Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
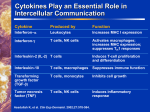
Interleukin-2: Its role in treating HIV infected patients and the possible ways to produce it Acquired immune deficiency syndrome (AIDS) is a disease that is currently a around the world problem including Asia. The human immunodeficiency virus (HIV) bind to CD4 glycoprotein on the surface of CD4 positive cells (CD4+ cells), e.g. helper T cells (CD4+ T cells), macrophages, and causes a decrease in the number of these cells especially CD4+ T cells. The loss of CD4+ T cells lead in turn to failure of proliferation of cytotoxic T cells (CD8+ T cells) and B cells, with eventual loss of immune function and death from opportunistic infection or cancer. Lymphocytes, macrophages, and other cells involved in immune response communicate and exert their effects in part by chemical messengers called cytokines. Interleukin-2 (IL-2) is the cytokine produced mainly by CD4+ T cells, cytotoxic T cells, and natural killer cells (NK cells). Its primary function is to induce proliferation and differentiation of CD4+ T cells and cytotoxic T cells. It also induces B cell proliferation, stimulate macrophage activity, and increase number and toxicity of NK cells. Its production is decreased in HIV infected patients. Thus, exogenous administration is being evaluated in a variety of dosages and route in HIV infected patients. Aldesleukin, a human IL-2 derivative, is a cytokine produced by recombinant DNA techniques. It is a protein of 132 amino acids and has an amino acid sequence closely related to the native human IL-2, differing from the native glycoprotein only by the absence of an N-terminal alanine, the replacement of cysteine 125 with serine, and the absence of glycosylation (Fig.1). Figure 1 Diagram of the amino acid sequences of aldesleukin. Aldesleukin possess immunological activity similar to that observed with native IL-2. It has been approved by the Food and Drug Administration (FDA) for treating metastatic renal cell carcinoma, and metastatic melanoma. It is now in phase III clinical trials in order to determine whether adding IL-2 to standard anti-HIV therapy will help people live longer or preserve the ability to fight off infections. Herein, I will review the clinical aspects of aldesleukin in HIV infected patients, i.e. the findings from clinical trials; indications, precautions, and contraindications; adverse effects; and dose and dosage schedule. Additionally I will review the production aspects of aldesleukin, i.e. production and purification of aldesleukin. Clinical aspects of aldesleukin Highly active antiretroviral therapy has dramatically changed the management of HIV infection. Combination regimens have sharply reduced the incidence of opportunistic infections and HIV related mortality. In some cases, these therapies have allowed for the discontinuation of some prophylactic agents. However, the currently available antiretrovirals are associated with numerous problems, including viral resistance, drug-drug interactions and adverse effects, necessitating the need for newer therapies. Aldesleukin is a promising one. Findings from clinical trials. Immunological benefits like an increase in CD4+cells have been well document in several clinical trials, i.e. increase CD4+ cells without sustained increase in viral load (Table 1). Kovacs et al (1996) compared in HIV infected patients with CD4+ above 200 cells/mm3 receiving interleukin-2 as a 5-day continuous infusion every eight week plus double nucleoside antiretroviral regimen with HIV infected patients receiving only double nucleoside antiretroviral regimen. Dosages ranged from 6 to 18 MIU/day and were adjusted for toxicity. At 1 year, patients in the interleukin-2 group had significant higher CD4+ count (+412 cells/mm3) compared with the control group (-48 cells/mm3). No differences were noted in viral load, although there was a trend for the interleukin-2 group to have a lower viral burden at the end of the study. Subcutaneous injection is similar to intravenous infusion in term of improvement in immunological parameters. In one study, patients with CD4+ count between 200 and 500 cells/mm3 were randomized to receive subcutaneous interleukin-2 at a starting dosage of 7.5 MIU twice daily for 5 days every 8 weeks in combination with antiretroviral therapy, or antiretroviral therapy alone. At 1 year, the mean increase of CD4+ counts in the interleukin-2 group was higher than that in the control group (+384 vs. +64 cells/mm3). Lower dosage of IL-2 (3 MIU/day) is still effective in term of increase CD4+ counts, although it may take longer to reach the CD4+ target number than it would with higher dosages. Duration of intermittent IL-2 therapy appears to be important. A shorter infusion time was evaluated in a randomized trial. Patients were randomized to receive either a 3-day, 4-day, or 5-day continuous infusion of IL-2 plus standard therapy or standard therapy alone. IL-2 was administered every 8 weeks for 6 cycles. It was found that the 5-day infusion period was associated