Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
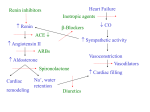
Inotropes in the management of acute heart failure John W. Petersen, MD; G. Michael Felker, MD, MHS, FACC Impaired cardiac contractility is a fundamental component of the heart failure syndrome, initiating the cycle of vasoconstriction, neurohormonal and inflammatory activation, and adverse ventricular remodeling that leads to heart failure progression. Based on this core paradigm, drugs that increase cardiac contractility (positive inotropes) are theoretically appealing as a heart failure therapy, and such agents have been extensively investigated in both acute and chronic heart failure. Although these agents clearly improve cardiac output, their use in heart failure has consistently been associated with increased myocardial oxygen demand, cardiac arrhythmias, and mortality in a variety of clinical settings. Based on these data, the routine use of inotropes as heart failure therapy is not indicated in either the acute or chronic setting. Inotropes may be a necessary evil in a subset of T he term acute heart failure (AHF) encompasses a group of related clinical syndromes broadly defined as new or worsening symptoms or signs of heart failure leading to hospitalization or unscheduled medical care (1). Data from a variety of sources support the idea that AHF is the most common and morbid acute cardiovascular condition in the Western world, with ⬎1 million hospitalizations per year in the United States and a 50% rate of recurrence or death within 6 months (2– 4). Within the broad spectrum of AHF syndromes, there are a variety of clinical presentations (e.g., acute pulmonary edema vs. gradual volume overload) and patient subtypes (e.g., impaired vs. preserved ventricular systolic function) (5). The severity of AHF may range from mild volume overload in the setting of nonadherence to diet or pharmacotherapy to life-threatening cardiogenic shock and multiorgan failure. Var- From the Division of Cardiovascular Medicine, Duke University Medical Center, Durham, NC. Dr. Petersen has not disclosed any potential conflicts of interest. Dr. Felker holds a consultancy with Cytokinetics. For information regarding this article, E-mail: [email protected] Copyright © 2007 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins DOI: 10.1097/01.CCM.0000296273.72952.39 S106 acute heart failure patients, such as those with acute heart failure decompensation in the setting of clinically evident hypoperfusion or shock, or as a bridge to more definitive treatment, such as revascularization or cardiac transplantation. Currently available inotropes, such as dobutamine and milrinone, act (directly or indirectly) by increasing cyclic adenylate monophosphate and therefore intracellular calcium flux. Whether newer inotropes with differing mechanisms of action will realize the potential clinical benefits of inotropic therapy without the risk remains a subject of ongoing investigation. (Crit Care Med 2008; 36[Suppl.]:S106–S111) KEY WORDS: cardiac contractility; heart failure syndrome; cardiac output ious clinical syndromes within the umbrella of AHF may differ significantly with regard to pathophysiology, appropriate clinical care, and outcomes. Despite these differences, several overriding therapeutic goals apply to most patients with AHF. Chief among these are relieving acute symptoms, restoring euvolemia, restoring or preserving end-organ function, limiting length of stay and resource utilization, and decreasing rehospitalization and short-term mortality. No available therapy for AHF is able to achieve all of these goals, but they provide a helpful framework for considering the appropriateness of a given therapy in various patient types. In this review, we discuss the data supporting (or rejecting) the efficacy of inotropic therapy for AHF patients, with an emphasis on applying the principles of evidence-based medicine. Rationale for Inotropic Therapy in Acute Heart Failure Until the 1980s, the predominant framework for understanding heart failure was based on a hemodynamic model. Within this model of heart failure pathophysiology, impaired cardiac contractility and decreases in cardiac output were considered the central abnormalities and thus the most logical target for therapy. This formed the rationale for treatment of heart failure patients with drugs de- signed to increase contractility and cardiac output (positive inotropes). Decades of experience with the use of oral inotropic agents as chronic therapy have shown convincingly that these agents lead to increased mortality in chronic heart failure (6 – 8). The failure of chronic inotropic therapy, coupled with the success of the neurohormonal model of chronic heart failure in guiding the development of angiotensin-converting enzyme inhibitors and -blockers, led to the ascendancy of the neurohormonal model of chronic heart failure and decreased