Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biology and consumer behaviour wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Oncogenomics wikipedia , lookup
Frameshift mutation wikipedia , lookup
Genetic engineering wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Gene expression profiling wikipedia , lookup
X-inactivation wikipedia , lookup
Extrachromosomal DNA wikipedia , lookup
Genomic imprinting wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Protein moonlighting wikipedia , lookup
Mitochondrial DNA wikipedia , lookup
Medical genetics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Public health genomics wikipedia , lookup
History of genetic engineering wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Genome (book) wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Point mutation wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Microevolution wikipedia , lookup
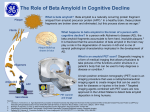
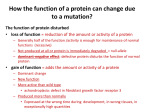
Hereditary Metabolic Disorders Introduction The gene is the fundamental unit of hereditary that carries a single Mendelian trait. A gene consists of proteincoding sequences (exons) interrupted by non-coding sequences (introns). Though they don’t code for protein, introns are important, sometimes acting as regulatory or promoter elements. Sequences of bases arranged in groups of three (codon) code for a specific amino acid, and multiple bound amino acids form a peptide. An allele is one of two or more alternate forms of a gene on a single genetic locus coding for the same protein product. If an individual has identical alleles, they are considered homozygous for a trait. If an individual has different alleles, they are said to be heterozygous. Polymorphism is the occurrence of two or more alleles at a genetic locus within the same population, with at least one minor allele having a frequency greater than 1%. Pseudogenes are defective copies of genes that lack introns and are rarely, if ever, expressed. A mutation is a stable, heritable alteration to DNA. Changes can be gross (chromosome deletion) or minute (point mutation). - - Disease represents a disequilibrium between the organism and environment The environment as well as the inherited characteristics of the organism play a role in disease o Some diseases result only from disorders of inheritance – single gene disease o Some diseases are purely due to the environment Most genetic disorders are related to protein-coding genes (RNA genes that are translated to protein) Few genetic disorders are linked to non-coding RNA genes (RNA genes that are not translated to protein) 1. Be familiar with the basic types of chromosomal disorders Chromosomal disorders - Addition or loss of one or more chromosome, resulting in abnormal chromosome number (aneuploidy) Trisomy (e.g. Trisomy 21, Klinefelter syndrome) Monosomy (e.g. Turner syndrome) – typically lethal - Breakage and loss of a piece of chromosome (deletion) - Breakage of two chromosomes with transfer and fusion of fragments onto each other (translocation) - Abnormal splitting of the centromere so that one arm is lost and one is duplicated (isochromosome) 2. Understand characteristics of the major types of Mendelian disorders Mendelian (monogenic) disorders - Disorders caused by a single mutant gene exhibit one of three simple patterns of inheritance - Autosomal dominant disorders Vertical pattern of inheritance o Mutation clinically manifests when individual has one mutant allele and one normal allele o Each affected individual has an affected parent o Normal children of affected individual will have normal offspring (assuming mate is normal) o Males and females are affected in equal proportions Characteristics of autosomal dominant traits o Delayed onset (e.g. Huntington’s disease) o Variability in clinical expression A 50% deficiency in the mutated gene product causes clinical signs that involve… o Abnormalities in proteins that regulate complex metabolic pathways, including receptors and rate-limiting enzymes (e.g. feline hypercholesterolemia) o Abnormalities in nonenzymatic or structural proteins, including hemoglobin and collagen (e.g. Sickle cell anemia) - Autosomal recessive disorders Horizontal pattern of inheritance o Mutation clinically manifests only when individual is homozygous for the mutant gene o Affected individual has clinically normal parents o Affected individual has affected siblings only o Males and female are affected in equal proportions Characteristics of autosomal recessive traits o The more infrequent the mutant gene is in a population, the stronger the likelihood that affected individuals are the product of consanguine mating (inbreeding) o If both parents are carriers (heterozygous) for the same autosomal recessive gene, 25% of offspring will be homozygous and affected with the disease o If an affected individual mates with a carrier (heterozygote), 50% of offspring will be affected o If two affected individuals