Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Epidemiology of metabolic syndrome wikipedia , lookup
Herpes simplex research wikipedia , lookup
Epidemiology wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Non-specific effect of vaccines wikipedia , lookup
Herd immunity wikipedia , lookup
Public health genomics wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Canine parvovirus wikipedia , lookup
Compartmental models in epidemiology wikipedia , lookup
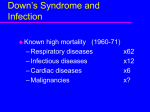
Chapter 16 Pneumococcal Infection 16 Pneumococcal Infection PPV introduced for “at risk” 1996 PCV7 introduced for “at risk” 2002 and as routine 2008 PCV13 replaced PCV7 in 2010 NOTIFIABLE In some circumstances, advice in these guidelines may differ from that in the Summary of Product Characteristics of the vaccines. When this occurs, the recommendations in these guidelines, which are based on current expert advice from NIAC, should be followed. Pneumococcal Infection August 2015 Introduction Streptococcus pneumoniae (pneumococcus) is an important cause of serious infection, especially in young children, older adults and immunocompromised people. Invasive pneumococcal disease (IPD) is defined as the isolation of S. pneumoniae from a normally sterile site (e.g. blood, cerebrospinal fluid (CSF), joint, pleural, or pericardial fluid). IPD is a disease mainly occurring in children under 5 years and those aged ≥65 years. Individuals with severe chronic disease or immunodeficiency are also at increased risk of this disease. Non-invasive manifestations of the disease include otitis media, particularly in children, sinusitis and bronchitis. Although more than 90 polysaccharide capsular serotypes of pneumococci are known, most infections are caused by a limited number of serotypes. In Europe in 2010, the serotypes most commonly implicated were 1, 3, 4, 7F, 8, 12F, 14, 19A, 19F and 22F. The fact that relatively few serotypes cause most invasive disease has allowed for the development of effective vaccines. Epidemiology Pneumococcal infection is a leading cause of death worldwide. Mortality is highest in patients who develop sepsis or meningitis. Pneumococcal 1 Chapter 16 Pneumococcal Infection meningitis case fatality rates of 11-16% were reported in Ireland in the years 2004-2010 and in 2011, a case fatality rate of 9% was reported associated with IPD. Transmission is from person to person by droplet infection or direct contact with respiratory secretions of someone carrying the organism. The incubation period varies by site of infection, and can be as short as 1-3 days. Infection can occur at any time throughout the year but rates peak during the winter months (Figure 16.1). Figure 16.1 Invasive pneumococcal disease (IPD) notifications in Ireland by month, 2007–2012 Pneumococcal Infection August 2015 Source: HPSC Each year the age specific incidence rates (ASIR) are highest among the elderly and young children. A decline in ASIR in the youngest age groups is evident in recent years (Figure 16.2). 2 Chapter 16 Pneumococcal Infection Figure 16.2 Age-specific incidence rates of confirmed invasive pneumococcal disease (IPD) notifications, 2008-2012 Source: HPSC Pneumococcal Infection August 2015 In Ireland PCV7* was recommended for at risk children in 2002 and was introduced into the routine primary immunisation schedule in September 2008, along with a catch up programme for all children under 2 years of age. In December 2010 PCV13** vaccine replaced PCV7 in the Irish childhood immunisation programme. PCV13 includes antigens from the seven serotypes contained in PCV7 plus six additional serotypes which cause IPD. Since the introduction of PCV7 there has been a 91% decrease in the incidence of IPD in young children due to PCV7 serotypes. The additional impact of the introduction of PCV13 should become evident over the next few years. Pneumococcal conjugate vaccines reduce the rates of nasopharyngeal colonisation by vaccine serotypes, thus decreasing the potential for transmission from vaccinated to unvaccinated persons. In the US there has been a significant reduction in the incidence of IPD in the adult population since 2001, following the introduction of PCV to their childhood vaccine schedule. *PCV 7 4, 6B, 9V, 14, 18C, 19F, 23F **PCV 13 1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19 A, 19F, 23F 3 Chapter 16 Pneumococcal Infection In Ireland, since 2008, based on notification data the burden of confirmed cases of IPD in the total population has been reduced by 9%. The greatest reduction have been seen in young children, particularly in those <2 years of age (Figure 16.2). Based on data available from the National Pneumococcal Typing Laboratory, the decrease in this age group can largely be attributed to a significant decline (>76%) in IPD