Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
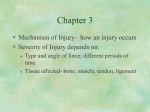
Last Modified: 7/31/2014 OFFICE VISITS & CONSULTS - Audit Tool Patient Name MRN New Patient Office Visit = 9920x Billed Audited Established Patient Office Visit = 9921x Auditor Office Consult = 9924x HISTORY HPI ROS ☐ ☐ Location (site on body) ☐Quality (characteristic: throbbing, sharp; how the problem feels, looks, behaves: acute, chronic, stable, worsening, waxing/waning) ☐Severity (1/10, intensity) ☐Duration (how long for problem/episode) ☐Timing (when it occurs: throughout the day, morning, at night continuously, etc) ☐Context (under what circumstances does the patient experience the symptom/problem) ☐Modifying Factors (what makes it better or worse) ☐Assoc. Signs/Symptoms (what else is happening when it occurs) Status of Chronic Conditions ☐ 1-2 ☐3 ☐Constitutional (Fevers, chills, weight change, fatigue, general health-feeling okay, sweating, appetite) ☐Eyes (Wears glasses, blurry vision, eye problems) ☐Ear, Nose, Mouth, Throat (Hearing loss, ringing in ears, earaches, drainage, sinus problems, nose bleeds, bad breath, sores or bleeding in mouth, voice change, snoring) ☐Cardiovascular (Chest pain, chest tightness, swelling of feet or hands, palpitations, no edema) ☐Respiratory (Cough, SOB, wheezing, sputum, coughing up blood) ☐GI (Change in bowel habits, nausea, vomiting, diarrhea, constipation, belly pain, rectal bleeding) ☐GU (Frequency, pain or burning on urination, change in force when urinating, blood in urine, incontinence, pain with menstruation, change in menstrual habits, testicle pain) ☐Musculo (Joint pain or stiffness, swelling, muscle pain, back pain, difficulty walking, gait) ☐Integumentary - Skin/Breast (Rash, itching, change in skin color, varicose veins, breast pain, lump) ☐Neuro (Headaches, lightheadedness, dizziness, tremors, numbness or tingling, weakness, paralysis) ☐Psych (Memory loss, confusion, suicidal ideation, depression, anxiety, hallucinations, behavior problems) ☐Endocrine (Excessive thirst or urination, heat or cold intolerance, dry skin, night sweats) ☐Hem/lymph (Bleeding or easy bruising, anemia, phlebitis, enlarged glands) ☐Allergic/Imm (Sneezing, itching eyes, rhinorrhea, nasal obstruction, or recurrent infections) ☐“All others negative” PFSH ☐Past Medical (experiences with illnesses, operations, injuries and treatments, updated medication list and allergies) ☐Family (a review of pertinent family medical events, diseases, and hereditary conditions that may place patient at risk) ☐Social (age appropriate review of past and current activities – employment, use of drugs/alcohol/tobacco, marital status, level of education, sexual history) ☐ History was unobtainable due to ______. HPI ☐ 1-3 ROS ☐ None ☐ 1-3 Or status of 1-2 chronic conditions ☐ ☐1 PFSH ☐ None ☐ None HISTORY LEVEL (choose lowest) Problem Focused ☐ Expanded Problem Focused ☐ ☐ 2-9 ☐ 1-2 (new pt/consult) ☐ (1 if Est pt) ☐ 4+ Or status of 3 chronic conditions ☐ ☐ 10+ ☐ 3 (new pt/consult) ☐ (2-3 if Est pt) Detailed ☐ Comprehensive ☐ ☐ 4+ 1995 EXAM ☐Constitutional (vital signs, general appearance, no acute distress) ☐Hem/lymph/Imm (no lymph nodes palpable) ☐Eyes ☐Ear, Nose, Mouth, Throat (teeth) ☐Cardiovascular (carotids, edema, pedal pulses, capillary refill) ☐Respiratory (percussion/auscultation) ☐GI (GI: no tenderness, HSM, normal bowel sounds ) ☐GU ☐Musculo (clubbing, cyanosis, CVA tenderness) ☐Integumentary - Skin/Breast (rashes, tattoos, piercings) ☐Neuro ☐Psych (affect – alert & oriented) OK to use “negative” or “normal” alone but if “abnormal” details must be added. ☐ Head (Including face) ☐ Chest (including breast/axillae) ☐ Neck ☐ Back # of organ systems/body areas EXAM LEVEL Limited to affected organ system/body area Problem Focused ☐ ☐ Abdomen ☐ Left Arm ☐ Genitalia/groin/buttocks ☐ Left Leg 2-4 Expanded Problem Focused ☐ 5-7 Detailed ☐ ☐ Right Arm ☐ Right Leg 8+ Organ Systems Comprehensive☐ Medical Decision Making Elements A) # OF DIAGNOSIS/MANAGEMENT OPTIONS (Problems to Examining Provider) Self-limited or minor (stable, improved, worsening) = 1 pt each, Max = 2 Est. problem (to examiner) stable, improved = 1 pt each Est. problem (to examiner) worsening = 2 pt ea New problem (to examiner) no additional workup = 3 pt each New problem (to examiner) additional workup = 4 pt each B) AMOUNT AND/OR COMPLEXITY OF DATA TO REVIEW (Data Reviewed by Examining Provider) Points A) Total Points Review and/or order LAB tests 1 Review and/or order RADIOLOGY tests Review and/or order MEDICINE tests 1 1 Discussion of test results with performing physician Decision to obtain old records and/or obtain history from someone other than patient Review & summarization of old records and/or obtaining history from someone other than the patient and/or discussion of case with another health care provider Independent visualization of image, specimen or tracing (NOT simply review of report) 1 1 2 2 B) Total C) RISK OF COMPLICATIONS, MORBIDITY and/or MORTALITY RISK Presenting problems Dx procedures ordered ☐ 1 minor or self-limited (cold, insect ☐ Venipuncture, CXR, EKG, EEG, Min bite, tinea corporis) UA, ultrasound/echo, KOH prep ☐ 2 or more minor; ☐ Physiologic tests NOT under 1 stable chronic problem; Acute stress; Non CV imaging w/ contrast Low uncomp illness/injury (cystitis, sprain, (barium enema); Superficial needle allergic rhinitis) biopsy; skin biopsies ☐ Mild exac of chronic prob; 2 stable ☐ Physiologic tests under stress; chronic prob; Acute illness + system Sx Dx endoscopies NO risk factors; (pyelonephritis, colitis); Acute Deep needle or incisional bx; CV Mod complicated injury (head injury brief loss imaging + contrast; Obtain fluid of consciousness); Undiagnosed new from body cavity problem w/ uncertain prognosis ☐ Severe exac of chronic prob or side ☐ CV imaging + contrast, risk effect of tx; Acute or chronic illness factors; Card electrophysiological High posing threat to life/limb; Abrupt change studies; DX endoscopies + risk neuro status (seizure, TIA, factors; Discography weakness/sensory loss) 1 or less - Minimal ☐ 2 – Limited ☐ 3 – Multiple ☐ 4 – Extensive ☐ B 1 or less - Minimal ☐ 2 – Limited ☐ 3 – Multiple ☐ 4 – Extensive ☐ C Minimal ☐ Low ☐ Moderate ☐ High ☐ SF ☐ Low ☐ Moderate ☐ High ☐ (choose column w/ 2-3 checks or center column) New Office Visit or Consult (need 3 of 3) ☐ PF ☐ EPF ☐D ☐C HISTORY ☐ PF ☐ EPF ☐D ☐C EXAM ☐ SF ☐ SF ☐L ☐M MDM ☐ 1 ☐ 2 ☐ Minor surgery + risk factors; Elective major surgery; Prescription drug therapy/management; Therapeutic nuclear medicine; IV fluids + additives ☐ Elective major surg + risk factors; Emergency major surg; Parenteral controlled sub; Rx requiring intense monitoring; DNR or de-escalation of care A MDM Level LEVEL Management options ☐ Rest, gargle, elastic bandages, superficial dressings ☐ OTC drugs; PT, OT; IV fluids without additives; Minor surgery NO risk factors ☐ 3 ☐ 4 Time Based Billing (in minutes) ☐ 20 ☐ 30 ☐ 45 New Office ☐ 10 ☐ 30 ☐ 40 ☐ 60 Off. Consult ☐ 15 ☐C ☐C ☐H ☐ 5 ☐ 60 ☐ 80 Established Office Visit (need 2 of 3) ☐ PF ☐ EPF ☐D HISTORY ☐ ☐ PF ☐ EPF ☐D EXAM Nurse Visit ☐ SF ☐L ☐M MDM LEVEL ☐ 1 ☐ 2 ☐ 3 ☐ 4 Time Based Billing (in minutes) ☐5 ☐ 10 ☐ 15 ☐ 25 Est Office ☐C ☐C ☐H ☐ 5 ☐ 40 TIME: If ALL responses regarding time are "Yes," billing may be based on time. *If the physician documents total time and suggests that counseling or coordinating care dominates (more than 50%) the encounter, time may determine level of service. Documentation may refer to: prognosis, differential diagnosis, risks, benefits of treatment, instructions, compliance, or risk education. Does documentation reveal total face-to-face time? ☐ Yes ☐ No Does documentation discuss the content of counseling or coordination of care? ☐ Yes ☐ No Does documentation reveal that more than 50% of the time was spent on counseling or coordination of care? ☐ Yes ☐ No