with the largest increase in CD4+ count. IL-2 plus highly active antiretroviral therapy may reduce the latent reservoir but a larger prospective randomized trial will be necessary to confirm these findings. Finally, a moderate size study in people with very low CD4+ cell counts (below 200) and controlled HIV replication (below 1,000 copies HIV RNA) showed that IL-2 therapy could lead to modest increases in CD4+ cell counts. Results have led the French regulatory agency to approve a Compassionate Use Program for IL-2 for people with low CD4+ cell counts and HIV levels below 1,000. These data, combined with other study results, provided French authorities with enough confidence to make IL-2 more widely available to patients with more advanced-stage HIV disease. The authorities in other countries have taken a more conservative approach and have not approved access to IL-2 in the same way. Despite this, many people manage to get IL2; because once a drug is approved for one clinical use, doctors have the right to use it however they choose. However, private insurance and other payers may not be willing to pay for the drug. Table 1 Clinical Trials of intermittent IL-2 in HIV infected patients. 2 Indications, precautions, and contraindications. IL-2 therapy can be used safely (though with significant side effects) by people at all levels of CD4+ cell counts. There are a number of situations in which IL-2 therapy should be avoided or approached with extreme caution. As a general rule, it is discouraged for people with high detectable viral loads, since IL-2 can at least temporarily cause the viral load to increase even more. People with an active infection (e.g. opportunistic infection) should avoid IL-2 or use it carefully because IL-2 can temporarily produce impaired neutrophil function (reduced chemotaxis). Therefore, anyone with an infection should wait until the condition has resolved before using IL-2. This also applies to people currently on an IL-2 regimen. If patients have an infection, they should consider waiting until it's resolved before starting next IL-2 cycle. If patients are taking IL-2 and develop an infection, they should delay IL-2 therapy until it's resolved. Patients with heart problems should also be cautious since IL-2 decreases blood pressure. Patients on medicine to lower blood pressure should consider either avoiding IL-2 therapy or consider stopping blood pressure medication during the 5-day courses of IL-2. The combination of IL-2 with blood pressure lowering medication could result in dangerously low blood pressure levels that could be fatal. IL-2 should not be used in patients with lung disease. Patients with autoimmune diseases, including Crohn's disease, psoriasis, and rheumatoid arthritis should not use IL-2, or use it with great caution because it may worsen these conditions. There are concerns that IL-2 therapy might also worsen diabetes, so patients with diabetes and patients with signs of insulin resistance should be cautious. Because IL-2 side effects 3 include flu-like symptoms, including fatigue, people experiencing extreme fatigue are encouraged to seek treatment for its cause and delay IL-2 therapy until the condition has resolved. In rare instances, IL-2 has caused hypothyroidism and thus should not be used by patients with thyroid problems. Women who become pregnant must stop IL-2 because it has not been studied in pregnant women and it can raise bilirubin levels that may cause serious harm to the developing child. And also it should be used with caution in children because studies in these groups of patients are just beginning. Adverse effects. The most common side effects of IL-2 therapy are flu-like symptoms found among the vast majority of IL-2 users. This side effect may be lessened by taking antihistamines and ibuprofen before taking IL-2 but some antihistamines may have serious interactions with protease inhibitors. Another relatively common side effect is swelling, redness, or lumps at injection site. Putting an ice pack on the injection site before and after injections can help diminish the development of swelling and bumps. Sometimes these lumps, or nodules at the site of injection, can last as long as a few months and they may even produce a scab. In nearly all cases they go away over time. Other less frequent side effects include sinus congestion, low blood pressure, liver toxicity, swelling due to water retention, nausea and vomiting, diarrhea, peeling skin, changes in mental status, and altered blood levels including albumin, potassium, magnesium, calcium, red blood cells, and platelets. Nearly all side effects diminish quickly when the drug is stopped, usually at the end of a five-day course. If side effects emerge, they are usually worst on the last two or three days of a 5day course. To minimize interference with day jobs, many patients begin their 5-day course of IL-2 on a Wednesday. This plan helps time the worst side effects to occur over a weekend or at a time when the patient is not working. The most serious adverse effect after IL-2 administration in HIV