due to serotypes covered by PCV7 between Jan-June 2008 and 2012 (Figure 16.3). Although overall incidence of IPD has decreased compared with 2008, some increase in the burden of illness due to non-PCV7 serotypes has emerged. The impact of the PCV7 vaccine on notifications is evident in the number of confirmed IPD cases in those <2 years of age decreasing from 51 reported in 2008 to 16 cases in 2012. A decline in notifications of disease caused by the additional serotypes included in the PCV13 was not yet evident in 2012. Any change in non-PCV 13 serotypes over time needs to be closely monitored. Figure 16.3 Number of IPD cases in all ages due to serotypes covered by PCV7, PCV13 and non PCV13, 2008-2012. Pneumococcal Infection August 2015 Source: HPSC, from National Pneumococcal Typing Laboratory 4 Chapter 16 Pneumococcal Infection Effects of pneumococcal infection Pneumococcal infection is the most common cause of bacteraemia, septicaemia, bacterial meningitis, pneumonia, sinusitis, and acute otitis media in children. It can also cause periorbital cellulitis, endocarditis, pericarditis, peritonitis, and soft tissue, bone and joint infection. Pneumococcal Infection August 2015 Clinical Risk Groups Persons with the following medical conditions are at risk of pneumococcal infection: • chronic respiratory disease including m a sthma which requires continuous or frequently repeated use of oral steroids m b ronchiectasis m b ronchopulmonary dysplasia (BPD) m c hronic obstructive pulmonary disease (COPD) m c ystic fibrosis m i nterstitial lung fibrosis m p neumoconiosis m r espiratory conditions caused by aspiration • hyposplenia or asplenia (including those with sickle cell and coeliac disease) • immunocompromised by disease or its treatment • neuromuscular disease (e.g. cerebral palsy) with a risk of aspiration In addition smoking, alcohol abuse and exposure to metal fumes also increase the risk of pneumococcal infection. Cigarette smokers are at significantly increased risk of invasive pneumococcal disease. In a US study, the risk for IPD among immunocompetent cigarette smokers aged 18-64 years was four times the risk for controls who had never smoked. Significant dose-response relationships with risk for IPD were also observed for number of cigarettes smoked and pack-years of smoking. Smoking also increases the risk for IPD among other groups, including immunocompromised persons. Individuals with a history of alcohol abuse are 1.6- 7.1 times more likely to develop IPD than the general population. Proposed reasons for the higher risk include increased bacterial colonisation, reduced ciliary motility and immune system compromise. 5 Chapter 16 Pneumococcal Infection There is an association between exposure to metal fumes (e.g. welding) and pneumonia and between welding and invasive pneumococcal disease. Management of cases, contacts, and outbreaks Cases of invasive pneumococcal disease (IPD) Any case of invasive pneumococcal infection or lobar pneumonia believed to be due to S. pneumoniae should prompt a review of the patient’s history to establish whether they are in a risk group and have been vaccinated. Patients with risk factors who have not previously been vaccinated should be given pneumococcal vaccination on discharge from hospital; they should continue vaccination as for other at-risk people (see section on recommendations for the use of pneumococcal vaccination). Pneumococcal Infection August 2015 Contacts of cases Antibiotic prophylaxis is not indicated for close contacts of a case of invasive pneumococcal disease as such contacts are not normally at increased risk of pneumococcal infection. Clusters of invasive pneumococcal disease should be discussed with local Specialists in Public Health Medicine. Outbreaks Outbreaks of pneumococcal infection in hospitals and residential care homes need prompt investigation. Control measures, including vaccination, may be appropriate; these measures should be agreed in discussion with local health-protection or infection-control teams. Pneumococcal vaccines There are two types of pneumococcal vaccine. • Pneumococcal polysaccharide vaccine (PPV23) contains purified capsular polysaccharide from 23 capsular types* of pneumococcus which account for up to 90% of IPD. It is only indicated for those ≥2 years of age; as an adequate antibody response does not develop in those under 2 years of age. • Pneumococcal conjugate vaccine contains polysaccharide antigens from 10 (PCV 10) or 13 (PCV 13) serotypes* conjugated to a protein. (PCV7 is no longer available). These have enhanced immunogenicity to their constituent * The following serotypes are contained in pneumococcal vaccines PCV 7 4, 6B, 9V, 14, 18C, 19F, 23F PCV10 1, 4, 5, 6B, 7F, 9V, 14 18C, 19F, 23F PCV 131, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F, 