Indexes at 6 months Change in 6 minute walk test at 6 and 12 months Combined cardiovascular mortality and morbidity that includes all cause death, hospitalization for heart failure, myocardial infarction and stroke at 6 and 12 months Demographics N = 32 Age, years Gender, male Weight, kg Height ,cm Smoking History History of Stroke History of Hypertension History of Diabetes History of Dyslipidemia Prior ICD Implantation Prior CRT Device Prior PCI Prior CABG Surgery HF Hosp. 12M Before Enrolled 53.1 ± 10.3 87.5% 80.7 ± 13.3 173.6 ± 9.1 81.3% 9.4% 75.0% 25.0% 81.3% 28.1% 12.5% 84.4% 12.5% 34.4% Parachute Procedural Summary 32 Treated Patients • Vascular / Valve Procedure Complications3 Major Complications – 9.3% • 1 aortic valve complications • 2 access site major bleeds Minor Complications – 6.3% • Stroke rate at 6 Months – 0% • Death (device related) at 6 Months – 0% 3.Leon et al: Standardized endpoint definitions for transcatheter aortic valve implantation clinical trials: a consensus report from the Valve Academic Research Consortium. EU Heart Journal (2011) 32, 205-217. Primary Endpoint: 6 Month MACE (device related) 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0% 0 0 30 60 90 120 Time (Days from Procedure) N=32 Treated at Baseline 150 180 Secondary Endpoint: LV Volume Reduction by Echo 217 185 156 127 p<0.05 p<0.05 EDV (ml) ESV (ml) Baseline 6M Baseline (N=26), 6M (N=29) Secondary Endpoint: 6 Month Functional Outcomes 6 Minute Walk NYHA 0% (meters) 0% 32% 2.5 2.1 383 53% 361 45% IV III II I 47% p<0.01 Baseline 23% 6M 0% Baseline Baseline (N=32), 6M (N=31) 6M p=ns Baseline 6M Baseline (N=32), 6M (N=29) 6 Month Repeat HF Hosp. + Death 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 12.5% 0.1 0 0 30 60 90 120 Time (Days from Procedure) N=32 Treated at Baseline 150 180 6 Month Mortality and Morbidity 1 0.9 0.8 0.7 0.6 0.5 0.4 0.3 15.6% 0.2 0.1 0 0 30 60 90 120 Time (Days from Procedure) 150 N=32 Treated at Baseline, Morbidity = hosp. for HF, MI, and stroke 180 Conclusions • Heart Failure patients have a very high hospitalization and mortality rate • The Parachute procedure has shown to be a safe procedure • Data trends continue to show improved outcomes for ischemic heart failure patients receiving the Parachute