infected patients is capillary leak syndrome (CLS). CLS is characterized by reduced vascular tone and extravasation of plasma proteins and fluid into the extravascular space. CLS results in hypotension and reduced organ perfusion, which may be severe and can result in death. CLS may be associated with cardiac arrhythmias (supraventricular and ventricular), angina, myocardial infarction, respiratory insufficiency requiring intubation, gastrointestinal bleeding or infarction, renal insufficiency, edema, and mental status changes. Dose and dosage schedule. IL-2 is administered subcutaneously with starting doses 9-15 MIU/day, twice daily for 5 consecutive days. This 5-day course is repeated every eight weeks. To manage toxicity and side effects, individuals reduce the daily dose of IL-2 in three MIU increments. For example, if 15 MIU daily schedule is very difficult for an individual to take, then the next 5-day course dose would be 6 MIU twice daily (total daily dose of 12 MIU), for five consecutive days. Unlike antiviral therapy, lowering the dose of IL-2 does not lead to resistance against the drug. Once the target CD4+ cell count has been reached, the time between courses of IL-2 therapy is increased by four-week periods. Patients using subcutaneous IL-2 who fail to achieve CD4+ cell increases over time may attain these increases when they switch to continuous intravenous (CIV) therapy. Early studies of IL-2 involved five-day CIV infusions, every eight weeks. 4 Starting doses ranged from 9-18 MIU, daily. In general, the 15-18 MIU CIV daily doses were not well tolerated. Starting doses of 9-15 MIU were preferred in more recent CIV IL-2 studies. Production aspects of aldesleukin Commercial available aldesleukin (Proleukin) is the product of recombinant DNA technology. When compared to other methods such as stimulation of certain cells in culture with appropriate mitogens, recombinant DNA technology can produce aldesleukin in sufficient quantities for human use and is also less costly to produce. The patent in the U.S. for aldesleukin will expired in the year 2003. There are many steps in the production of aldesleukin. The first step is preparing IL-2 cDNA libraries, i.e. a collection of plasmid cloning vectors carrying complete or incomplete IL-2 cDNA. The procedure is shown in Figure 2. In brief, peripheral blood lymphocytes or Jurkat cells (a type of human leukemic cells) are stimulated with certain mitogens (e.g. phytohemagglutinin) and mRNA is collected. The mRNA is converted to double strand DNA (cDNA) by the actions of reverse transcriptase and Klenow fragment of DNA polymerase I enzyme as shown in Figure 3. Then these cDNAs are ligated in plasmid cloning vector to form IL-2 cDNA libraries. These IL-2 cDNA libraries are used to transform host cells. PBL or Jurkat cells mitogen Collect of mRNA for IL-2 Convert to double strand DNA (cDNA) Join into a plasmid cloning vector IL-2 cDNA libraries Figure 2 Steps in preparing IL-2 cDNA libraries. The second step is screening and identification of IL-2 cDNA clones to identify the colonies of host cells that carry complete IL-2 cDNA. This step was carried out by DNA hybridization technique with an oligonucleotide probe. The positive clones were rescreened with the same oligonucleotide probe. Clones carrying complete IL-2 cDNA were identified and confirmed by restriction enzyme mapping techniques. The third step is cloning complete IL-2 cDNA into M13 vector, a bacteriophage DNA, to produce single strand DNA template for use in the next step. 5 Figure 3 Step in synthesis of cDNA. The forth step is oligonucleotide-directed mutagenesis to engineer the complete IL-2 cDNA in order to get the IL-2 derivative which has suited physical and chemical properties. In this case, they engineered the complete IL-2 cDNA in order to get the IL-2 derivative that has serine residue at amino acid position 125 (while in native IL-2 the residue at this position is cysteine). Native human IL-2 is reported to have three cysteine residues located at positions 58, 105, and 125. IL-2 is in an aggregated oligomeric form when isolated from bacterial cells and has to be reduced with reducing agents in order to obtain a good yield from bacterial extracts. In addition, the purified reduced IL-2 protein is unstable and readily reoxidized upon storage to an oligomeric inactive form. The presence of three cysteines means that upon reoxidation, the protein may randomly form one of three possible intramolecular disulfide bridges, with only one of those being the correct bridge found in the native molecule. Since the disulfide structure of the native IL-2 protein is not known, it is possible to use the present invention to create mutations at codons 58, 105 and 125 of the IL-2 gene and identify which cysteine residues are necessary for activity and therefore most likely to be involved in native disulfide bridge formation. In the same vein, the cysteine residue that is not necessary for activity can be modified so as to 6 prevent the formation of incorrect intramolecular disulfide bridges and minimize the