Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
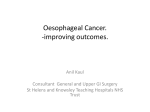
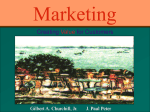
Articles Stents as sole therapy for oesophageal cancer: a prospective analysis of outcomes after placement Russell E White, Robert K Parker, John W Fitzwater, Zachariah Kasepoi, Mark Topazian Summary Lancet Oncol 2009; 10: 240–46 Published Online February 17, 2009 DOI:10.1016/S14702045(09)70004-X See Reflection and Reaction page 203 Tenwek Hospital, Bomet, Kenya (R E White MD, R K Parker BS, J W Fitzwater MD, Z Kasepoi MBchB); Department of Surgery, Brown Medical School, Rhode Island Hospital, Providence, RI, USA (R E White); Indiana University School of Medicine, Indianapolis, IN, USA (R K Parker); Texas Tech University Health Sciences Center, Lubbock, TX, USA (J W Fitzwater); and Miles and Shirley Fiterman Center for Digestive Diseases, Department of Internal Medicine, Mayo Clinic, Rochester, MN, USA (M Topazian MD) Correspondence to: Dr Russell E White, Tenwek Hospital, PO Box 39, Bomet, Kenya [email protected] Background Therapies for inoperable oesophageal cancer include chemoradiotherapy and placement of a self-expanding metal stent (SEMS). Few data are available regarding SEMS as sole therapy for patients with inoperable disease who have not already received, or are unfit for, chemoradiotherapy. The aim of this study was to determine survival, adequacy of palliation, and complications after SEMS placement as sole therapy for inoperable oesophageal cancer in a resource-limited setting. Methods Data were prospectively gathered on all patients with oesophageal cancer treated with SEMS between Jan 1, 1999, and May 20, 2008, at a hospital in Kenya where chemoradiotherapy is unavailable. Dysphagia scores, morbidity, mortality, and survival were assessed. Follow-up was done during clinic visits, home visits, and by mobile phone. Findings 1000 stents were placed in 951 patients. Long-term follow-up was obtained for 334 patients (35%) with a median survival of 250 days (IQR 130–431, 95%CI 217–301). Mean dysphagia scores improved from 3·3 (SD 0·6) pre-SEMS (n=697) to 1·0 (SD 1·3) for patients (n=78) still alive and 1·8 (SD 1·2) at time of death (n=165). Survival of 17 patients with follow-up who had perforation during tumour dilation (treated with SEMS) was 283 days (IQR 227– 538) similar to the 317 patients with follow-up data who did not have a perforation (245 days, 124–430). 20 patients with a tracheo-oesophageal fistula lived a median of 142 days (IQR 73–329). Early complications occurred in 6% (54 of 951 patients) and late complications occurred in 19% (62 of 334 patients). SEMS-related mortality was 0·3% (three of 951). Interpretation SEMS effectively palliate inoperable oesophageal cancer. Survival may be longer than previously reported when SEMS are placed in all patients with inoperable oesophageal cancer, as in our study, rather than those failing or unfit for chemoradiotherapy. SEMS seem to be an appropriate technology for palliation of oesophageal cancer in resource-limited settings. Given the proportion of patients lost to follow up, these findings merit further confirmation. Funding Boston Scientific Corporation (Natick, MA, USA) and Advanced Technology and Materials Company (Beijing, China). Introduction Oesophageal carcinoma, the sixth most common cause of cancer mortality, has a worldwide 5-year prognosis of less than 10%.1,2 Dysphagia is the most common presenting symptom. Due to the elastic properties of the oesophageal wall, and the lack of a serosal layer in the oesophagus, dysphagia develops late in the course of the disease, and locally advanced cancer is usually present by the time symptoms develop. Squamous-cell oesophageal carcinoma has a marked geographical variation in incidence, and is the most common cancer in Kenya.3 At our referral hospital in western Kenya, oesophageal carcinoma accounts for 35% of all tumours, and 90% of patients present with inoperable disease.4 Combination chemotherapy and radiotherapy has efficacy in the treatment of locally advanced oesophageal cancer,5 but our patients do not have routine access to these treatment modalities. Palliation is therefore the treatment goal in these patients and ideally should be minimally invasive and affordable by use of the locally available technology, with as little need as possible for re-intervention.6 240 Self-expanding metal stents (SEMS) are an established palliative therapy for cancer of the oesophagus. SEMS provide fast, complete, and life-long management of dysphagia in most patients.7,8 Outpatient placement of SEMS is the palliative treatment of choice at our institution, located in a resource-limited area of rural western Kenya.9 This study was designed to assess the outcomes of inoperable patients with symptomatic oesophageal cancer who were treated solely with SEMS placement. Methods Patients All patients were cared for at a single institution, Tenwek Hospital in