Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
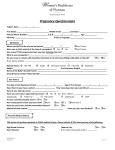
Obstetric New Patient Questionnaire Patient Name: _______________________________________ Age: ___________________ Partner/Father’s Name: ________________________________ Age: ___________________ How did you hear about us? ____________________________________________________________ Occupation: ________________________________Education: ________________________________ Pharmacy, Phone Number: _____________________________________________________________ Primary MD, Phone Number: ____________________________________________________________ Stress Level: low/med/high Office use only: EDD: ________ GA: ______ PPWt: ______ Wt: ______ Ht: ______ BP: ________ Today’s Visit: Current Complaints (i.e. Nausea/Vomiting/Breast Tenderness/Bleeding): _____________________________________________________________________________________________ _____________________________________________________________________________________________ ____________________________________________________________________________________________ Current Medications and Supplements: _____________________________________________________________________________________________ _____________________________________________________________________________________________ _____________________________________________________________________________________________ Allergies to Medication/Food/Latex: ________________________________________________________________ _____________________________________________________________________________________________ Past Surgeries/Hospitalizations: ___________________________________________________________________ _____________________________________________________________________________________________ Diet (i.e. Regular, Vegetarian, Gluten Free, etc.): _____________________________________________________ Exercise (how often): ___________________________________________________________________________ Gynecologic/Obstetrical History: On what date did your last menstrual period start? Are your menses monthly and regular? How many days from the start of one menses to the next? Menses Flow (light, moderate, heavy)? Duration of Flow (days)? At what age did you first get your menses? Current Birth Control Method? What age were you when you had your first child (if applicable)? Abnormal Pap Smear History? If so, explain: How many pregnancies have you had? How many pregnancies have you delivered at full term (>37 weeks)? How many pregnancies have you delivered prematurely (<37 weeks)? How many abortions have you had? How many miscarriages have you had? Have you ever had an ectopic (tubal) pregnancy? Have you ever had twins or triplets? How many children do you currently have living? On what date did you have your first positive pregnancy test? Date of Delivery: MM/DD/YY Weeks Pregnant at time of delivery: Number of hours you labored: Birth Weight of baby: Sex of baby: Mode of delivery (vaginal/forceps/vaccum/csection): Type of anesthesia used (none/IV meds/epidural): Place of delivery (home/birth center/hospital): Preterm Labor (yes or no) Name of baby: Additional Comments: Please circle all problems below that you have ever had and write any details about this problem. Please also indicate any family members who may have these problems. Example: Children, Parents, Siblings, Grandparents, Aunts, Uncles, 1st cousins. Please indicate if maternal or paternal. Alcohol: _______________________________________________________________________ Anemia: _______________________________________________________________________ Anesthetic Complications: ________________________________________________________ Anxiety: ______________________________________________________________________ Arthritis: _______________________________________________________________________ Asthma: _______________________________________________________________________ Autoimmune Disorder (Lupus/Rheumatoid): _________________________________________ Breast Problems: _______________________________________________________________ Caffiene:______________________________________________________________________ Cancer: _______________________________________________________________________ D (Rh) Sensitivity: _______________________________________________________________ Depression/Post-Partum Depression: _______________________________________________ Diabetes: ______________________________________________________________________ Endometriosis: ____________________________________________________________________ GI Problems: _____________________________________________________________________ Gyn Surgery: ___________________________________________________________________ Headaches or Migraines: __________________________________________________________ Heart Disease: _________________________________________________________________ Hepatitis/Liver Disease: __________________________________________________________ History of abnormal Pap smear: ___________________________________________________ History of Blood Transfusions: _____________________________________________________ Hypertension (High Blood Pressure): _________________________________________________ Illicit/Recreational Drug Use: ______________________________________________________ Infertility: _____________________________________________________________________ Kidney Disease/UTI: ____________________________________________________________ Lung Disease: ____________________________________________________________________ Neurologic/Epilepsy: ____________________________________________________________ Operations/Hospitalizations: ______________________________________________________ Ovarian Cancer: ________________________________________________________________ Psychiatric Illness: _________________________________________________________________ Pulmonary (TB/Asthma): _________________________________________________________ Seasonal Allergies: ______________________________________________________________ Thyroid Disorders: ______________________________________________________________ Tobacco use (smoking): __________________________________________________________ Trauma/Violence: _______________________________________________________________ Uterine anomaly/DES Exposure: ___________________________________________________ Varicella immune? (chicken pox): __________________________________________________ Varicose Veins/Phlebitis: _________________________________________________________ When was your last Pap smear: ___________________________________________________ Would you accept blood products: _________________________________________________ Family Genetic History: Patients age at time of delivery: ___________________________________________________ Any history of the following: ______________________________________________________ Thalassemia or are you of Italian, Greek, Mediterranean or Asian decent: __________________ Neural Tube Defects: ____________________________________________________________ Congenital Heart Defects: ________________________________________________________ Down syndrome: _______________________________________________________________ Tay-Sachs (eg, Jewish, Cajun, French-Canadian): _______________________________________ Canavan disease: _______________________________________________________________ Sickle cell disease or trait: _________________________________________________________ Hemophilia or other blood disorder: ________________________________________________ Muscular dystrophy: _____________________________________________________________ Huntington’s Chorea: _____________________________________________________________ Cystic Fibrosis: _________________________________________________________________ Mental Retardation/Autism: ______________________________________________________ If yes, was person tested for fragile X: _______________________________________________ Other inherited genetic or chromosomal disorder: _____________________________________ Recurrent pregnancy loss or stillbirth: _______________________________________________ Medication/Illicit/Recreational Drugs or alcohol since last menstrual period: ________________ If yes, what agent and strength/dosage: _____________________________________________ Any other genetic history: _________________________________________________________ Infection History: Live with someone with or been exposed to TB: _______________________________________ Patient or partner with genital or oral herpes (cold sores/fever blisters): ____________________ Rash or viral illness since last menstrual period: _______________________________________ History of STD: _________________________________________________________________ Do you have any cats: ____________________________________________________________ History of MRSA: ________________________________________________________________ Other infection history: ______________________________________________________________