emphasis on hemodynamic considerations and contractility. No chronic oral inotropes are in routine clinical use in the United States, and chronic inotropic therapy is not covered by this review. In contrast to the situation in chronic heart failure, the hemodynamic considerations remain prominent in thinking about AHF syndromes. A decrease in cardiac contractility (e.g., due to ischemia) is often postulated to be the inciting event that leads to a transition from compensated to decompensated heart failure in at least some patients with AHF. The recent European guidelines for the management of AHF state that “the final common denominator in the syndrome of AHF is a critical inability of the myocardium to maintain a cardiac output sufficient to meet the demands of the periphCrit Care Med 2008 Vol. 36, No. 1 (Suppl.) eral circulation” (9). This line of reasoning has resulted in the continued (although controversial) use of intravenous inotropic drugs in selected patients with AHF. As with chronic heart failure, more recent attention has increasingly focused on the role of various neurohormonal pathways (such as the renin-angiotensinaldosterone system, inflammatory cytokines, and natriuretic peptides), the peripheral vasculature, and interactions with other organ systems (such as the kidney) in attempting to understand the pathogenesis of AHF (5, 10). Still, hemodynamic considerations have remained prominent. Here we review the evidence supporting the use of inotropic agents in patients with AHF, the mechanisms of action of available agents, and the development of novel agents with inotropic properties. Which Patients With AHF Should Receive Inotropes? Based on data from the Acute Decompensated Heart Failure National (ADHERE) Registry, 9.6% of patients hospitalized for AHF in the United States receive therapy with an intravenous inotrope (either milrinone or dobutamine) (11). Patients in ADHERE treated with inotropic agents tended to have a clinical profile associated with more severe disease, including lower blood pressure, lower ejection fraction, and higher blood urea nitrogen (11). Is 10% an appropriate utilization of inotropes in a broad population of AHF patients? Given the adverse outcomes seen with inotropic therapy when given chronically to heart failure patients, justification for inotropic therapy in AHF must be based on data supporting the ability of inotropes to achieve important therapeutic goals that cannot be met by other, safer therapies. As noted previously, two shortterm goals of therapy can be defined in the initial management of AHF syndromes: 1. Rapid relief of symptoms (typically dyspnea) by resolution of congestion 2. Maintenance or restoration of adequate end-organ perfusion and function Next, we outline the data addressing the extent to which inotropes address these two short-term goals of therapy in specific patient subtypes. Crit Care Med 2008 Vol. 36, No. 1 (Suppl.) Inotropes in Patients Without Clinical Hypoperfusion Data from large multicenter registries support the idea that the majority of patients presenting with AHF have congestion/volume overload, with relatively preserved end-organ function, normal to elevated blood pressure, and no clinical evidence of shock (3–5). This clinical profile includes patients with both impaired and preserved ejection fraction and probably accounts for ⬎70% of all AHF hospitalizations, although it may be less common in tertiary care centers where advanced disease is more prevalent (5). Since these patients generally have preserved end-organ function, there is little rationale for improving end-organ perfusion with inotropic therapy. Since the main symptom complex of this group of patients involves symptoms of dyspnea and congestion, the primary question in considering inotropic therapy in such patients is “Do inotropes lead to more rapid resolution of symptoms/relief of congestion or earlier discharge?” In contrast to many areas of AHF therapy, the use of an inotropic agent in this patient population has been evaluated in a placebo-controlled, double-blind randomized clinical trial, the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbation of Chronic Heart Failure (OPTIMECHF) study (12). OPTIME-CHF randomized patients with AHF who were not believed to have a clinical indication for inotropic therapy (i.e., patients without evidence of inadequate end-organ perfusion) to 48 hrs of milrinone infusion or placebo. The proposed benefit of inotropes in this population was that inotropic therapy might speed the resolution of acute symptoms, facilitate diuresis, and enable treatment with higher doses of chronic neurohormonal antagonists, such as angiotensin-converting enzyme inhibitors. It was hypothesized that these effects would decrease length of stay and rehospitalization for heart failure. At the time the OPTIME-CHF therapy was designed, use of intravenous milrinone to achieve these putative