Bomet, Kenya, between Jan 1, 1999, and May 20, 2008. Patient data were obtained from a prospectively collected, standardised database. Patients with dysphagia due to inoperable oesophageal cancer (panel) were offered treatment with SEMS. Informed consent was obtained from all patients and their available family members before undergoing endoscopy, dilation, or stent placement. This study was approved by the ethical review committee at Tenwek Hospital. A few patients included in the database www.thelancet.com/oncology Vol 10 March 2009 Articles who were enrolled on this study were also described in initial reports of SEMS placement without fluoroscopy9 and SEMS placement for iatrogenic perforation.10 Additionally, a few patients are participants in an ongoing prospective trial comparing SEMS diameters. Procedure Before stent placement, patients clinically suspected to have oesophageal cancer because of progressive dysphagia were referred for endoscopy. Most patients declined sedation for endoscopy, because it doubles the cost of the procedure (from around US$13 to $26). All patients received pharyngeal topical anaesthesia. Before endoscopy, the possibility of SEMS placement was discussed with patients, especially those who did not appear to be candidates for surgery (panel); about half were potential candidates for surgery or decided not to undergo SEMS placement, usually because of cost (the average cost of an Advanced Technology and Materials [Beijing, China] SEMS was about $200 during the study period). Endoscopic visualisation of the tumour was done and biopsies were typically taken for confirmation. If the tumour prevented passage of a 9·8-mm diameter endoscope, it was progressively dilated with tapered dilators (Savary-Gillard; Wilson Cook Medical, Winston-Salem, NC, USA) after the passage of a guidewire as previously described.9 Patients choosing not to receive SEMS also underwent dilation to provide some relief of dysphagia. Tumour dilation was necessary in about 90% of patients in this series. After dilation, the endoscope was passed through the tumour to the stomach, proximal and distal tumour margins were visualised, and the distance of these tumour margins from the incisors was noted. A SEMS was then deployed under direct endoscopic visualisation without the use of fluoroscopy, as previously described.9 All patients with a stent crossing the gastro-oesophageal junction were informed of the likelihood of reflux and prescribed acidblocking medication. Patients with a tracheo-oesophageal fistula were given indefinite, suppressive antibiotics in an attempt to reduce morbidity from pneumonia. Diagnosis and treatment were often done during the same initial visit and during one endoscopic procedure. Statistical analysis Dysphagia scores were noted prospectively, both before and after stent placement, by use of Ogilvie’s scale: 0=able to swallow a normal diet; 1=able to swallow some solids; 2=able to swallow semi-solids only; 3=able to swallow only liquids; 4=unable to swallow saliva.11 Systematic, prospective efforts were made to obtain follow-up data by several methods: patients were interviewed at the time of return visits to the hospital outpatient clinics; home visits were made by endoscopy personnel for patients who lived within Tenwek Hospital’s community health catchment area (the two surrounding districts representing a radius of about 75 km); and patients with mobile phones www.thelancet.com/oncology Vol 10 March 2009 were contacted by phone to obtain follow-up data. Follow-up data were sought at 3-month intervals after SEMS placement. For patients who died, date of death and symptoms present at death were obtained from family members. Outcome was assessed with regard to early complications (including chest pain, perforation, bleeding, infection, and death), late complications (including stent migration, overgrowth, obstruction, tracheo-oesophageal fistula, and gastrointestinal Panel: Indications and contraindications for SEMS placement at Tenwek Hospital Indications for SEMS as opposed to surgical resection • Distant metastases • Tracheo-oesophageal fistula • Phrenic or recurrent laryngeal nerve palsy Relative indications for SEMS as opposed to surgical resection • Age >80 years • Extreme cachexia or malnutrition • Poor exercise tolerance • Marked medical comorbidities • HIV positivity Absolute contraindications for SEMS • Tumour involving the upper oesophageal sphincter Relative contraindications for SEMS • Extensive tumour involvement of the gastric cardia Patients Patient demographics Patients, n Age (years), mean (SD) 951 62 (14) Age ≥50 years, n 547/702 Male sex , n 443/715 Kalenjin ethnicity , n 305/683 Preprocedure dysphagia score, mean (SD) 3·3 (0·6) Procedure and tumour specifics Tumour length (cm), mean (SD) Maximum dilation size (mm), median (IQR) 5·8 (2·7) 14 (13–15) Tumour histology Squamous-cell carcinoma, n Adenocarcinoma, n Other, n Unknown or not recorded, n 339/360 18/360 3/360 