Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
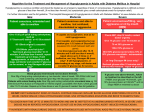
Con Ed Diabetes/PG/AM 26/09/2007 MODULE 15: 12:31 Page 1 Diabetes mellitus GLOBALLY the incidence of diabetes is likely to exceed 250 million people by 2025 – that is a measure of the scale of the problem this condition is likely to present in the future. It is evidence of how diabetes will be one of the foremost public PART 9 Acute complications by Rita Forde THE complications of diabetes can be broadly categorised as acute or chronic, with the latter resulting in the debilitating macrovascular and microvascular conditions. It is these chronic complications that present the greatest cost both in human and fiscal terms. A significant proportion of diabetes care is aimed at preventing these conditions, namely retinopathy, nephropathy, neuropathy and cardiovascular disease. However the acute complications of diabetes can also lead to serious morbidity and mortality. Hypoglycaemia and hyperglycaemic states provide a challenge for the person living with diabetes and the healthcare professionals alike. Hypoglycaemia Clinically hypoglycaemia is defined as a blood glucose level of less than 4mmols/l. For people requiring insulin and sulphonylureas hypoglycaemia is a significant limitation in the management of their diabetes as without it all people with diabetes could have normal glycaemic control over a lifetime of diabetes.2 Hypoglycaemia is the most common acute complication of diabetes, with its onset usually being rapid and the symptoms ranging from very mild to severe enough to cause brain damage or death.3 Falling levels of blood glucose concentration cause an array of signs and symptoms that are triggered by the central nervous system and the sympatho-adrenal system.2 The symptoms of hypoglycaemia are subjective and idiosyncratic but have a fundamental protective role by providing early warning of a fall in blood glucose. The symptoms of hypoglycaemia can be considered as neurogenic (autonomic), neuroglycopenic or non-specific. The neurogenic symptoms are the result of the perception of the physiological changes caused by activation of the central nervous system due to the falling blood glucose level. The neurogenic symptoms are either adrenergic or cholinergic mediated and include tremor, feelings of anxiety and or hunger and sweating. health challenges facing the world in the decades ahead. This month Rita Forde discusses the range of complications that can arise from diabetes and emphasises the importance of not underestimating the psychological implications for patients. Neuroglycopenic symptoms are the result of brain neuronal glucose deprivation. Symptoms range from feelings of warmth and confusion to include seizure activity, loss of consciousness and, if severe and prolonged, brain damage or death may occur. The non-specific symptoms include feelings of nausea and headache.4 The physical signs resulting from the activation of the sympatho-adrenal system include pallor and diaphoresis. These signs are often prominent compared to the more subtle increase in heart rate and blood pressure. Awareness of hypoglycaemia is largely the result of the perceptions of the neurogenic symptoms and the recognition that they are indicative of hypoglycaemia. However the neuroglycopenic symptoms are often the clues recognised by the family and friends of the person with diabetes.2 During a hypoglycaemic episode the intensity of an individual symptom is of greater importance than either the nature or the total number of symptoms in the perception of the low blood glucose level.5 Diagnosis While the clinical presentation of hypoglycaemia can be characteristic the signs and symptoms are often non-specific. It is for this reason that it is recommended to test and record the blood glucose level when hypoglycaemia is suspected.2 A blood glucose reading of less than 4mmols/l is considered a hypoglycaemia event and should be treated accordingly. While there is no grading system for hypoglycaemia it is generally categorised as mild, moderate or severe. Mild hypoglycaemia is one that is easily treated by the individual by the intake of some refined carbohydrate. Moderate hypoglycaemia is when the intervention of someone else is necessary to provide carbohydrate (food or drink) to the person with diabetes as they may display some cognitive impairment. A severe hypoglycaemia means that the individual has altered consciousness or maybe unconscious and requires assistance with treating the episode.6 Treatment Treatment of hypoglycaemia should be initiated immediately once diagnosed. When the person is conscious 15gm of a refined carbohydrate should be taken orally. This can be taken in many forms such as 80ml of regular lucozade, 200ml of orange juice or five dextrose sweets. The blood sugar should be rechecked after 15 minutes and if it remains less than 4mmols/l the above treatment repeated. Oral carbohydrate should only be administered if the person is conscious and coherent. In the event that it is not safe to take carbohydrate orally, 1mg glycogen should be administered subcutaneously or intramuscularly. This treatment can be repeated after ten minutes if the blood glucose level has not risen WIN October 2007 Vol 15 Iss 9 47 Con Ed Diabetes/PG/AM 26/09/2007 12:33 Page 2 Continuing Education Table Counter regulatory hormonal response to at least 4mmols/l. If the hypoglycaemic episode does not resolve following the second glycogen then intravenous glucose is necessary, therefore the person will need to be brought to their local emergency department.6 In the event that a mild to moderate hypoglycaemic episode occurs while the person is hospitalised 15gm of a refined carbohydrate should be administered as described previously. However, if the person is unconscious or not capable of safely taking