Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Meningococcal disease wikipedia , lookup
Onchocerciasis wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Chagas disease wikipedia , lookup
Schistosomiasis wikipedia , lookup
Leishmaniasis wikipedia , lookup
Leptospirosis wikipedia , lookup
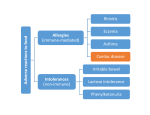
Coeliac disease • Coeliac disease is a permanent intolerance to gliadin the protein component of wheat. It is a lifelong inflammatory condition of the gastrointestinal tract that affects the small intestine in genetically susceptible individuals. Coeliac disease is characterized by malabsorption due to morphological abnormalities in the small intestinal mucosa reversible • These changes are reversible on withdrawal of gluten from the diet. The first detailed description of coeliac disease in children was given in 1887. Classically, coeliac disease is characterized by the development of diarrhoea, loss of appetite, and wasting when a weaning diet containing gluten is introduced, together with secondary effects of malabsorption such as anaemia • Coeliac disease is also known as coeliac sprueâ and it is interesting that the name sprueâ was derived from the Dutch word for aphthous ulcer, this indicating the high proportion of sufferers with oral ulceration adult coeliac disease • In adult coeliac disease, • diarrohea, • weight loss, and weakness are the classic signs and symptoms qiyaastii • Approximately 5-10 per cent of patients with coeliac disease have an affected firstdegree relative. There is also a recognized association of coeliac disease with other autoimmune diseases such as insulindependent diabetes mellitus. Approximately 5-10 per cent of people with this sort of diabetes will also have coeliac disease. diagnosis • Definitive diagnosis of coeliac disease requires the demonstration of characteristic mucosal abnormalities in biopsies of the small bowel (usually obtained via endoscopy Dentists and coelic disease • Dentists may suspect coeliac disease because of enamel defects on permanent teeth—particularly lower incisors. Inflammatory bowel disease (IBD) • The inflammatory bowel diseases are lifelong conditions resulting from aberrant inflammation of the mucosal lining of the gastrointestinal tract. The two main categories are Crohn's disease, which may affect the gut anywhere from mouth to anus, and ulcerative colitis, which is predominantly within the colon. Oral manifestations of coeliac disease • • • • Oral ulceration—RAS Glossitis Angular cheilitis Enamel hypoplasia Clinical features of orofacial granulomatosisâ oral Crohn's disease oral Crohn's disease • Swelling of lips and face* Mucosal tags or cobblestoning Oral ulceration (RAS and non-RAS) Angular cheilitis Lip fissures Persistent lymphadenopathy Perioral erythema and scaling of skin Full-widthâ gingivitis Orofacial swelling • Orofacial swelling, particularly involving the lips, is the most consistent feature of OFG and the most common reason for patients presenting for investigation and treatment. The swelling of the lips • The swelling of the lips is painless, has a firm, rubbery consistency; and can involve both upper and lower lips, individually or together. It can be unilateral or bilateral. crohn”s Disease Buccal mucosa OFG: aetiology and other associations • The aetiology of OFG unrelated to systemic disease remains unclear. However, allergy, infections, and hereditary causes have all been implicated, together with infectious agents such as Mycobacterium paratuberculosis, and ‘ bacteria. Management of OFG • Patients with OFG must be appropriately investigated, not only to confirm the diagnosis but to identify any provoking factors and signs and symptoms, suggestive of an underlying systemic condition, such as CD or sarcoidosis A full range • A full range of haematological and biochemical investigations, including inflammatory markers, should be undertaken, together with an estimation of the serum angiotensin-converting enzyme (ACE) and a chest radiograph. Biopsy of an affected site (usually the labial or buccal mucosa and occasionally the gingivae) should be carried out Patients with OFG • Patients with OFG often seek treatment for lip swelling, which causes distress and embarrassment Treatment • of OFG is unsatisfactory and response to drug-therapy is disappointing treatment • Topical steroids and antiseptic and analgesic mouthwashes can be helpful for managing the oral ulceration, associated with OFG. Angular cheilitis and lip fissures frequently become secondarily infected but in many cases can be improved by the application of an antifungal or antibiotic cream (for example, nystatin, fusidic acid, miconazole), as indicated by microbiology. Ulcerative colitis • Ulcerative colitis is a disease, usually beginning in young adult life, in which inflammatory changes in the colonic mucosa and submucosa lead to widespread ulceration complicated by • This ulceration may be complicated by haemorrhage, perforation, and, occasionally, by the eventual onset of malignancy. Pain, diarrhoea, and generalized abdominal discomfort are the predominant symptoms aetiology • The aetiology of ulcerative colitis is not clear, although it seems to be one of the ‘diseases of civilization’. The treatment of ulcerative colitis is by the use of sulfasalazine and steroids, used either locally. Surgery may be necessary if medical treatment fails. Different B/W • Crohn's disease can affect any part of the gastrointestinal tract. Ulcerative colitis only affects the large bowel. Gastro-oesophageal reflux disorder (GORD) gastro-oesophageal reflux • Healthy individuals experience gastrooesophageal reflux after a meal and this is due to the relaxation of the lower oesophageal sphincter. In patients with gastro-oesophageal reflux disorder (GORD), there is increased frequency and duration of reflux and damage is caused to the oesophageal mucosa by regurgitation of gastric contents • As a result there can be reflux oesophagitis, ulceration, stricture, or epithelial metaplasia (oesophagus). Symptoms of GORD include heart-burn, epigastric pain, and regurgitation. However, some patients, the ‘silent refluxers’, have no symptoms. Drug therapy • Drug therapy is usually successful for GORD and consists of simple antacids (or covering agents), H2 receptor blockers (for example, cimetedine) that inhibit gastric acid secretion, or protonpump inhibitors (for example, omeprazole) that inhibit acid production Surgery • Surgery is rarely indicated but patients who develop oesophageal strictures may need periodic dilatation. Patients with GORD may develop dental erosion particularly of the palatal aspects of the teeth, and, in patients who are asymptomatic, this erosion may be the only indicator of pathological GORD. Patients who regularly chew antacid