23F PPV23 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, 33F 6 Chapter 16 Pneumococcal Infection antigens compared with the polysaccharide vaccine, and are immunogenic from 6 weeks of age. Conjugate vaccines are active against 75-90% of serotypes causing IPD, including a significant number of penicillin-resistant strains. The number of doses required for optimum immunogenicity depends on the age and immune status of the recipient. There is a lower response to conjugate vaccines in preterm infants, but the response is adequate to confer significant protection. An up to-date list of licensed vaccines can be accessed on the HPRA website www.hpra.ie A list of the vaccines currently available from the National Cold Chain Service and be found at www.immunisation.ie Pneumococcal vaccines should be stored at +2 to +8oC. Dose and route of administration 1. Pneumococcal Conjugate Vaccine (PCV). The dose is 0.5 ml given by intramuscular injection in the deltoid or the anterolateral thigh. Pneumococcal Infection August 2015 2. Pneumococcal Polysaccharide Vaccine (PPV23). The dose is 0.5 ml given by intramuscular injection in the deltoid. Indications for pneumococcal vaccination. 1. Routine Childhood Pneumococcal Conjugate Vaccine (PCV) The course consists of 3 doses at 2, 6 and 12 months of age. Older children aged 12- <24 months of age who have not received PCV vaccine require 1 dose. For children aged 12-< 24 months, PCV and seasonal influenza vaccine administration should be separated by an interval of at least one week (to decrease the risk of febrile convulsions occurring). PCV is not recommended for children aged over 24 months unless they are in an at risk group (see below). 2. Routine Adult Pneumococcal Polysaccharide Vaccine (PPV23) One dose of PPV23 is recommended for all aged 65 years and older. 3. Clinical Risk Groups The following groups are considered at higher risk of invasive 7 Chapter 16 Pneumococcal Infection pneumococcal disease than the general population and often both PCV and PPV23 are recommended (see Table 16.1). Table 16.1 Clinical risk groups who require pneumococcal vaccination Group A Those at high risk Group B Children at medium risk Group C Adults at medium risk • Asplenia, hyposplenia (including splenectomy, sickle cell disease, haemoglobinopathies, and coeliac disease) 1 • Chronic renal disease or nephrotic syndrome • Chronic renal disease or nephrotic syndrome • Chronic heart, lung, or liver disease • Chronic heart, lung, or liver disease • Complement deficiency (particularly C1-C4) • Immunosuppressive conditions (e.g. some B- and T-cell disorders, HIV infection, leukaemia, lymphoma,) and those receiving immunosuppressive therapies2 • CSF leaks (congenital or complicating skull fracture or neurosurgery) Pneumococcal Infection August 2015 • Intracranial shunt • Diabetes mellitus requiring insulin or oral hypoglycaemic drugs • Down syndrome • Children under 5 years of age following invasive pneumococcal disease • Candidates for, or recipients of, a cochlear implant • Diabetes mellitus requiring insulin or oral hypoglycaemic drugs • Smokers and alcoholics • Individuals with occupational exposure to metal fumes (i.e. welders) • Post haematopoietic stem-cell transplant • Solid organ transplant 1 2 require 2 doses of PCV 2 months apart individuals with primary immunodeficiency may have a suboptimal response to all vaccines. Pneumococcal vaccines are unlikely to be immunogenic in children with primary immune deficiencies involving significant B cell compromise who are receiving regular IVIG replacement therapy. However vaccination should be given as it may have some effect. 3.1 C hildren 2 -<5 years Risk group A: PCV and PPV23 Risk group B: PCV and PPV23 5 - <18 years Risk group A: PCV and PPV23 Risk group B: PPV23 3.2 Adults Risk group A: PCV and PPV23 Risk group C: PPV23 8 Chapter 16 Pneumococcal Infection For vaccine types and schedule see Table 16.2 below. Pneumococcal vaccination should ideally be completed at least 2 weeks prior to elective splenectomy or cochlear implant. Table 16.2 Pneumococcal immunisation for children and adults at increased risk of IPD Age at first vaccination Vaccine type, number of doses and intervals PCV 6 weeks -<12 months Doses 1 & 2 at 2 month intervals Dose 3 at ≥12 months of age, ≥ 2 months after dose 2 PPV23 1 dose given ≥24 months of age, ( ≥2 months after final dose of PCV) 1 or 2 doses1 at 2 month intervals 24 months to 5 years2 1 or 2 doses1 at 2 month intervals 1 dose (≥2 months after PCV) >5- <18 years2 0, 1 or 2 doses1 2 18 and older 0, 1 or 2 doses1 2 1 dose ( ≥2 months after PCV if given) Pneumococcal Infection August 2015 12-<24 months 1 dose of PCV required for all medically at risk over 12 months except when response may be blunted e.g. asplenia/hyposplenia including sickle cell disease, IgA-, IgG subclass- and specific antibody deficiencies. This group needs 2 doses unless they have previously received PCV or PPV23 in which case they need 1 dose of PCV. 1 2 1 dose of PCV13 may be given to at-risk children who have completed a course of PCV7. For those who have received PPV23, wait ≥ 1 year before giving PCV to optimise the immune response. 