Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Coronary artery disease wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Myocardial infarction wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Electrocardiography wikipedia , lookup
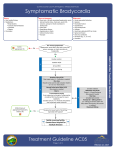
What is the mechanism of complete AV block in inferior MI ? Conduction disturbance is a fairly common occurrence following MI. Inferior STEMI is especially prone for AV blocks. This is because the blood supply to AV nodal tissues and the inferoposterior surface of the heart share the same arterial territory . AV node gets it supply 90% of time by right coronary artery(RCA ) and 10% by LCX. Very rarely from both . The common bradyarrhytmias that we encounter in inferior MI are Sinus bradycardia Sinus pauses ,SA blocks AV blocks Functional Vagotonic Organic Ischemic Necrotic ECG types 1 degree AV block 2 degree AV block – Type 1 Wenke bach Complete heart blcok Mechanisms The inferior aspect of the heart has rich innervation of vagal nerve terminals (While the sympathetic adrenergic system is concentrated in the anterior surface) . The moment infero posterior MI occur it stimualtes the vagus and a prompt bradycardic response occur .Many times the classical hypotension /bradycardia reaction is simply a reflection of heightened vagal tone. Consequence of vagal tone on SA nodal and AV nodal conduction As expected, vagal stimulation can result in a spectrum of arrhythmias from the simple bradycardia to complete SA block to AV block. Extreme bradycardia , may release the junctional pace maker and result in junctional rhythm with a rate of around 40-50. There can be a functional AV dissociation between SA node and AV node. Careful ECG analysis is required here , as it can mimic organic AV block.The simple way to differentiate between organic AV block from simple AV dissociation is to look at the p waves.In AV dissociation both atrial rate and ventricular rate are nearly equal or VR is slightly more than AR .In CHB atrial rate exceeds ventricular rate. SA and AV block occur due to various mechanisms in inferior MI High vagal tone Ischemia of SA/AV node Necrosis of AV node Drug effects -Like morphine Reperfusion bradycardia* Ischemic AV nodal arrhythmias are some times very difficult to differentiate from vagotonia especially if occur within 24h. Irreversible AV nodal block due to necrosis is rare.But if occur , usually associated with extensive inferior mI/RVMI/ .AV block that persist beyond 48-72hours should raise the suspicion of damage to AV node.( As vagal tone is very unlikely;y to last beyond 48h) * Some time a an episode of sudden severe bradycardia can be manifestation of RCA reperfusion.Flushing of SA nodal or AV nodal branch of RCA might trigger this. This has a potential to bring the heart to asystole.The resultant extreme bradycardia often triggers VT/VF .The reported high incidence of primary VF in infero posterior MI is attributed to this sudden RCA perfusion. Medical management for CHB Brady arrhythmia’s due to high vagal tone are generally benign .No specific intervention is required.Atropine will be suffice in most situations.Some times isoprenaline may be required. Aminophyline , now Ivabradine may have a role. Atropine not only corrects the HR it raises the BP also as it counters both cardioinhibitory and vasodepressive limbs of vagal stimulus mediated by acetyl choline . Pacing for Bradycardias in inferior MI. Generally not necessary for sinus bradycardia. Few with CHB require it Persistent hypotension and RVMI needs it often.(Dual chamber temporary pacing preferred as AV synchrony is vital here.) Weaning of temporary pacing in inferior MI. This could be a tricky issue. It can be weaned off in less than a week.A practical way is to use temporary pacing only in back up mode at a heart rate of few beats less than the patients rhythm.Pacing for long hours at high rates may delay the resumption of patients own rhythm and may result in false diagnosis of irreversible CHB and a subsequent PPM How many will require permanent pacing following infero posterior MI ? Only a fraction of patients with CHB require long term pacing . There are some centres tend to overuse PPM in this situation. Wait and watch policy may be the best.A unnecessary lead within a infarcted ventricle has a potential to create problems .There have been occasions a stable RV MI has been destabilised due to RV pacing lead triggered recurrent VF. Tachycardias in inferior MI It is relatively uncommon.Atrial involvement is more common with infero posterior MI and hence a greater incidence of atrial fibrillation . RV MI can induce ventricular tachycardia arising from the RV myocardium