fluids orally then intravenous dextrose (usually 20ml of dextrose 50%) should be the first line treatment. In the event that this is not possible then glycogen should be administered. The brain is dependent on adequate levels of circulating blood glucose as it requires 120gm-140gm per day to function normally. When the blood glucose level falls below normal the body releases hormones to counteract the effects of hypoglycaemia, known as the counter regulatory response.7 Prevention Hypoglycaemia is a classic example of prevention being better than cure and patient education is fundamental to the avoidance of this potentially life threatening complication of diabetes.5 It is important to appreciate that hypoglycaemia is not caused by diabetes but by the treatment of diabetes. All people requiring insulin and sulphonylureas should receive education in relation to hypoglycaemia. This should include information about the signs and symptoms and also how to treat hypoglycaemia. However strategies to prevent its occurrence are a fundamental component of this education. An awareness of the several risk factors involved should be outlined and the methods to avoid hypoglycaemia explained to all people with diabetes. Risk factors There are many risk factors for hypoglycaemia including5: Insulin excess Too much insulin taken for the carbohydrate being consumed, or insulin taken at the wrong time or the incorrect type of insulin administered. Decreased exogenous glucose Missed meals or snacks or not enough food taken at a meal. Prolonged fasting can also lead to hypoglycaemia. Decreased endogenous glucose production Alcohol can inhibit glycogenolysis Increased glucose utilisation Excessive exercise or activity for the food consumed. Increased insulin sensitivity This can occur after exercise or if the person increases their fitness level or loses weight. It can also be induced by some medications and also by increased temperatures such as very warm weather or following a hot bath or shower. Decreased insulin clearance Occurs as a result of diminished renal function or renal failure. Compromised glucose counter regulation An insulin deficiency or a history of severe or frequent hypoglycaemic episodes can lead to this. In addition intensive diabetes management with a very low glycaemic control can result in a compromised glucose counter regulation system. Hypoglycaemia unawareness This is defined as the reduced ability or failure to recognise hypoglycaemia at the physiological plasma glucose concentration at which warning symptoms would normally occur.8 People with hypoglycaemia unawareness either do not realise that their 48 WIN October 2007 Vol 15 Iss 9 Hormone Glucagon Action Increased glucose output from the liver and muscle (glycogenolysis) Adrenaline and nor adrenaline Enhanced glycogenolysis in liver and muscles Enhanced gluconeogenesis Decreased insulin secretion Causes many of the signs and symptoms of hypoglycaemia Cortisol Mobilises the substrate for gluconeogenesis Growth hormone Acts with glucose and adrenaline to inhibit peripheral glucose utilisation blood glucose level has fallen below normal or they ultimately feel the warning symptoms but at a much lower than normal plasma glucose level.8 Unawareness is thought to be due to reduced sympathoadrenal responses and the resultant reduced neurogenic symptoms to a given level of glucose concentration.2 It is associated with the frequency of hypoglycaemia episodes and their severity. The more episodes experienced by the person or the more severe the episode the greater the risk of hypoglycaemia unawareness in the future.This can be reversed with strict avoidance of hypoglycaemia and early treatment of falling blood glucose levels. However a chronic complication of diabetes, autonomic neuropathy can lead to hypoglycaemia unawareness that is not reversible. Once hypoglycaemic unawareness is suspected the person should receive further education on the avoidance of a low blood sugar level and its treatment. It is imperative that the frequency of home blood glucose monitoring is adequate. More frequent testing will be required especially before driving. If driving for a long distance the blood sugar level should be re-tested periodically. Psychological implications Hypoglycaemia is feared by a significant proportion of people with diabetes as it has a profound effect on quality of life. This is evident in relation to having a hypoglycaemic event while driving, while at work or at any social event. There is also the fear of brain damage or death to be considered. Therefore it is not unusual for people to deliberately have their blood glucose level higher than recommended in an attempt to avoid hypoglycaemia and a potentially embarrassing or unsafe situation. However this compromise in glycaemic control increases the risk of the chronic debilitating complications of diabetes.The psychological implications of diabetes and its management should be considered at all stages of care and education. Hypoglycaemia is an acute complication of the management of diabetes and is defined as a blood glucose level less than 4mmols/l. The symptoms of hypoglycaemia can be considered as neurogenic (autonomic), neuroglycopenic or non-specific and are resultant of a cascade of events triggered by the falling glucose level. All patient education programmes should include strategies to prevent hypoglycaemia in addition to the correct management of it. Loss of awareness of a falling blood glucose level can occur as a result of frequent or severe episodes of hypoglycaemia. The psychological implications of this acute complication of diabetes should not be under estimated. Rita Forde is an advanced nurse practitioner in diabetes at the Mater University Hospital, Dublin References on request from [email protected] (quote: R.Forde WIN 2007; 15(9): 47-48)