Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
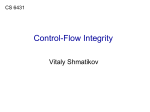
Genetic Mutations Affecting Complement Factor I in Atypical Haemolytic Uraemic Syndrome Introduction Genomic disorders affecting the genes encoding factor H and the factor H related proteins are well described in atypical haemolytic uraemic syndrome (aHUS). In contrast, genomic disorders affecting the gene (CFI) encoding factor I are extremely rare, and have not been previously reported in aHUS. Here, we describe a novel heterozygous deletion of CFI associated with aHUS and present the CFI variants found in the Newcastle cohort of aHUS patients. Methods Sanger sequencing and multiplex ligation-dependent probe amplification (MLPA) were used to screen for CFI variants and genomic disorders, respectively. C3 and C4 were measured by rate nephelometry. Factor H and factor I were measured by radial immunodiffusion. Complement auto-antibodies were screened by ELISA. The breakpoint of the heterozygous deletion involving CFI was defined by microarray, high density SNP genotyping and long range PCR. Results A 36 year old male presented with renal failure, thrombocytopaenia and schistocytes on blood film. A renal biopsy showed thrombotic microangiopathy. Factor I concentration was low. No abnormalities were detected on Sanger sequencing of CFI but further analysis revealed a heterozygous 875,324bp deletion at 4q25 encompassing CFI and ten other genes. The patient undergoes peritoneal dialysis and is now listed for kidney transplantation with eculizumab prophylaxis. We undertook MLPA in 7 other patients with low factor I levels and normal Sanger sequencing of CFI, but did not identify any deletions. In the Newcastle aHUS cohort we have identified 32 different CFI variants in 56 patients. Twenty-seven of the 32 different variants are non-synonymous; the amino acid changes are shown in crystal structure where possible (Fig. 1). Factor I levels in patients with CFI variants are shown (Fig. 2). Thirty-nine percent (22/56) carry, in addition, either a rare variant in another complement gene and/or antibodies against factor H. 1 . 2 . . . Conclusion Genomic disorders affecting CFI in aHUS are extremely rare. However, given the major clinical implications, particularly with respect to transplantation, CFI MLPA should be undertaken as part of routine screening in aHUS.