benefits was increasingly common in the management of AHF in the United States. Review of baseline characteristics of the patients enrolled in the OPTIME study suggests that the trial was generally successful in enrolling a target population representative of most patients with AHF, with a normal mean blood pressure (120/71 mm Hg) and little evidence of end-organ dysfunction (mean creatinine 1.5 mg/dL in the placebo group and 1.4 mg/dL in the treatment group). The primary end point of OPTIME was total number of days hospitalized for cardiovascular causes or within 60 days of randomization. For the purposes of this end point, patients who died during follow-up were considered as hospitalized for the days they were deceased. This end point was chosen based on the hypothesis that milrinone therapy would decrease the length of stay of the index hospitalization and potentially limit rehospitalization. The primary end point did not differ significantly between those randomized to milrinone and those to placebo (median of 6 days for milrinone vs. 7 days for placebo, p ⫽ .71). Other important secondary end points, such as the proportion of patients reaching target doses of angiotensin-converting enzyme inhibitor therapy, did not differ between the treatment groups. Mortality at 60 days (10.3% for milrinone vs. 8.9% for placebo, p ⫽ .41) and 60-day rates of death or rehospitalization (35.0% for milrinone and 35.3% for placebo, p ⫽ .92) were similar between the groups. Randomization to milrinone was associated with more adverse events, with significantly higher incidence of atrial fibrillation or flutter (4.6% vs. 1.5%, p ⫽ .004) and hypotension (10.7% vs. 3.2%, p ⬍ 0.001). Post hoc secondary analyses of the OPTIME data have suggested that the harmful effects of milrinone were primarily seen in those patients with an ischemic etiology of heart failure, potentially due to adverse consequences of milrinone on myocardial oxygen demand or to arrhythmogenesis (Fig. 1) (13). Taken as a whole, the OPTIME data strongly suggest that the routine use of inotropes in patients without evidence of impaired end-organ perfusion is not indicated in AHF. Since such patients represent the majority of AHF patients in the United States, these data suggest a limited role for inotropic therapy in AHF management. Inotropes in Patients With Clinical Hypoperfusion As noted previously, patients with clinical evidence for end-organ hypoperfusion or shock are a minority of patients hospitalized for AHF (probably ⬍10%). This hemodynamic profile, often referred to as a low output state, represents a very high-risk group with significant shortterm mortality (14). Classically, hypotenS107 (%) 50 45 40 35 30 25 20 15 10 5 0 Placebo Milrinone Ischemic Non-Ischemic Figure 1. Rates of death or rehospitalization at 60 days stratified by heart failure etiology and treatment assignment in the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbation of Chronic Heart Failure (OPTIME-CHF) study. p ⫽ .01 for etiology ⫻ treatment interaction. sion has been considered a powerful predictor of low output states, and lower systolic blood pressure on admission has consistently been shown to be a very powerful predictor of adverse outcomes in AHF (15, 16). Importantly, however, clinical exam findings may be inaccurate in identifying patients with low output states, and not all such patients present with hypotension (17). Particularly in patients with long-standing chronic heart failure, low output states may be associated with more subtle clinical signs, such as abdominal pain, nausea, fatigue, and slowed mentation (18). A common clinical finding often believed to be suggestive of marginal or impaired end-organ perfusion is worsening renal function, a finding that often occurs after initiation of AHF treatment with intravenous loop diuretics (so-called cardiorenal syndrome) (19). Although cardiorenal syndrome traditionally was thought to be related to low cardiac output states, more recent data have suggested a much more complex pathophysiology for cardiorenal syndrome, and many such patients appear to have a relatively preserved cardiac output and hypertension (20). Although the results of the ESCAPE trial (21) do not support the routine use of invasive monitoring in AHF, pulmonary artery catheterization may be helpful in distinguishing which patients with low output states may be amenable to treatment with inotropes. In general, inotropic drugs appear effective in increasing cardiac output and improving end-organ perfusion in patients with AHF and diminished cardiac output. The utility of inotropic therapy in restoring end-organ perfusion in these patients is based primarily on clinical experience rather than randomized clinical trial data, given the difficulty in performing randomized clinical trials in this very sick group of patients. Other drugs, such as vasodilators, may also be effective in S108 this clinical