chance of intermolecular disulfide bridges by removal or replacement of the free cysteine residue. The procedure is shown in Figure 4. In brief, M13-IL2 single strand DNA was prepared from M13-IL2 double strand, and it is hybridized with synthetic oligonucleotide primer. When the M13-IL2 single strand carries the sense strand of IL-2 cDNA the primer used is shown where the C nucleotide is changed to the G nucleotide. So the codon at position 125 is changed from cysteine to serine. Then the primer is extended by action of Klenow fragment and the double strand is circularized by action of T4 DNA ligase. The circular DNA is used to transform E. coli. M13-IL2 (double strand) M13-IL2 (single strand) Add synthetic oligonucleotide primer GATGATGCTCTGAGAAAAGGTAATC Add Klenow fragment and dNTPs Add T4 DNA ligase Transform E. coli Figure 4 Oligonucleotide-directed mutagenesis. The fifth step is screening and identification of mutagenized phage plaques to identify clones that contain mutated sequence of IL-2 gene. This step is carried out by DNA hybridization technique and confirmed by digestion with the restriction enzyme DdeI. One positive clone called M13-LW46 was inoculated into a culture of JM103 E. coli to prepare RF-DNA. The sixth step is recloning of the mutagenized IL-2 gene for expression in E. coli. The procedure is shown in Figure 5. In brief, RF-DNA from M13-LW46 clone and Plasmid pTrp3 were digested with the same restriction enzyme, the desired fragments were joined together forming ligated plasmid called pLW46. This plasmid was used to transform E. coli. The presence of this plasmid in the bacterial clone was confirmed by restriction enzyme mapping. The positive clones were collected and used for expression of mutagenized IL-2 gene, i.e. as a factory for the production of aldesleukin. A sample of E. coli K12 strain MM294 transformed with pLW46 was deposited in the American Type Culture Collection, 12301 Parklawn Dr., Rockville, Md. 20852, USA on 26 September 1983 and has been assigned ATCC Number 39,452. Fragment RF-DNA from M13-LW46 + Fragment of plasmid pTrp3 Ligated plasmid called pLW46 Tranform into E. coli Restriction enzyme mapping E. coli transformed with pLW46 Figure 5 Recloning of the mutagenized IL-2 gene for expression in E. coli. 7 Next I will mention briefly the production and purification of aldesleukin by growing clones of E. coli transformed with pLW46 in fermenter (Figure 6). In brief, E. coli transformed with pLW46 was grown in appropriate medium. After certain periods of time the medium was changed to that containing a low concentration of tryptophan to increase expression of mutagenized IL-2 gene. The culture material is harvested, concentrated and the cells in the concentrate are broken. Subsequent steps are shown in figure 6. Fermentation of E. coli transformed with pLW46 Harvest Culture Extract into a buffered solution containing sodium dodecyl sulfate (SDS) Reduction, size exclusion chromatography, and oxidation Further purification by reversed phase high performance liquid chromatography Concentration by precipitation Solubilization with a 1% SDS solution Further purification via a size exclusion chromatography Reduce the SDS concentration by diafiltered technique Adjust the concentration of IL-2 by adding Mannitol and phosphate buffer Make is sterile by filtration Aseptically filled into glass vials and lyophilized Figure 6 Steps in production and purification of aldesleukin. Conclusion Aldesleukin, human IL-2 derivative, is produced by recombinant DNA techniques. It has been approved by FDA for treating certain types of kidney and skin cancer. Now, it is in phase III clinical trials in HIV infected patients. In order to put it into the large-scale production we need to explore other points, i.e. principle of microbial growth, maximizing the efficiency of fermentation process, bioreactors, typical large-scale fermentation, harvesting microbial cells, disrupting microbial cells, and downstream processing. References 1. Ganong WF. Review of medical physiology. 18 th ed. Stamford, Connecticut: Appleton & Lange; 1997. 2. Hardman JG, Limbird LE, Molinoff PB, Ruddon RW, editors. Goodman & Gilman’s The pharmacological basis of therapeutics. 9th ed. n.p. : McGraw-Hill; 1996. 3. Piscitelli SC, Bhat N, Pau A. A risk-benefit assessment of interleukin2 as an adjunct to antiviral therapy in HIV infection. Drug Saf 2000; 22(1): 19-31. 8 4. McEvoy GK, editor. AHFS drug information. Bethesda : American Society of Hospital Pharmacists; 1999. 5. Mark DF, Lin LS, Lu SY. Human recombinant interleukin-2 muteins. US patent 4,518,584. May 21, 1985. 6. Project Inform. Interleukin-2 (IL-2, Proleukin) [online]. Available from: http://www.projinf.org/fs/IL2.html [Accessed 2000 June 12]. 7. National Library of Medicine. IGM Full Record Screen: Aldesleukin [online]. Available from: http://130.14.32.45/cgi-bin/VERSION_A/IGMclient?18263+detail+2 [Accessed 2000 June 17]. 8. Glick BR, Pasternak JJ. Molecular biotechnology: principles and applications of recombinant DNA. 2nd ed. Washington, DC: ASM Press; 1998. 9