mate, all offspring will be affected - X-linked disorders Genes responsible for these disorders are located on the X chromosome Females may be either heterozygous or homozygous for mutant gene (b/c have two X chromosomes) Disorder may demonstrate either recessive or dominant expression Males will be affected if inherit gene, regardless of dominance (b/c have only one X chromosome) Characteristics of X-linked recessive disorders o Pedigree pattern tends to be oblique Trait occurs in maternal uncles of affected males Trait occurs in male cousins descended from mother’s sisters who are carriers o 50% of male offspring from carrier females are affected o All female offspring from affected males are carriers o Affected homozygous females result only when affected male mates with carrier female o Affected males do not transmit the disease to sons o Unaffected individuals do not transmit disorder to any offspring Characteristics of X-linked dominant disorders o Females are affected twice as often as males o Affected female transmits disorder to half her sons and half her daughters (assuming she is heterozygous) o Affected male transmits the disorder to all of his daughters and none of his sons o Disorder is more variable and less severe in heterozygous affected females than in hemizygous affected males (sometimes there is lethality in these individuals) Hemizygous males are those that express an X-linked trait. Because males possess only one X chromosome, they express a single allele of the gene 3. What is genomic imprinting and how does it occur? Genetic imprinting is an epigenetic phenomenon by which certain genes (imprinted genes) are either expressed only from the allele inherited from the mother or only from the allele inherited from the father - Parental imprinting process affects a small number of genes on only a few chromosomes - The purpose of genomic imprinting is to ensure proper embryonic development - There are 4 requirements of biochemical DNA modification for parental imprinting to occur DNA modification must take place prior to fertilization DNA modification must be able to confer transcriptional silencing DNA modification should be transmitted unaltered through mitosis in somatic cells DNA modification should be reversible on passage through the opposite parental germline Mechanisms of imprinting - Site-specific DNA methylation The methylation pattern of a gene correlates with and influences gene expression Current thought is that gene expression decreases with increased methylation Methylation occurs only at the cytosine residue of a cytosine-phosphate-guanidine (CpG) dinucleotide o DNA of sperm is CpG-methylated in a different pattern than the DNA of ova o A maternally-derived gene is more highly methylated than the paternally-derived gene o The methylation pattern changes as the genes passes from females to males and vice versa Recent work suggests that chromatin structure may dictate methylation pattern - Uniparental disomy contributes to the phenomenon of parental imprinting Inheritance of pair of chromosomes from a single parent and none from the other parent - Expansion of an unstable trinucleotide repeat sequence (probably not classified under epigenetics) Normal individuals experience CGG trinucleotide repeats that number from 2-60 When the repeated sequence reaches longer than critical length, they become unstable and can inactivate other genes during DNA replication Affected and carrier individuals may exhibit 60-200 CGG repeats Understand that hereditary disorders can manifest into disruptions of cell and organ function through a variety of mechanisms. These include, mutation-derived alteration of metabolic pathways (e.g. overproduction of uric acid in Gout), disordered feedback regulation of synthetic pathways (e.g. familial hypercholesterolemia), disorders of membrane function (e.g. malignant hyperthermia), disordered intracellular compartmentation (e.g. disruption of signal sequence that allows proper transport of protein through ER), distorted tissue architecture (e.g. RBC shape distortion in Sickle cell anemia resulting from abnormal hemoglobin). 4. What techniques are available to diagnose metabolic diseases? - Identification of accumulated or missing metabolites (using chemical methods, including chromatography) - Direct enzyme assay of blood or fresh tissue - Identification of protein variants (via electrophoresis and immunological procedures for cross-reactivity) - Cell culture studies (using various parameter, including cell hybridization) - Polymerase chain reaction (PCR) Allows identification of a specific DNA sequence present in a given clinical specimen - Molecular biology diagnostic techniques Molecular methods can be used to achieve direct detection of the mutation Establish diagnosis using linkage with negligible recombination (using clone gene as a probe) o DNA probes are capable of detecting small variations in a DNA sequence Establish diagnosis using linkage with detectable