Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
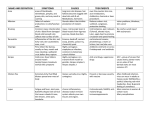
Herpes virus infection and prophylaxis Introduction Clinical neonatal herpes is uncommon in Australia. Data from the Australian Paediatric Surveillance Unit (APSU) gives an incidence of 3.4 - 8 /100,000 live births. In the USA the incidence is higher, between 15 48 /100, 000 1 . In the UK the incidence is 1.7/100,000 2 . A 3 year prospective Canadian study reported an incidence of 5.9/100,000 with the majority of cases (62%) being due to Herpes Simplex type 1 3 . This is also the case in Australia 4 . In the prospective Canadian study 40% of the cases of neonatal herpes had no history of genital herpes before delivery 3 . The following table summarises the risk by maternal presentation 5 . Note that a primary infection includes first infection by type 1 or type 2 virus in a woman who has seroconverted to the other type. Maternal infection Risk of neonatal infection Primary infection (no seroconversion) 30-50% Primary infection (seroconversion before 34 weeks) <3% Recurrent infection with visible vesicles < 1% Recurrent infection without visible vesicles 0.02 - 3% These data are also available on-line. http://www.asid.net.au/downloads/Management-of-PerinatalInfections-ASID-2002-rev-2007.pdf Nosocomial infection and infection by a primary caregiver are well recognised 6,7,8 . Neonates are therefore at risk of herpes infection if they come into contact with herpes labialis, or an herpetic whitlow. Consequences: There are four presentations [time of presentation]. localised to skin or mucous membranes generalised multiorgan involvement [week 1; range 0-2 weeks] localised to lung (pneumonitis) [3-7 days] meningoencephalitis [7-30 days] 80 % of untreated localised disease will progress to disseminated +/- CNS disease if untreated. Despite treatment the mortality rate in disseminated disease is 15-20%. 50% of the survivors of CNS disease and 86 % of the survivors of disseminated disease have sequelae 2 . Diagnosis: Virus culture takes 1-4 days 2 . Since delay in diagnosis contributes to worse outcomes 9 , rapid screening with PCR for herpes DNA should be requested in surface vesicle swabs (if present) , nasopharyngeal swabs, blood and CSF. Delay in diagnosis is also contributed to by the absence of vesicles in 30% of file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM] cases, and up to 70% of CNS / disseminated disease 9 . In neonates with a non specific septic illness, and with negative bacterial cultures, features such as elevated transaminases, thrombocytopenia, DIC, respiratory distress and CSF pleocytosis are associated with herpes infection 1, 10 . CNS disease can, however, be present in the absence of pleocytosis and a negative PCR 1 . Maternal presentation RANZCOG does not have a guideline on intervention for maternal herpes but supports the recommendations 1,5 of the Australasian Society for Infectious Diseases (ASID) http://www.asid.net.au/downloads/Management-of-Perinatal-Infections-ASID-2002-rev-2007.pdf The UK Royal College of Obstetricians and Gynaecologists (RCOG) has a published Green-top guideline 11 (no 30) http://www.rcog.org.uk/resources/Public/pdf/greentop30_genital_herpes0907.pdf . Also from the UK, the British Association for Sexual Health and HIV (BASHH) have published guidelines. 12 These can be accessed through the National Guideline Clearinghouse (NCG) http://www.guidelines.gov/summary/summary.aspx?doc_id=12214 Caesarean section is effective in preventing neonatal herpes infection 13 . Prophylactic aciclovir beginning at 36 weeks for recurrent infection is also effective at reducing clinical recurrence at delivery, HSV detection, asymptomatic shedding and C/S for clinical recurrence 14 . The following table summarises the main recommendations of these resources. All three sources stipulate that the neonatologist be informed of the birth. Note that the following is given for information only. This may not reflect the obstetric practice within RPAH presentation ASID RCOG Caesarean section (Level of Evidence III, Grade of Recommendation B) Primary infection at or near term (membrane rupture < 6 hours) Secondary infection with no lesions at delivery Secondary infection with active lesions at If vaginal delivery avoid invasive Caesarean procedures and membrane rupture. Consider IV aciclovir to section mother and infant. (Level of Consider Evidence III, Grade of suppresive Recommendation C) aciclovir Insufficient evidence to recommend continuous aciclovir in the last 4 weeks (Level of Evidence III, Grade of Recommendation B) Vaginal delivery BASHH Caesarean section (Grade of Recommendation B) If vaginal delivery avoid invasive procedures and membrane rupture. Consider IV aciclovir to mother and infant. (Level of evidence IV Grade of recommendation C) Continuous aciclovir in the last 4 weeks. (Level of Evidence Ib, Grade of Recommendation B) Caesarean section not indicated (Level of Evidence III, Grade of Recommendation B) Vaginal delivery (Level of Evidence III, Grade of Recommendation B) Continuous aciclovir in the last 4 weeks reduces recurrence and C/S. (Level of Evidence IV, Grade of Recommendation A) Continuous aciclovir in the last 4 weeks reduces recurrence and C/S. (Level of Evidence Ia, Grade of Recommendation A) Caesarean Caesarean section not routinely section if recommended. (Level of ROM < 6 Evidence III, Grade of file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM] Caesarean section should be considered. (Level of Evidence III, Grade of Recommendation