Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
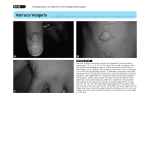
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES BANGALORE, KARNATAKA ANNEXURE-II APPLICATION FOR REGISTRATION OF SUBJECT FOR DISSERTATION 1. NAME OF THE CANDIDATE DR. SAGAR S JAMBAGI. & ADDRESS DEPARTMENT OF PEDIATRICS, FATHER MULLER HOMOEOPATHIC MEDICAL COLLEGE AND HOSPITAL, UNIVERSITY ROAD,DERALAKATTE, MANGALORE-574160. KARNATAKA. PERMANENT ADDRESS DR. SAGAR S JAMBAGI. S/O SURYA NARAYAN JAMBAGI. “BANNI BHAVANI BHAVAN”, H. NO: 9-587/ 1/2A 142, KAILAS NAGAR, GULBARGA-585101. KARNATAKA. 2. NAME OF THE FATHER MULLER HOMOEOPATHIC INSTITUTION MEDICAL COLLEGE AND HOSPITAL, DERALAKATTE, MANGALORE-574160. KARNATAKA. 3. 4. COURSE OF THE STUDY & M .D.(HOM) SUBJECT HOMOEOPATHIC PEDIATRICS DATE OF ADMISSION TO 20-06-2009. THE COURSE 5. TITLE OF THE TOPIC: EFFECTIVENESS OF HOMOEOPATHIC TREATMENT MOLLUSCUM CONTAGIOSUM OF PEDIATRIC AGE GROUP. 1 IN 6. BRIEF RESUME OF THE INTENDED WORK 6.1 NEED FOR STUDY: Molluscum contagiosum is one of the viral skin diseases which commonly affect the children. Some study has shown that, it comprises nearly 1% of all the skin diseases and its incidence has increased nearly fourfold during past twenty years. Though it is self limiting disease, some patients need treatment to prevent autoinoculation and complications. Conventional mode of treatment is curettage or cryosurgery which has to be done repeatedly. Moreover the utility of curettage and cryosurgery is limited when the lesions are too small and too many. Formation of scar as a sequel of such treatment is high. In this scenario, homoeopathy has very effective role in treatment of molluscum contagiosum. This system provides a Holistic approach catering to all the spheres of the individual and it strengthens the immune system causing healing from within outwards. Thus, reduces incidence of recurrent attacks. Homoeopathy has a better scope in this field, and much work has to be done in this field. Hence there is need to study in detail the efficacy of homoeopathic treatment of molluscum contagiosum in pediatric age group. 6.2 REVIEW OF THE LITERATURE: DEFINITION: Molluscum contagiosum is a common cutaneous viral infection in children. It is caused by infection with a DNA virus of the Molluscipoxvirus genus.1 2 AETIOLOGY: Molluscum contagiosum is caused by a large brick-shaped DNA poxvirus with an ultra structural resemblance to vaccinia virus.2 Molluscum contagiosum virus (MCV) has four major types based upon DNA analysis: MCV-1, MCV-1a, MCV-2, and MCV-3. MCV-1 is more prevalent than MCV-2.1 Molluscum contagiosum is caused due to Exciting cause and categorized under individual acute disease. In this molluscum contagiosum virus acts as an exciting cause. EPIDEMIOLOGY: Molluscum contagiosum virus infection occurs worldwide and appear specific to humans.3 It commonly affects children and sexually active adults as well as immunocompromised individuals.4 AGE: Molluscum contagiosum is more common in children younger than 5 years of age.5 SEX: Molluscum contagiosum is more common in boys than in girls.5 PREDISPOSING FACTORS: 1. Impaired cellular immunity. 2. HIV infected patients.1 3. Atopic dermatitis.3 3 4. Topical steroids and other topical immunomodulatory drugs.4 MODE OF INFECTION: 1. By direct skin or mucous membrane contact. 2. Bath towels, swimming pools, and Turkish baths. 3. Individuals involved in close contact sports (e.g., wrestling). 4. Koebnerization.3 5. By fomites. 6. Autoinoculation.1,3 INCUBATION PERIOD: The incubation period averages 2-8 weeks, may be maximum for 6 months.6 PATHOGENESIS AND PATHOLOGY: Molluscum contagiosum virus (MCV) enters the basal keratinocyte and increases the rate of cell division to twice that of normal skin, probably by inhibition of normal keratinocyte apoptotic differentiation programmed by specific MCV encoded proteins. In prickle cell layer, mitosis declines as viral DNA synthesis increases. The cellular proliferation produces lobulated epidermal growths that compress the papillae until they appear as fibrous septa between the lobules. The basal layer remains intact. Each cell enlarges in size and the cytoplasm is filled with a large hyaline acidophilic granular mass known as molluscum bodies, which pushes the nucleus to the edge of the cell. These bodies are present in large number in the cavity which appear ear the surface of the 4 center of a fully developed lesion. Inflammatory changes in the dermis are absent or slight. But in lesions of long duration, there may be a chronic granulomatous infiltrate.4 Studies of Cellular kinetics demonstrated three distinct stages of evolution in