recombination o Use Restriction Fragment Length Polymorphism (RLFP) o Identification of RLFP linked to disease genes is useful for DNA diagnosis of disease risk Establish diagnosis based on linkage disequilibrium between genetic markers and disease mutation 6. What techniques are available for the diagnosis of lysosomal storage diseases? - Current diagnostic procedures Enzyme assay Assays for determination of undegraded, stored, or excreted substances Morphologic studies via light and electron microscopy Mass spectrometry - Future diagnostic procedures Direct analysis of genetic disease using gene probes Indirect analysis using RFLPs detected by gene probes Indirect analysis using RFLPs associated with linked DNA segments - Early detection – Prenatal diagnosis in high-risk patients via chorionic villi sampling or cultured amniotic cells - Therapy – enzyme replacement, bone marrow transplantation, and gene therapy may benefit patients 5. What is the specific disorder of membrane function, Malignant Hyperthermia? Describe the pathogenesis. Porcine stress syndrome (PSS) is an inherited malignant hyperthermia that manifests as stress-induced death or acute stress prior to slaughter that results in pale, soft, exudative (PSE) carcasses unfit for market - Underlying cause of PSS is a mutation in the Ca++ release channel protein called ryanodine receptor, an important channel protein that facilitates the release of Ca++ during muscle contraction Two genes encode for two different ryanodine receptors o RYR1 encodes Ca++ release channels on skeletal muscle o RYR2 encodes Ca++ release channels expressed in cardiac muscle and the brain Pathophysiology - In malignant hyperthermia, the abnormal Ca++ release channel is sensitive to lower concentrations of stimulators that induce channel opening. Thus, the channel releases Ca++ at higher rates and does not close readily. Consequently, the cell is flooded with Ca++, causing sustained muscle contraction. This sustained contraction accounts for continuous glycolytic and aerobic metabolism, which generates lactic acid, CO2, heat, and enhanced oxygen uptake - Cell membrane damage and ionic imbalances ultimately account for life-threatening systemic problems - The Malignant hyperthermia (MH) gene is thought to be associated with leanness and muscle hypertrophy Endolysosome System - Comprised of endosomes (early, recycling, late endosomes) and lysosomes essential for a variety of cellular functions, including membrane trafficking, protein transport, autophagy, and signal transduction - Characteristic feature is the acidic pH within the lumen of these organelles (pH is established by ion pumps) pH of 6 within the early endosomes pH of 5.5 within the late endosomes pH of 4.5 within the lysosome - The lysosomal apparatus is the vital digestive and recycling system of cells and performs numerous functions Contains ~40 membrane-bound proteins that function as receptors and transporters Contains 70+ hydrolytic enzymes that participate in cellular and extracellular turnover Involved in post-translational modification of proteins Participates in exogenous antigen processing and presentation Involved in production of hormones (e.g. ACTH, MSH) - The most common cause of lysosomal storage diseases is deficiency of lysosomal enzymes (hydrolases) that results in abnormal storage of catabolic intermediates Accumulation of substrate only occurs when hydrolase activity is below critical threshold o Normal activity of hydrolases is more than 10x higher than critical threshold Acute form of disease results from total absence of enzyme Chronic form of disease is maintained when enzyme activity remains at 5% o Individuals with 10% of normal enzyme activity are not affected, though may be metabolically compromised, and thus referred to as “pseudodeficient” Classification of Lysosomal Storage Diseases - Classification is according to the “major” stored material Mucopolysaccharides, mucolipids, sphingolipids (glycolipids), lipids, glycoprotein, glycogen Note that in many of these disorders, there is lysosomal accumulation of more than one type of compound (due to the fact that hydrolases often degrade more than one substrate) - Classification should consider specificity of morphologic changes Although lysosomal enzyme deficiency affects all cells, morphologic changes tend to manifest only in specific cell types o Morphologic manifestation depends not only on enzyme activity but also substrate load (gangliosidosis most severely affect the nervous system, where cells are rich in gangliosides) 7. Lysosomal storage diseases manifest as what types cellular disorders? Defects in mucopolysaccharide degradation - Mesenchymal cells are most often affected - Metabolites of proteoglycans (protein bound to a glycosaminoglycan) accumulate in the extracellular matrix due to deficient activity of specific lysosomal enzymes Glycosaminoglycans include chondroitin sulfate, dermatan sulfate, heparan sulfate, keratan sulfate o