B) delivery hours Recommendation B) Continuous aciclovir in the last 4 weeks reduces recurrence and C/S. ( Grade of Recommendation A) Baby The ASID resource has an algorithm for treating babies born to mothers with a history of genital herpes in 5. Clinical signs of Herpes Infection Full investigations should be performed including lumbar puncture, and iv aciclovir started at 60 mg/kg/day in 3 divided doses 15 . High risk The baby should have surface swabs and investigations, and commenced on aciclovir. If the baby then develops symptoms then lumbar puncture and CNS imaging should be added. Low risk Collect surface swabs at 24 hours and review clinically. If the baby develops clinical signs or the swabs are positive then iv aciclovir is started. Investigations HSV PCR on swabs, blood, CSF (if performed), FBC, LFT's, viral culture on CSF (if performed). Neither the RCOG or BASHH guidelines specify recommendations for the newborn apart from "informing the neonatologist" 11,12 Duration of therapy 15 14 days for localised disease ie skin, oral or ocular. 21 days for disseminated or CNS disease. Nosocomial infection The BASHH guidelines state that mothers, staff and friends/relatives with active HSV infection such as orolabial or an hereptic whitlow should avoid contact between the lesions and neonate (Level of evidence IV grade of Recommendation C) 12 . The RCOG guideline states that "mothers, family members and healthcare workers should take measures to avoid transmission of the virus to the neonate (Level of evidence IV grade of Recommendation C). 11 . Breast feeding should continue unless there is active herpes infection around the nipple area. If a mother develops herpes infection in the perinatal period she should have her immune status to HSV 1 and 2 determined. Staff with active herpes infection should not come to work until the lesion has dried. Staff who have no clinical contact with babies may, however, fulfil administrative duties, teaching, research etc. file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM] Meta-analysis of RCTs of topical aciclovir has found that this reduces healing time but the effect is small, about one day 16 . References 1. Freedman E, Mindel A, Jones CA. Epidemiological, clinical and laboratory aids for the diagnosis of neonatal herpes -- an Australian perspective. Herpes. 2004 Aug;11(2):38-44. 2. Isaacs D and Moxon ER. Handbook of Neonatal Infections; a practical guide. (1999) WB Saunders, London 3. Kropp RY, Wong T, Cormier L, Ringrose A, Burton S, Embree JE, Steben M. Neonatal herpes simplex virus infections in Canada: results of a 3-year national prospective study. Pediatrics. 2006 Jun;117(6):195562. 4. Jones CA, McIntyre P, Isaacs D, Members of the Neonatal HSV study team. Epidemiology of neonatal herpes simplex virus infection in Australia: preliminary report on the Australian Paediatric Surveillance Unit study (1997-1999). Journal of Paediatrics and Child Health 36(3), A15. 2000 5. Jones CA. Herpes simplex virus infections in pregnancy. In: Management of Perinatal Infections (Palasanthiran P, Starr M, Jones CA,eds). Australasian Society for Infectious Disease 2002:pp16–18. 6. Sakaoka H, Saheki Y, Uzuki K, Nakakita T, Saito H, Sekine K, Fujinaga K. Two outbreaks of herpes simplex virus type 1 nosocomial infection among newborns. J Clin Microbiol. 1986 Jul;24(1):36-40. 7. Douglas J, Schmidt O, Corey L. Acquisition of neonatal HSV-1 infection from a paternal source contact. J Pediatr 1983;103: 908–10. 8. Hammerberg O, Watts J, Chernesky M, Luchsinger I, Rawls W. An outbreak of herpes simplex virus type 1 in an intensive care nursery. Pediatr Infect Dis 1983;2:290–4. 9. Kimberlin et al Natural History of Neonatal Herpes Simplex Virus Infections in the Acyclovir Era. Pediatrics 2001;108;223-229 10. Caviness AC, Demmler GJ, Selwyn BJ. Clinical and laboratory features of neonatal herpes simplex virus infection: a case-control study. Pediatr Infect Dis J. 2008 May;27(5):425-30 11. http://www.rcog.org.uk/resources/Public/pdf/greentop30_genital_herpes0907.pdf 12. Clinical Effectiveness Group. 2007 national guideline for the management of genital herpes. London (UK): British Association for Sexual Health and HIV (BASHH); 2007. 13. Brown ZA, Wald A, Morrow RA, Selke S, Zeh J, Corey L. Effect of serologic status and cesarean delivery on transmission rates of herpes simplex virus from mother to infant JAMA. 2003;289:203-9 14. Hollier LM, Wendel GD. Third trimester antiviral prophylaxis for preventing maternal genital herpes simplex virus (HSV) recurrences and neonatal infection. Cochrane Database of Systematic Reviews 2008, Issue 1. Art. No.: CD004946. DOI: 10.1002/14651858.CD004946.pub2. 15. Kimberlin et al. Safety and Efficacy of High-Dose Intravenous Acyclovir in the Management of Neonatal Herpes Simplex Virus Infections Pediatrics 2001 (108 ) 2 , pp. 230-238 16. Worrall G. Clin Evid. 2004 Dec;(12):2312-20. back file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM] file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM] file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM] Revised: December 2008: Dr Girvan Malcolm Reproduced by kind permission of the authors: Jones CA. Herpes simplex virus infections in pregnancy. In:" Management of Perinatal Infections". Palasanthiran P, Starr M , Jones CA, Eds. Australasian Society for Infectious Diseases. Book House, Sydney, 2002. p 16-18. Note that an updated version is in preparation which will include further recommendations file:///Volumes/neonatal/html/Newprot/herpes.html[15/10/13 11:54:58 AM]