Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
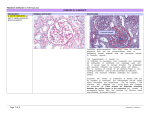
INTEGRATED PATHOPHYSIOLOGY BTECH TEST 1 AUGUST 2007 QUESTION ONE For questions 1.1. – 1.10 refer to the data projector slides (15) QUESTION TWO 2.1 Match the disease characteristics in column A with the correct glomerular disease in column B. A A. Occurs in Goodpasture’s syndrome B. Is associated with a granular immunofluorescent pattern in the basement membrane C. There is interstitial fibrosis and tubular atrophy D. “Rail track” appearance of basement membrane on EM E. Subendothelial deposits of C3 and IgG B MEMBRANOUS GN MESANGIOCAPILLARY GN (TYPE 1& 2) RAPIDLY PROGRESSIVE GN CHRONIC GN ACUTE DIFFUSE PROLIFERATIVE GN (5) 2.2 A clinical study is performed involving subjects with glomerulonephritis. One group of subjects has a diagnosis of crescentic glomerulonephritis and another group has membranous glomerulonephritis. Which one of the following laboratory findings is most likely to be found in the absence of other findings in subjects with membranous glomerulonephritis? a. Rapid onset b. Red blood cell casts c. Oliguria d. Albuminuria e. Hypertension (1) 2.3 Outline the features of nephritic syndrome. (5) 2.4 List three (3) factors that affect the rate of urine production. (3) 2.5 By means of a table match the clinical finding with the appropriate renal syndrome. A A. Recent onset of azotaemia B. Pyuria C. Renal colic D. Asymptomatic haematuria E. prolonged uraemia F. Heavy protienuria B NEPHROTIC SYNDROME CHRONIC RENAL FAILURE URINARY TRACT INFECTIONS ACUTE RENAL FAILURE NEPHROLITHIASIS MILD GLOMERULAR DISEASE (6) 2.6 By means of a pencil sketch indicate the electron microscopy for ADPGN. (4) 2.7 A 50-year-old man is hospitalized for acute myocardial infarction. He has decreased cardiac output with hypotension requiring multiple pressor agents. His urine output drops over the next 3 days. His serum urea nitrogen increases to 59 mg/dL, with creatinine of 2.9 mg/dL. Urinalysis reveals no protein or glucose, a trace blood, and numerous hyaline casts. Five days later, he develops polyuria and his serum urea nitrogen declines. Which of the following pathologic findings in his kidneys is most likely to have caused his azotemia? a. Patchy tubular necrosis b. Fusion of podocyte foot processes c. Glomerular crescents d. Hyperplastic arteriolosclerosis e. Mesangial immune complex deposition 2.8 Discuss the pathogenesis of glomerular nephritis. (1) (15) 2.9 Define the following terms: a. Diffuse glomerulosclerosis (1) b. Interstitial nephritis (1) c. Nephrocalcinosis (1) d. Nephrolithiasis (1) 2.10 Study the diagrams below and answer the questions that follow: A B 2.10.1 The coloured in grey patches indicate areas affected by ATN. Which diagram A or B represents ATN due to shock? (1) 2.10.2 And which represents ATN due to toxicity? (1) 2.10.3 Provide aetiology for 2.10.1 and 2.10.2 (2) 2.11 Discuss the oliguriac phase of ATN. (10) 2.12 A 20-year-old previously healthy man has been feeling tired for the past 5 days. He goes to his physician when he passes dark-colored urine. On physical examination his blood pressure is 155/90 mm Hg. Laboratory studies show his serum creatinine is 4.4 mg/dL. A urinalysis reveals pH 6, specific gravity 1.011, 3+ blood, 1+ protein, no glucose, and no ketones. On urine microscopic examination there are numerous RBC casts. Which of the following pathologic findings on renal biopsy is most likely to be present in this man? a. Glomerular crescents b. Widened proximal tubules c. Polymorphonuclear infiltrates d. Lipiduria e. IgA deposited in glomerular capillaries (1) 2.13 Name the characteristic macroscopy of malignant hypertension in the kidney and provide a pathogenesis for each. (6) 2.14 Discuss the pathogenesis of chronic pyelonephritis. (12) 2.15 List three (3) complications of end stage therapies. (3) [95] ADDENDUM - NORMAL VALUES Creatinine 0.6 - 1.2 mg/dL Glucose Tested after fasting: 70 110 mg/dL Hematocrit Male: 45 - 62% Female: 37 - 48% Hemoglobin Male: 13 - 18 gm/dL Female: 12 - 16 gm/dL Mean Corpuscular Volume (MCV) 76 - 100 cu µm Platelet Count 150,000 - 350,000/mL Potassium 3.5 - 5.0 mmol/L Urea Nitrogen (BUN) 7 - 18 mg/dL Chloride 98 - 106 mmol/L Carbon Dioxide Pressure 35 - 45 mm Hg Sodium 135 - 145 mEq/L White Blood Cell Count (WBC) 4,300 - 10,800 cells/µL/cu mm Thyroid-Stimulating Hormone (TSH) 0.5 - 6.0 µ units/mL Bicarbonate 18 - 23 mEq/L (carbon dioxide content) Osmolality 280 - 296 mOsm/kg water Serum Alkaline Phosphatase 50 - 160 units/L (normally higher in infants and adolescents) (alkaline) Thyroxine (T4), serum Urinalysis Specific gravity pH Protein Glucose Ketone Bilirubin Blood Nitrite Leukocyte Urobilinogen RBCs WBCs RBC CASTS 5-12 ug/dL 64-155 nmol/L 1.002-1.030 5-7 Negative – trace Negative Negative Negative Negative Negative Negative 0.2-1.0 Ehr U/dL 0-2/HPF (High power field) 0-2/HPF (High Power Field) 0/HPF (High power field)