Play a role in resilience, water binding, viscosity maintenance, regulation of fibrillogenesis and fibril diameter, cell recognition, cell attachment, and cell permeability Proteins to which they are bound include collagen, elastin, fibronectin, laminin, and plasma membrane Defects in glycoprotein and oligosaccharide degradation - Glycoproteins consist of a peptide backbone with covalently-attached oligosaccharide - Mammalian tissues contain two major groups of glycoproteins O-linked – linkage of Gal-Na to serine or threonine (e.g. blood group compounds, maxillary mucins) N-linked – linkage of GlcNAc to asparagine (e.g. thyroglobulins, IgM) - There are 8 steps in the lysosomal degradation of N-linked oligosaccharide chains of glycoproteins Enzyme hydrolase deficiencies (via mutation) exist at 7 of these steps, resulting in a variety of storage diseases o Common deficiencies of α-fucosidase, β-galactosidase, β-hexosaminidase A and B Defects in glycosphingolipid degradation - Glycosphingolipids consist of ceramide bound to a carbohydrate chain and vary according to these sugar chains Plant-induced α-mannosidosis - Ingestion of specific plant genera induces α-mannosidosis via inhibition of lysosomal and golgi mannosidase - Accumulation of complex oligosaccharides in lysosomes leads to neurological and behavioral disorders Drug-induced lysosomal storage disease (phospholipidosis) - More than 50 drugs (including antidepressant, antianginal, antimalaria and cholesterol-lowing agents) are implicated in the development of phospholipidosis via different mechanisms Inhibition of lysosomal phospholipidase activity Inhibition of lysosomal enzyme transport Enhanced phospholipid biosynthesis Enhanced cholesterol biosynthesis Disorders associated with abnormal transport of miss folding proteins - Major pathways of protein clearance in the cell are performed by both lysosomes and proteasomes - Pathways become compromised with age, resulting in abnormal accumulation of misfolded/aggregated proteins and the development of neurodegenerative diseases (e.g. Huntington’s and Parkinson’s disease) Disorders of lysosome-related organelles - Specialized cell types contain lysosomal-related organelles that share features with lysosomes but have distinct morphology, composition, and/or function Melanocytes contain melanosomes Lymphocytes contain lytic granules Platelets contains delta granules - Abnormal biosynthesis of lysosome-related organelles can result in disease (e.g. Chediak-Higashi Syndrome) Characteristics of Mitochondria - Mitochondria are elongated organelles located in specific cells near a site of high ATP consumption - Mammalian mitochondria contain ~1500 proteins 99% are coded by nuclear DNA (nDNA), synthesized by ribosomes, and transported to mitochondria 1% are coded by mitochondrial DNA (mtDNA) and synthesized by matrix mibosomes - Mitochondria produce most of organism’s cellular energy (ATP) via oxidative phosphorylation (OXPHOS) 8. Explain the unusual inheritance pattern and pathophysiology of inherited mitochondrial disease. Why do these disorders preferentially affect certain tissues? Inheritance of mitochondrial disease - OXPHOS involves ~100 peptides, most of which are encoded by Mendelian-inherited genes of nDNA - 13 peptides are encoded by mtDNA transmitted by a non-Mendelian inheritance All mtDNA is transmitted via maternal inheritance by the ovum during zygote formation Mutation of mtDNA is also transmitted by maternal inheritance Affected mother transmits disease to all offspring, but only her daughters transmit disorder to subsequent generations Mutation of mtDNA - Thought to arise due to the close proximity of mtDNA to OXPHOS mechanisms OXPHOS causes leakage of harmful reactive oxygen species (ROS) - Mutation frequency in mtDNA is much higher than that of nDNA Due to increased susceptibility of mtDNA to oxidative damage Due to the rapidity of replication of mtDNA (10-20x faster than nDNA) - Mutation of mtDNA results in defects in OXPHOS, which produces clinical signs when ATP production falls below the minimum threshold required to maintain normal cellular or tissue function Most severe clinical signs develop in organs most dependant on OXPHOS (e.g. CNS, skeletal muscle, cardiac muscle, kidney, liver) o Neurological signs include nystagmus, cerebral ataxia, seizures, peripheral neuropathy o Cardiac dysfunction manifests as cardiomyopathy o Hepatic disorders include steatosis and cirrhosis - Severity of disorder depends on degree of mtDNA mutation as well as the number of mutated mitochondria Mutation of nDNA leading to inherited mitochondrial disease - Most OXPHOS genes are encoded by nDNA, which codes for peptides that must be synthesized on ribosomes and appropriately transported into mitochondria - Mutation at any point in this process can also result in inherited mitochondrial disease 9. What is amyloid, its particular microscopic appearance, and molecular organization? - Amyloid is a generic term for the group