scenario and may not be associated with some of the adverse effects of inotropes. Some efforts have been made to directly compare outcomes with vasodilators and inotropes using observational data from large registries, although such analyses are highly confounded by indication (i.e., physicians tend to use inotropic agents in patients with more severe disease). Even after sophisticated statistical adjustment (such as with propensity analysis) for baseline differences, the possibility of unmeasured confounders substantially weakens this type of analysis. Given these caveats, data from the ADHERE registry do suggest worsened outcomes with inotropic drugs compared with vasodilator therapy in AHF patients treated with intravenous vasoactive medications (11). In general, use of vasodilators in this population of patients is often limited by hypotension and may require invasive hemodynamic monitoring in an intensive care setting to be done safely. In patients with significant hypotension, even traditional inotropes, such as milrinone or dobutamine, may be poorly tolerated due to their vasodilatory effects, and peripherally acting agents, such as dopamine, may be transiently required to support the blood pressure during the initiation of inotropic therapy in patients with severe hypotension and cardiogenic shock. If inotropic drugs are used in AHF patients, these agents should be seen as the initial phase of treatment, leading to hemodynamic stabilization and restoration of adequate organ perfusion. If inotropic therapy is not sufficient to restore hemodynamic stability, adjunctive mechanical support (such as with an intraaortic balloon pump) may be required and may be useful even in patients with nonischemic cardiomyopathy. Once short-term hemodynamic stabilization is achieved, an important goal of therapy should be to identify a strategy for tran- sitioning the patient off of inotropic support. This ultimate “destination” for a given patient depends on the clinical scenario. In patients in whom the pathophysiology of hemodynamic compromise is related to potentially reversible insults (such as acute myocardial infarction or fulminant myocarditis), inotropic therapy can serve as a bridge to more definitive therapy (such as revascularization) or recovery. In patients without obvious reversible causes, inotropic therapy can stabilize the patient sufficiently to consider the suitability of other treatments, such as cardiac transplantation or ventricular assist device therapy. In a small number of end-stage patients in whom other therapies are not appropriate, chronic intravenous inotropes may be considered as a palliative option as part of end-of-life care. In sum, use of intravenous inotropes in patients with AHF should be limited to short-term treatment of patients with clinical evidence of impaired end-organ perfusion, with a goal or restoring hemodynamic stability and end-organ function. Choice of Inotropes Mechanism of Action. The most commonly used intravenous inotropes for the management of AHF are dobutamine and milrinone. Both agents increase contractility by increasing intracellular levels of cyclic adenylate monophosphate (cAMP), although they affect cAMP by differing mechanisms. Elevated levels of cAMP lead to increased calcium release from the sarcoplasmic reticulum and increased force generation by the actin-myosin apparatus, with a resulting increase in cardiac contractility. In addition to increasing contractile function, the elevated levels of intracellular calcium resulting from cAMP increases may partially explain the side effects of these agents, especially arrhythmogenesis. Dobutamine increases cAMP production by -adrenergic-mediated stimulation of adenylate cyclase, which leads to cAMP production. Phosphodiesterase (PDE) inhibitors, such as milrinone, increase cAMP levels by blocking the enzyme that breaks down cAMP. Hemodynamic and Clinical Effects. Milrinone and dobutamine have similar hemodynamic effects with some potentially important differences (Table 1) (22). Both agents lead to similar increases in cardiac output and decrease cardiac filling pressures, although milriCrit Care Med 2008 Vol. 36, No. 1 (Suppl.) Table 1. Effects of dobutamine and milrinone on systemic and coronary hemodynamics Dobutamine Milrinone CI HR LVEDP MPAP PVR SAP SVR CSBF MOC 1 1 _ 1 2 + 2 + 2 + 2/1 2 2 + 1 7 1 7 CI, cardiac index; HR, heart rate; LVEDP, left ventricular end-diastolic pressure; MPAP, mean pulmonary artery pressure; PVR, pulmonary vascular resistance; SAP, systemic arterial pressure; SVR, systemic vascular resistance; CSBF, coronary sinus blood flow; MOC, myocardial oxygen consumption. none appears to lower filling pressures to a greater degree than does dobutamine. Milrinone has more significant vasodilatory effects than dobutamine (it is often termed an inodilator), leading to a greater decrease in systemic vascular resistance and systemic blood