growth; an early stage, in which epithelium nuclei divide, a middle stage, in which epithelium division diminishes, and a late stage, in which dermal endothelial cells and fibroblasts becomes activated. Inflammatory cells may be present in all three stages.5 HISTOLOGY: Molluscum lesions are acanthomas consisting of hyperplasctic and hypertrophied epidermal cells which proliferate in a downward fashion into the dermis. Cells are filled with intracytoplasmic inclusion bodies, so called Henderson-Paterson bodies, which are eosinophilic ovoid structures in the lower malphighian layer. In the upper epidermis, they become more basophilic and may be as large as 35 µm in diameter.5 CLINICAL FEATURES: 1. The typical lesion of molluscum contagiosum are discrete, dome shaped, umbilicated waxy papules. 2. They may be skin colored, pink or white. 3. A small central punctum frequently is visible.5 4. A lesion starts as a tiny papule and progresses to a size of 5–10mm in 6-12 weeks. 5 5. Small lesions may join to form a plaque (‘agminate form’).4 6. Lesion may appear vesicular because of a translucent quality. 7. The size may vary from 1 to 5mm, few lesions can occur as large as 10 to 15 mm called as giant molluscum.5 8. Lesions can occur anywhere on the body, but mostly on face, axillae, sides of trunk and genitalia in children. Palms and soles are rarely involved.6 9. The disease usually lasts for 6 to 9 months, although individual lesions persist for only about 2 months.7 10. Lesions usually resolute spontaneously by forming erythema, pus and crusting. 11. Eczematous dermatitis occurs around the molluscum in 10% of cases known as molluscum dermatitis. 12. Multiple and widespread lesions are reported in atopic individuals and in immunosuppressed. 13. Lesions on eyelids may produce conjunctivitis and/ or keratitis.6 DIAGNOSIS: 1. The diagnosis of molluscum contagiosum is usually established on the basis of clinical appearance alone.8 2. Smears, made from the cheesy material expressed from the lesion is crushed between two slides and stained with Giemsa and Wright’s stain show homogenous pear-shaped molluscum bodies. 3. Skin biopsy reveals Henderson-Paterson bodies.6 6 DIFFERENTIAL DIAGNOSIS: 1. Varicella.3,5 2. Verrucae. 3. Juvenile xanthogranuloma. 4. Folliculitis. 5. Furunculosis. 5 6. Lichen planus. 7. Plain warts.4 8. Chickenpox.8 COMPLICATIONS: 1. Pruritus is sometimes a significant problem, particularly in those patients with underlying atopic dermatitis. 2. Chronic conjunctivitis and punctuate keratitis may develop in patient with eyelid lesions. 3. Secondary bacterial infection can occur, particularly if patients scratch their lesions. 3 GENERAL MANAGEMENT: 1. Avoid going to swimming pools, communal baths. 2. Avoid sharing personal items like towels etc.3 PREVENTION: Prevention of spread may be enhanced by avoiding trauma to the site of involvement as well as avoiding scratching. Auto-inoculation may be decreased by treating existing lesions.3 7 HOMOEOPATHIC APPROACH : Homoeopathy is a system of medicine which aims to treat each particular individual be a child or adult.9 It recognizes the individuality of each patient or case. It does not treat disease, it treats patient, in one word individualization.10 It means constitutional treatment based on the totality of the mental and physical reaction. It should be able to cover the level of susceptibility, tendencies, behavioral patterns and the underlying miasms.11 As mentioned in aphorism 5, the physician should consider the probable exciting cause of the acute disease and physical constitution of a patient to cure.12 Hence the physical constitution should never be neglected while arriving at the similimum.13 In molluscum contagiosum, patient develops sensitivity to molluscum contagiosum virus due to disturbances in constitution and weak immune system, which is manifested over the skin as discrete, dome shaped, umbilicated waxy papules. Hence, it requires the constitutional remedy for cure and also to prevent recurrent attacks, simultaneously to strengthen the immune system of the individual. REMEDIES : A few remedies for molluscum contagiosum collected from different repertories are given below: Ambra.; Ars.alb.; Brom.; Bry.; Calc. ar.; Calc. car.; Cal. phos.; Caust.; Con.; Dulc.; Graph.; Hep.; Kali. iod.; Lyc.; Merc.; Nat. mur.; Nit. ac.; Phos. ac.; Phos.; Puls.; Rhus. tox.; Sil.; Staph.; Sulph.; Teucr.; Thuj.11,14-16 8 6.3 OBJECTIVE OF THE STUDY: 1. To assess the effectiveness of constitutional approach in the treatment of molluscum contagiosum in pediatric age group. 2. To analyze group of remedies effective in the treatment of molluscum contagiosum in pediatric age group. 