4. Cases of invasive pneumococcal disease (IPD) Patients with risk factors who have not been vaccinated should be given pneumococcal vaccination before discharge from hospital; they should continue vaccination as for other at-risk people. 9 Chapter 16 Pneumococcal Infection Following IPD in a child under 5 years of age, full blood count, immunoglobulin levels (including IgG sub classes) and complement levels should be checked. All children under 5 years of age who have had IPD, even if not in a clinical risk group, should receive a dose of PCV irrespective of vaccine history followed by a dose of PPV23 2 months later (at or after 2 years of age). Children under 12 months who are unvaccinated or partially vaccinated should complete the routine immunisation schedule followed by an additional dose of PCV 2 months after their 12 month dose and a dose of PPV23 at 2 years of age. Booster doses of PPV23 (see Figure 16.4) Booster doses are not recommended for immunocompetent people aged <65 years because of lack of evidence of improved immunity and evidence of an increased incidence of local side-effects after repeated doses. Pneumococcal Infection August 2015 For individuals whose antibody levels are likely to decline more rapidly, (e.g. asplenia, hyposplenism, and immunosuppression) one booster should be given 5 years after the first dose. Adults 65 years or older should receive a dose of PPV23 if they received PPV23 more than 5 years previously and were less than 65 years of age at the time. Those who received one dose of PPV23 at age 65 or older do not require any further dose regardless of immune status. Contraindications (PCV and PPV23) Anaphylaxis to any of the vaccine constituents. Precautions (PCV and PPV23) Acute severe febrile illness; defer until recovery. PPV23 only. Revaccination within 5 years of a previous dose of PPV23. However, if the vaccine has been given during chemotherapy or radiotherapy, revaccination 3 months after treatment is recommended. 10 Chapter 16 Pneumococcal Infection Pregnancy and breast feeding PPV23 can be given to pregnant women in Group A Table16.1. PCV should be deferred until after delivery as, although is unlikely to result in adverse effects, it has not been evaluated during pregnancy. Adverse reactions PCV Local: Localised tenderness and erythema at the injection site may occur. General: Fever, irritability, decreased appetite, and increased and/or decreased sleep. PPV23 Local: Localised tenderness and erythema at the injection site may occur. Reimmunisation with PPV23 can produce severe local reactions especially if less than 5 years has elapsed since the first injection. General: Occasional low-grade fever lasting less than 24 hours. Pneumococcal Infection August 2015 11 * Asplenia or splenic dysfunction (splenectomy, sickle cell disease, haemoglobinopathies, coeliac syndrome); chronic renal, heart, lung, liver disease, diabetes mellitus, complement deficiency, immunosuppressive conditions; CSF leak, cochlear implant recipients or candidates for implants; post allogeneic bone marrow transplant, solid organ transplant; children < 5 years with history of invasive disease; smokers; alcoholics; individuals with occupational risk due to exposure to metal fumes e.g. welders. ^ Revaccination not indicated for any person who has received a dose of PPV23 at age ≥65 years. ‡ If vaccination has been given during chemotherapy or radiotherapy revaccination 3 months after treatment is indicated. ** Those with asplenia, hyposplenism, immunosuppression including HIV infection, nephrotic syndrome, renal transplant or chronic renal disease. Pneumococcal Infection August 2015 Chapter 16 Pneumococcal Infection Figure 16.4 Pneumococcal polysaccharide vaccination algorithm Adapted from NIO 12 Chapter 16 Pneumococcal Infection Bibliography American Academy of Pediatrics (2012). Red Book: Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics. Centers for Disease Control (2011). Epidemiology and prevention of VaccinePreventable Diseases. Atkinson W, Wolfe S, Hamborsky J, eds. 12th ed. Washington DC: Public Health Foundation. Department of Health, UK (2013) Immunisation against Infectious Diseases (The Green Book) www.dh.gov/uk/greenbook Health Protection Surveillance Centre (2013). Invasive pneumococcal disease publications http://www.hpsc.ie/hpsc/A-Z/VaccinePreventable/ PneumococcalDisease/Publications/ Pneumococcal Infection August 2015 13