pressure than is seen with dobutamine. Although both agents can cause tachycardia, dobutamine in general leads to higher heart rates (due to its effects on -adrenergic receptors) than milrinone. Both agents increase myocardial oxygen demand, although dobutamine appears to do so to a greater extent than milrinone. Clinically, there are no high-quality randomized data directly comparing the efficacy of milrinone and dobutamine in patients with AHF. A retrospective analysis of 329 patients admitted with AHF compared the hemodynamic and clinical effects of milrinone vs. dobutamine (23). In this study, there were no differences in baseline characteristics or hemodynamic profiles between the two treatment groups, except for a higher mean pulmonary arterial pressure in the milrinone group (47 mm Hg vs. 42 mm Hg, p ⬍ .001). As compared with dobutamine, milrinone did lead to lower systemic vascular resistance (p ⫽ .01), lower pulmonary artery occlusion pressure (p ⬍ .001), and a larger change in the percentage increase of cardiac index (p ⫽ .03), percentage decrease in pulmonary vascular resistance (p ⫽ .0001), and percentage decrease in mean pulmonary artery pressure (p ⫽ .002). Despite the more favorable hemodynamic response in patients treated with milrinone, there was no statistically significant difference in the inhospital mortality rates between those treated with milrinone (7.8%) or dobutamine (10%) in this small study. The cost of drug was significantly higher in the milrinone group compared with the dobutamine group ($1855 vs. $45, p ⬍ .0001). This cost imbalance, which was primarily related to the costs of the drugs themselves, would be much more comparable between the two therapies today Crit Care Med 2008 Vol. 36, No. 1 (Suppl.) Table 2. Preferred inotrope in different clinical settings Clinical Setting Increased pulmonary artery pressure Need for -blockade Hypotension Renal insufficiency Preferred Inotrope Milrinone Milrinone Dobutamine Dobutamine due to the availability of generic milrinone. In clinical use, hemodynamic differences may influence the choice of one agent or the other for a given patient (Table 2). Due to its greater vasodilator activity, milrinone may be preferred in patients with very elevated filling pressures, in particularly those patients with elevated pulmonary artery pressures. This may be a particular issue for patients being listed for cardiac transplantation, where elevation of pulmonary vascular resistance is a strong relative contraindication to transplantation. Conversely, the use of milrinone may be limited in patients with low blood pressure due to its greater tendency to cause hypotension. The initial hypotensive effect of milrinone may be blunted by beginning at very low infusion rates (0.125 g/kg/min without a bolus). Because it works independently of -adrenergic receptor activation, milrinone retains its hemodynamic effects in the setting of ongoing -blocker therapy. Indeed, some data have suggested more potent hemodynamic effects for milrinone with ongoing -blockade (24). Because milrinone has a relatively long half-life (ⵑ4 – 6 hrs) and is renally cleared, caution must be used with prolonged milrinone therapy in patients with abnormal or changing renal function. Both milrinone and dobutamine increase myocardial oxygen demand and therefore may exacerbate myocardial ischemia. Although dobutamine leads to more sinus tachycardia, both agents carry a significant risk of atrial and ventricular arrhythmias, presumably related to increases in intracellular calcium levels (25, 26). It has also been suggested that inotropes may have direct toxicity to the myocardium. Multiple studies have established the adverse association between elevation of circulating catecholamines and outcomes (27). Indirect data have suggested that exposure to inotropic agents may lead to greater myocardial dysfunction after these agents are discontinued, particularly in those patients with ischemic substrate (28, 29). Newer Inotropes Levosimendan. Despite the limitations of available inotropes, there have been substantial efforts to develop agents that improve cardiac contractility without the adverse consequences of currently available agents. Levosimendan, which has been approved for use in treatment of AHF in Europe, has a primary mechanism of action that differs from that of the -agonists and PDE inhibitors. It is a calcium sensitizer that stabilizes the conformational change in troponin C when it binds to calcium, facilitating myocardial cross-bridging and thus improving contractility (30). At higher doses, levosimendan also inhibits PDE, similar to other PDE inhibitors, such as milrinone. Finally, levosimendan has vasodilator effects through its action on adenosine triphosphate-sensitive potassium channels. Hemodynamic studies of levosimendan in normal volunteers and in patients with heart failure demonstrate its ability to increase cardiac output