7. MATERIALS AND METHODS: 7.1 SOURCE OF DATA: The subjects will be selected from OPD’s, IPD, peripheral centers, and camps of Father Muller Homoeopathic Medical College, Deralakatte, Mangalore. 7.2 METHOD OF COLLECTION OF DATA: A sample of minimum of 30 cases will be selected purposive sampling method as per the inclusion criteria and will be followed for a minimum period of 2-6 months duration. Every case will be analyzed with reference from materia medica, repertory, and therapeutics whenever required. The potency selection and repetition of the doses will be done according to the demand of the case, with consideration of potency selection criteria such as Acute or Chronic, Susceptibility, Vitality and Suppression (if any), changes in structural and functional level and the degree of correspondence to the remedies selected. 9 INCLUSION CRITERIA: 1. The sample on both sexes aged less than 15 years. 2. Diagnostic criteria are mainly based on clinical presentation. EXCLUSION CRITERIA: 1. Cases above 15 years of both sexes. 2. Cases associated with systemic disorders and complications. RESEARCH HYPOTHESIS: Homoeopathic medicines are effective in the treatment of molluscum contagiosum in pediatric age group. NULL HYPOTHESIS: There is no significant improvement among molluscum contagiosum in pediatric age group after homoeopathic treatment. PLAN FOR ANALYSIS The collected date will be analyzed by paired‘t’ test and data will be presented in the form of mean, standard deviation, frequencies and percentages. 7.3 Does the study require any investigations to be conducted on patients, or other humans (or animals)? If so please describe briefly. The diagnosis of molluscum contagiosum is mainly established on the basis of clinical appearance. 10 To confirm the molluscum contagiosum following investigations can be done (If required), Histopathological study. Skin biopsy. 7.4 Has ethical clearance been obtained from your institution in case of 7.3? Yes, enclosed. 11 8. LIST OF REFERENCES: 1. Thappa MD. Clinical pediatric dermatology. Noida, India: Elsevier, A division of Reed Elsevier India Pvt. Ltd; 2009. p. 50. 2. Weedon D. Skin pathology. 2nd ed. China: Churchill Livingstone, an imprint of Elsevier limited; 2005. p. 693. 3. Wolff K, Goldsmith AL, Katz IS, Gilchrest AB, Paller SA, Leffel JD editors. Fitzpatrick’s dermatology in general medicine. 7th ed. USA: MC Graw Hill Companies Inc; 2008. P. 1911–3. (vol 2). 4. Valia GR, Valia RA, IADVL text book of dermatology. 3rd ed. Mumbai, India: Bhalani publishing house; 2008. p. 333. (vol I). 5. Schachner AL, Hansen CR editors. Pediatric dermatology. 2nd ed. USA: Churchill Livingstone; 1995. p. 1278–9. (vol 2). 6. Inamadar CA, Sacchidanand S. Text book of pediatric dermatology. New Delhi: Jaypee Brothers Medical Publishers (P) Ltd; 2009. p. 139. 7. Ruocco E, Donnarumma G, Baroni A, Tufano AM. Bacterial and Viral Skin Diseases. Dermatologic clinics. 2007 October; vol 25(4). P. 671. 8. Jenson BH, Baltimore SR. Pediatric infectious diseases: Principle & Practice. 2nd ed. Philadelphia: W B Saunders Company; 2002. p. 569. 9. Homoeopathy and children. Wonders of homoeopathy. Address: URL: http://wonders of homeopathy.com/homoeopathy for children.html. Accessed on: 24 October 2009. 10. Close S. The genius of homeopathy lectures and essays on homoeopathic philosophy. New Delhi: B Jain Publishers (P) Ltd; 2004. p. 51. 12 11. Tiwari SK. Homoeopathy child care therapeutics, child types, repertory. New Delhi: B Jain Publishers (P) Ltd; 2004. p. 28. 12. Hahnemann S. Organon of medicine. 6th ed. New Delhi: Indian Books & Periodical Publishers; 2004. p. 91–2. 13. Jain BP. Essentials of pediatrics. Maharastra: Nitya Publications; 1992. p. 13. 14. Boericke W. Pocket manual of homoeopathic materia medica with Indian medicine and repertory. New Delhi: Indian Books & Periodicals Publishers; 2006. p. 910. 15. Murphy R. Homoeopathic medical repertory, a modern alphabetical repertory. New Delhi: Indian books & periodical syndicate; 1994. p. 582. 16. Bakshi PJ. The phoenix repertory. New Delhi: Cosmic Healers Pvt Ltd; 1999. p. 1976. (vol 2). 13 9. SIGNATURE OF THE CANDIDATE 10. REMARKS OF THE GUIDE 11. NAME & DESIGNATION OF (IN BLOCK LETTERS) 11.1 GUIDE DR. SHASHIKANT TIWARI. D.M.S., Dip.N.I.H. PROFESSOR, FATHER MULLER HOMOEOPATHIC MEDICAL COLLEGE & HOSPITAL, DERALAKATTE, MANGALORE. 11.2 SIGNATURE 11.3 CO-GUIDE 11.4 SIGNATURE 11.5 HEAD OF THE DR. JYOSHNA S. DEPARTMENT B.H.M.S, M.D (HOM), PROFESSOR, DEPT OF PEDIATRICS, FATHER MULLER HOMOEOPATHIC MEDICAL COLLEGE & HOSPITAL, DERALAKATTE, MANGALORE. 11.6 SIGNATURE 12. 12.1 REMARKS OF THE CHAIRMAN& PRINCIPAL 12.2 SIGNATURE 14