591/951 Type of stent AT&M SEMS (Advanced Technology and Materials, Beijing, China), n 612/1000 Ultraflex (Boston Scientific Corporation, MA, USA), n 289/1000 Wallstent (Boston Scientific Corporation, MA, USA), n 14/1000 Other or unknown or not recorded, n 85/1000 Table 1: Characteristics of patients who underwent SEMS placement 241 Articles Role of the funding source 1·0 The sponsors of this study had no role in the design of the study, data collection or analysis, data interpretation, or manuscript preparation. The sponsors did not have access to study data. The corresponding author had full access to all the data and the final responsibility to submit for publication. Proportion surviving 0·75 0·5 Results 0·25 Median survival 250 days 0 0 200 400 600 800 1000 1200 1400 Follow-up time (days) Number at risk 334 137 37 10 5 3 2 Figure 1: Kaplan-Meier analysis of survival for all patients with follow-up (n=334) Number of complications Early complications Perforation Bleeding Severe chest pain Death 34* 7 10 3 Late complications† Overgrowth or obstruction 55 Migration 3 Tracheo-oesophageal fistula after SEMS placement 8 SEMS=self-expanding metal stent. 10 patients had both an early and late complication. *37 perforations occurred in the 1950 patients undergoing endoscopic dilation of an oesophageal tumour during the study period, 34 of whom were treated with SEMS placement. Overall perforation frequency was 1·9%. †Occurring in 62 of 334 patients with long-term follow-up; four patients had obstruction or overgrowth twice. Table 2: Procedure-related complications haemorrhage), dysphagia scores, and survival. Performance scores were not prospectively collected for most patients in this study, with data available for only 26 patients. Results were noted as mean (SD) and as medians with IQR when appropriate. Survival was expressed as median survival in days to death and also assessed by the Kaplan-Meier method by using patients still alive at the time of last follow-up as the censored variable. p<0·05 was considered statistically significant. Variables that were significant for survival at p<0·1 (ie, tracheooesophageal fistula at presentation, perforation, male sex, and age under 50 years) were included in a Cox proportional hazard analysis of risk factors. Data analysis was done with Microsoft Excel, Epi Info version 3.4.3, and STATA/IC 10.1. 242 1000 stents were placed in 951 patients. Patient characteristics are shown in table 1. The median age at presentation was 62 years (range 20–99; IQR 53–71). The male to female ratio was 1·6:1. Mean pre-endoscopy dysphagia score was 3·3 (SD 0·6), with 96% of patients (667 of 697), for whom data was available, scoring three or above. Pathology reports of oesophageal biopsy were available on the hospital endoscopy database for nearly half of the patients; others had previously undergone biopsies at other institutions, did not undergo biopsy, or their biopsy result was not recorded in the endoscopy database. The proportion of patients with squamous-cell oesophageal carcinoma was 94% (339 of 360). The most common contraindication to surgery was extreme cachexia and malnutrition. Three patients were deemed inoperable because of HIV infection; until 2005, CD4 counts and highly active antiretroviral therapy were not available to our patients. Most stents were placed in patients on an outpatient basis in our endoscopy clinic, and various types of stent were used (table 1). Complete data on stent diameters and lengths was not available, and these variables could not be assessed in univariate analysis. Covered stents were placed in 819 of 915 patients (90%). Follow-up data were available for 334 of 951 (35%) patients with a mean follow-up time of 207 days (SD 187; [range 2–1277]). 74 patients with mobile phones were successfully contacted, 17 of whom were still alive at the time of most recent follow-up. Follow-up data were obtained during clinic visits for 106 patients. The rest of the follow-up data for the 154 remaining patients were obtained during home visits. 195 patients were followed until the end of life, and 139 were alive at the time of the most recent follow-up, a mean of 184 days after SEMS placement (SD 187; range 6–1277). Overall, Kaplan-Meier median survival was 250 days (IQR 130–431, 95%CI 217–301) (figure 1). Of the patients who were alive at the time of the most recent follow-up, 70 of 78 (90%) reported continued improvement in dysphagia, with a mean dysphagia score of 1·0 (SD 1·3). For patients who died, mean dysphagia score at death (as reported by family members) was 1·8 (SD 1·2), with 129 of 165 (77%) reporting improvement, 36 of 165 (20%) reporting no change, and five of 165 (3%) reporting worsened dysphagia compared with initial presentation. A tracheo-oesophageal fistula was present on initial diagnosis of cancer in 41 patients. Follow-up data available for 20 patients with a tracheo-oesophageal fistula showed a median survival of 142 days (IQR 73–329; p=0·08 