and lower ventricular filling pressures in a dosedependent manner (31, 32). At therapeutic doses, levosimendan does not appear to have significant effects on myocardial oxygen consumption (33). A phase II study of levosimendan in low-output heart failure, the Levosimendan Infusion or Dobutamine (LIDO) study, randomized 203 patients with AHF who were believed to require invasive hemodynamic monitoring and an inotropic agent (34). Patients were randomized to a 24-hr continuous infusion of levosimendan (24 mg/kg bolus followed by 0.1 mg/ kg/min) or dobutamine (5 mg/kg/min), with a primary end point of the proportion of patients with hemodynamic improvement (defined as a ⱖ30% increase in cardiac output and a ⱖ25% decrease in pulmonary artery occlusion pressure at 24 hrs). A greater proportion of patients S109 in the levosimendan group than in the dobutamine group achieved the primary end point (p ⫽ .022). In this study population, -blockade did not attenuate the favorable hemodynamic effects of levosimendan. Those in the levosimendan group had a greater median number of days alive out of hospital and improved mortality through the first 180 days compared with the dobutamine group. Another phase II investigation in patients with acute myocardial infarction, the Randomized Study on Safety and Effectiveness of Levosimendan in Patients with Left Ventricular Failure after an Acute Myocardial Infarct (RUSSLAN) trial, also suggested that levosimendan reduced mortality and worsening heart failure in patients with AHF and myocardial infarction (35). These initial promising data led to the development of the REVIVE and SURVIVE phase III studies. Data from the phase III REVIVE and SURVIVE studies have been presented but not yet published. The REVIVE program randomized 600 patients with AHF and left ventricular systolic dysfunction to a 24-hr infusion of levosimendan or placebo (36). REVIVE used a unique clinical composite end point, which evaluated the clinical status at 6 hrs, 24 hrs, and 5 days after randomization. The primary end point was the proportion of patients classified as improved at 5 days. This end point was significantly improved by treatment with levosimendan, with 33% more patients in the levosimendan group improving and 30% fewer of them worsening compared with the control group (p ⫽ .015 for both differences). Despite the positive results with regard to the primary end point, potentially significant safety concerns were associated with levosimendan, including a trend toward increased mortality at 90 days (15.1% vs. 11.6% for placebo) and increased rates of hypotension and ventricular arrhythmias. The SURVIVE study compared levosimendan directly with dobutamine in patients with AHF due to left ventricular dysfunction and a clinical indication for inotropic therapy (36). In SURVIVE, 1,327 patients were randomized to infusion of dobutamine or levosimendan, with a primary end point of all-cause mortality at 6 months. There was no significant difference in the primary end point between levosimendan (26% mortality) and dobutamine (28% mortality, hazard ratio ⫽ 0.91, p not significant). The phase III levosimendan experiS110 ence suggests that levosimendan appears to improve symptoms more than placebo in AHF (based on REVIVE) but with worrisome trends toward greater adverse events and mortality (compared with placebo). Based on SURVIVE, levosimendan appears to have similar mortality risk to dobutamine in patients with AHF and a clinical indication for inotropic therapy. Levosimendan is currently approved for use in AHF in Europe but not in the United States. Future development of this agent in the United States remains uncertain. Cardiac Myosin Activators. Given the impairment in cardiac contractile function that is a fundamental feature of the heart failure syndrome, efforts to develop inotropic agents with more favorable safety profiles continue. Recently, insights into the molecular machinery of cardiac contraction have led to the development of a new class of small molecules that work by altering the relationship between actin and myosin. These agents, termed cardiac myosin activators, directly target myocardial myosin adenosine triphosphatase. By increasing the efficiency of actin-myosin cross-bridge formation, these agents may be able to improve contractility without affecting intracellular calcium concentrations. A family of small-molecule myosin activators has been extensively evaluated in animal models, and one drug candidate (CK1827452) has recently begun clinical development in humans with heart failure. Animal data from this agent suggest that it is able to increase the duration of systolic ejection (and therefore the stroke volume) without direct effects on intracellular calcium cycling, myocardial oxygen consumption, the sympathetic nervous system, or PDE activity (37, 38). This appears to result in a significant increase in myocardial efficiency (i.e., greater amount of external work without an increase in energy consumption). Such an agent may possibly allow the clinical benefits of increasing cardiac contractility without the costs in terms of myocardial oxygen demand and arrhythmogenesis. Initial human studies of this potentially promising new agent have recently been reported (39, 40). CONCLUSION AHF is a common, highly morbid condition, with few effective, evidence-based therapies. This situation may explain the persistent use of inotropes in a significant minority of patients who are hospitalized with AHF (41). For the majority of patients with AHF, with normal systemic blood pressure and no clinical evidence of hypoperfusion, there are no data to support a role for inotropic therapy. Although inotropes are often used in patients who develop the cardiorenal syndrome, available data do not support the effectiveness of this therapy, and indeed the emerging profile of patients with cardiorenal syndrome is not generally consistent with a low output state. Inotropic therapy continues to have a role in the short-term stabilization of patients with clear evidence of impaired organ perfusion and low output state. If inotropic therapy is required, selection of a specific agent may depend on aspects of the clinical profile of the patient, including systemic blood pressure, underlying substrate (ischemic vs. nonischemic), and renal function. Despite the lack of general success with inotropic therapy in heart failure, efforts continue to develop novel agents that will realize the potential clinical benefits of increased contractility, but without the costs in terms of arrhythmogenesis and myocardial oxygen consumption. REFERENCES 1. Felker GM, Adams KF, Konstam MA, et al: The problem of decompensated heart failure: Nomenclature, classification, and risk stratification. Am Heart J 2003; 145:S18 –S25 2. Thom T, Haase N, Rosamond W, et al: Heart disease and stroke statistics—2006 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation 2006; 113:e85–151 3. Cleland JGF, Swedberg K, Follath F, et al: The EuroHeart Failure survey programme—A survey on the quality of care among patients with heart failure in Europe: Part 1: Patient characteristics and diagnosis. Eur Heart J 2003; 24: 442– 463 4. Adams J, Fonarow GC, Emerman CL, et al: Characteristics and outcomes of patients hospitalized for heart failure in the United States: Rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 2005; 149:209 –216 5. Gheorghiade M, Zannad F, Sopko G, et al: Acute heart failure syndromes: Current state and framework for future research. Circulation 2005; 112:3958 –3968 6. Massie BM, Berk MR, Brozena SC, et al: Can further benefit be achieved by adding flosequinan to patients with congestive heart failure who remain symptomatic on diuretic, digoxin, and an angiotensin converting en- Crit Care Med 2008 Vol. 36, No. 1 (Suppl.) 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. zyme inhibitor? Results of the flosequinanACE inhibitor trial (FACET). Circulation 1993; 88:492–501 Packer M, Medina N, Yushak M: Hemodynamic and clinical limitations of long-term inotropic therapy with amrinone in patients with severe chronic heart failure. Circulation 1984; 70:1038 –1047 Packer M, Carver JR, Rodeheffer RJ, et al: Effect of oral milrinone on mortality in severe chronic heart failure: The PROMISE Study Research Group. N Engl J Med 1991; 325:1468 –1475 Nieminen MS, Bohm M, Cowie MR, et al: Executive summary of the guidelines on the diagnosis and treatment of acute heart failure: The Task Force on Acute Heart Failure of the European Society of Cardiology. Eur Heart J 2005; 26:384 – 416 Cotter G, Moshkovitz Y, Milovanov O, et al: Acute heart failure: A novel approach to its pathogenesis and treatment. Eur J Heart Fail 2002; 4:227–234 Abraham WT, Adams KF, Fonarow GC, et al: In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: An analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Am Coll Cardiol 2005; 46:57– 64 Cuffe MS, Califf RM, Adams KF Jr, et al: Short-term intravenous milrinone for acute exacerbation of chronic heart failure: A randomized controlled trial. JAMA 2002; 287: 1541–1547 Felker GM, Benza RL, Chandler AB, et al: Heart failure etiology and response to milrinone in decompensated heart failure: Results from the OPTIME-CHF study. J Am Coll Cardiol 2003; 41:997–1003 Nohria A, Tsang SW, Fang JC, et al: Clinical assessment identifies hemodynamic profiles that predict outcomes in patients admitted with heart failure. J Am Coll Cardiol 2003; 41:1797–1804 Felker GM, Leimberger JD, Califf RM, et al: Risk stratification after hospitalization for decompensated heart failure. J Card Fail 2004; 10:460 – 466 Gheorghiade M, Abraham WT, Albert NM, et al: Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006; 296:2217–2226 Shah MR, Hasselblad V, Stinnett SS, et al: Hemodynamic profiles of advanced heart failure: Association with clinical characteristics and long-term outcomes. J Card Fail 2001; 7:105–113 Stevenson LW, Massie BM, Francis GS: Op- Crit Care Med 2008 Vol. 36, No. 1 (Suppl.) 