of diverse extracellular protein deposits that have common morphological properties and stain with specific dyes All amyloid exhibits a characteristic appearance of green birefringence (i.e. apple green) under polarized light when stained with congo red dye Major factor responsible for birefringence is the physicochemical aggregation of amyloid fibrils in a crossed β-pleated sheet configuration, which is optically intensified by the congo red staining - There are 15 biochemically distinct forms of amyloid proteins, two of which are most common These two amyloid proteins are associated with primary and secondary amyloidosis Amyloid structure - 95% of amyloid material consists of fibrillar proteins, the type of which varies with specific disease - 5% of amyloid material is P component P component is a pentagonal/doughnut-shaped structure (glycoprotein) with and external diameter of 9 nm and an internal diameter of 4 nm 10. What is amyloidosis, its common forms, and various clinical signs? - Amyloidosis is a group of diseases that involve the deposition of amyloid (similar-appearing proteins) Currently, 20 different disease conditions have been linked to amyloid deposition Deposits consist mostly of non-branching fibrils of indefinite length, 7.5-10 nm in diameter o Fibrils may appear singly, in bundles, or in an interlocking meshwork Primary amyloidosis - Associated with immunocyte dyscrasias - Fibrils are AL (amyloid light chain) protein formed from complete Ig light chains (mostly λ-light chains) - Fibrils are secreted into the circulation by neoplastic plasma cells (in multiple myeloma) B/c these excessive circulating light chains are small, they pass through glomeruli and are excreted in urine where they are known as Bence Jones proteins - Deposits are found sub-endothelially in various organs Secondary amyloidosis - Associated with chronic inflammation (e.g. tuberculosis, viral infection, cancer) - Fibrils are AA (amyloid associated) protein synthesized primarily in the liver Protein is known as SAA (serum amyloid associated) in circulation and has characteristics of an apoprotein of high-density lipoprotein (HDL) Other types of amyloid - Transthyretin – normal serum protein (synthesized by the liver) that binds and transports thyroxin and retinol - β2-microglobulin – component of MHC class I molecules - β2-amyloid protein – found in cerebral plaques of aged individuals and vascular walls of Alzheimer’s patients Localized amyloid deposits occur in several endocrine tumors - Thyroid carcinoma originating from C cells – accumulation of amyloid that is a procalcitonin fragment - Insulin-secreting tumors of β-cells are found to have amyloid - Deposition of islet amyloid polypeptide (IAPP) in β-cells of adult cats with Diabetes mellitus Systemic amyloid deposition - Involve processes that stimulate synthesis/secretion of amyloid precursors and/or inhibit their degradation Most forms of amyloid are derived from a soluble precursor found in the circulation In some cases, there is an increase in the level of normal serum precursors (LA, SAA, β2microglobulin), while in other cases, a genetic defect results in an abnormal precursor protein Conversion of soluble precursors to their insoluble form (amyloid) involves some form of processing or proteolytic degradation. It’s postulated that fibrillogenesis of amyloid takes place near to the site of deposition and that macrophages are involved in the conversion of the precursor proteins to fibrils A new hypothesis regarding the formation of amyloid was recently proposed, suggesting that a mutation in the gene that codes for the fibrillar protein, or changes in the milieu in which the protein is presented leads to the amyloid deposit. Mature proteins must be folded properly in order to circulate and function. However, if the proteins are partially folded due to mutation, or they are out of their normal milieu, they form self-aggregates and deposits. Features of amyloid and amyloid deposition disorders in different tissues - Systemic amyloidosis always features extracellular amyloid deposition b/w parenchymal cells and blood supply Progressive deposition of amyloid fibrils causes tissue discoloration and increased size Thus, deposition affects the consistency and weight of an affected organ - Localization often leads to ischemic and pressure atrophy of the parenchymal cells (especially seen in hepatocytes and myocardial cells) - Cardiac amyloidosis produces restrictive cardiomyopathy, conduction disturbance and arrhythmias - Chronic deposition of amyloid between the glomerular endothelial cells and podocytes eventually alters their selective filtering characteristics, leading to the passage of large amounts of proteins (i.e., albumin) into urine Proteinuria in renal amyloidosis is an important cause of nephrotic syndrome, in which prolonged loss of serum proteins leads to widespread edema, renal failure, and uremia - Gastrointestinal amyloidosis may lead to malabsorption syndrome