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. timizing therapy for complex or refractory heart failure: A management algorithm. Am Heart J 1998; 135:S293–S309 Forman DE, Butler J, Wang Y, et al: Incidence, predictors at admission, and impact of worsening renal function among patients hospitalized with heart failure. J Am Coll Cardiol 2004; 43:61– 67 Stevenson LW, Nohria A, Mielniczuk L: Torrent or torment from the tubules? Challenge of the cardiorenal connections. J Am Coll Cardiol 2005; 45:2004 –2007 The ESCAPE investigators and ESCAPE study coordinators: Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: The ESCAPE trial. JAMA 2005; 294:1625–1633 Grose R, Strain J, Greenberg M, et al: Systemic and coronary effects of intravenous milrinone and dobutamine in congestive heart failure. J Am Coll Cardiol 1986; 7:1107–1113 Yamani MH, Haji SA, Starling RC, et al: Comparison of dobutamine-based and milrinone-based therapy for advanced decompensated congestive heart failure: Hemodynamic efficacy, clinical outcome, and economic impact. Am Heart J 2001; 142:998 –1002 Bohm M, Deutsch HJ, Hartmann D, et al: Improvement of postreceptor events by metoprolol treatment in patients with chronic heart failure. J Am Coll Cardiol 1997; 30:992–996 Burger AJ, Horton DP, LeJemtel T, et al: Effect of nesiritide (B-type natriuretic peptide) and dobutamine on ventricular arrhythmias in the treatment of patients with acutely decompensated congestive heart failure: The PRECEDENT study. Am Heart J 2002; 144:1102–1108 Benza RL, Tallaj JA, Felker GM, et al: The impact of arrhythmias in acute heart failure. J Card Fail 2004; 10:279 –284 Cohn JN, Levine TB, Olivari MT, et al: Plasma norepinephrine as a guide to prognosis in patients with chronic congestive heart failure. N Engl J Med 1984; 311:819 – 823 Indolfi C, Piscione F, Perrone-Filardi P, et al: Inotropic stimulation by dobutamine increases left ventricular regional function at the expense of metabolism in hibernating myocardium. Am Heart J 1996; 132:542–549 Packer M, Medina N, Yushak M: Hemodynamic and clinical limitations of long-term inotropic therapy with amrinone in patients with severe chronic heart failure. Circulation 1984; 70:1038 –1047 Earl GL, Fitzpatrick JT: Levosimendan: A novel inotropic agent for treatment of acute, decompensated heart failure. Ann Pharmacother 2005; 39:1888 –1896 31. Nieminen MS, Akkila J, Hasenfuss G, et al: Hemodynamic and neurohumoral effects of continuous infusion of levosimendan in patients with congestive heart failure. J Am Coll Cardiol 2000; 36:1903–1912 32. Slawsky MT, Colucci WS, Gottlieb SS, et al: Acute hemodynamic and clinical effects of levosimendan in patients with severe heart failure: Study investigators. Circulation 2000; 102:2222–2227 33. Michaels AD, McKeown B, Kostal M, et al: Effects of intravenous levosimendan on human coronary vasomotor regulation, left ventricular wall stress, and myocardial oxygen uptake. Circulation 2005; 111:1504 –1509 34. Follath F, Cleland JG, Just H, et al: Efficacy and safety of intravenous levosimendan compared with dobutamine in severe low-output heart failure (the LIDO study): A randomised doubleblind trial. Lancet 2002; 360:196 –202 35. Moiseyev VS, Poder P, Andrejevs N, et al: Safety and efficacy of a novel calcium sensitizer, levosimendan, in patients with left ventricular failure due to an acute myocardial infarction: A randomised, placebo-controlled, double-blind study (RUSSLAN). Eur Heart J 2002; 23:1422–1432 36. Cleland JG, Freemantle N, Coletta AP, et al: Clinical trials update from the American Heart Association: REPAIR-AMI, ASTAMI, JELIS, MEGA, REVIVE-II, SURVIVE, and PROACTIVE. Eur J Heart Fail 2006; 8:105–110 37. Anderson RL, Sueoka S, Lee KH, et al: In vitro and in vivo characterization CK1827452, a selective cardiac myosin activator. J Card Fail 2006; 12:S86 38. Shen YT, Vatner SF, Morgans DJ, et al: Activating cardiac myosin, a novel inotropic mechanism to improve cardiac function in conscious dogs with congestive heart failure. J Card Fail 2006; 12:S87 39. Teerlink JR, Malik FI, Clarke CP, et al: The selective cardiac myosin activator, CK1827452, increases left ventricular systolic function by increasing ejection time: Results of a first-in-human study of a unique and novel mechanism. J Card Fail 2006; 12:763 40. Malik F, Teerlink J, Escandon R, et al: The selective myosin activator, CK-1827452, a calcium independent inotrope, increases left ventricular systolic function by increasing ejection time rather than the velocity of contraction. Circulation 2006; 114:441 41. Hauptman PJ, Schnitzler MA, Swindle J, et al: Use of nesiritide before and after publications suggesting drug-related risks in patients with acute decompensated heart failure. JAMA 2006; 296:1877–1884 S111