compared www.thelancet.com/oncology Vol 10 March 2009 Articles with the remainder of the study cohort who had a median survival of 257 days [IQR 136–431]). Eleven of these patients were followed until death at a median of 94 days (IQR 50–177) after SEMS placement, and nine were still alive at the time of most recent follow-up. Data regarding dysphagia were available for 15 patients with a tracheooesophageal fistula; 13 showed an improvement in symptoms after SEMS placement. Tracheo-oesophageal fistula was diagnosed after SEMS placement in an additional eight patients; median time to diagnosis was 177 days (IQR 150–254; range 88–396) post-procedure. Four of these patients underwent placement of a second stent. Only two patients who developed a tracheo-oesophageal fistula after SEMS placement were followed until death; one received a second stent, the other elected not to undergo further intervention, and each lived for one month after the diagnosis of the tracheo-oesophageal fistula. Procedural-related complications are shown in table 2. Although pain was adequately treated post-procedure with codeine for most patients, ten of 951 needed additional analgesics. No stents were removed due to intolerable pain. During the study period, 1950 oesophageal tumour-dilation procedures were done at Tenwek Hospital, with perforation occurring in 37. 34 of the 37 patients were treated with immediate SEMS placement. For some of these 34 patients, SEMS placement had not been originally planned. One of the 34 patients with a perforation who received SEMS and the three patients with a perforation who underwent surgery died within 30 days of the procedure. Long-term follow-up data were available for 17 of the remaining 33 patients, with nine patients still alive at the time of the most recent follow-up (mean 187 days [SD 112]) and eight followed until death at a median of 261 days (IQR 198–453) after SEMS placement, resulting in Kaplan-Meier median survival of 283 days (IQR 227–528). Because only half of all patients undergoing tumour dilation had SEMS placement at our institution, but almost all patients with a perforation received a SEMS as therapy for their perforation (even if SEMS placement was not planned beforehand), we have reported the incidence of perforation using all 1950 tumour dilation procedures as the denominator. Three procedural-related deaths occurred within 30 days of stent placement. One patient who had a stent placed after an iatrogenic perforation during dilation of a bulky tumour died within the first week of ongoing sepsis, despite aggressive inpatient antibiotic therapy. A patient with advanced carcinoma and vocal-cord paralysis, who was stented without complication, presented 12 days after the procedure with altered mental status and left empyema. Despite appropriate treatment with a chest tube and intravenous antibiotics, the patient never regained consciousness and died 16 days after stent placement. The third patient died at home during the night of the date of discharge from the hospital. After stent placement, the patient had been observed overnight at the hospital with no significant chest pain, and was swallowing at discharge. The family reported that the patient was doing well on www.thelancet.com/oncology Vol 10 March 2009 arrival at home and died suddenly. Although the cause is unknown, we included this patient as a procedural-related death because of the time course. Symptomatic tumour overgrowth of the stent was diagnosed in 51 of 334 patients during follow-up at a Initial group, n Patients with follow-up data, n Median survival p value p value (days), IQR (Wilcoxon) (Log-rank) Age (years) ≤50 156 67 128 (86–399) >50 547 263 263 (144–455) Men 443 206 216 (121–376) Women 272 127 304 (159–552) Kalenjin 305 187 237 (116–375) Non-Kalenjin 378 137 315 (146–430) 1 or 2 30 15 310 (216–352) 3 or 4 667 309 247 (127–431) <4 429 205 252 (144–430) 4 268 119 233 (114–442) <3 N/A 107 175 (91–314) 3 or 4 N/A 58 181 (115–281) Mobile ‘phone N/A 74 208 (134–498) Home visit and clinic records N/A 260 254 (118–426) Proximal edge ≤ 8 cm of UOS 230 121 265 (136–430) Proximal edge >8 cm from UOS 470 196 248 (123–450) Sex Ethnicity Initial dysphagia score Initial dysphagia score Dysphagia score at death Type of follow-up Proximal measurement of tumour Maximum dilation before SEMS placement <14 mm 188 65 233 (114–406) ≥14 mm 280 138 192 (95–438) Perforation treated with SEMS placement Yes 34 17 283 (227–528) No 685 317 245 (124–430) Yes 41 20 142 (73–329) No 678 314 257 (136–431) 339 154 250 (137–389) 18 10 331 (90–533) TOF diagnosed at initial presentation 0·015 0·062 0·037 0·0010 0·21 0·44 0·20 0·61 0·32 0·42 0·86 0·26 0·61 0·17 0·41 0·43 0·18 0·62 0·094 0·18 0·087 0·27 0·52 0·58 0·10 0·078 0·50 0·54 Histology Squamous-cell carcinoma Adenocarcinoma Tumour length ≤6 cm 314 146 281 (159–533) >6 cm 329 160 226 (125–413) AT&M 612 154 228 (115–430) Ultraflex 289 153 249 (141–410) Type of stent IQR=interquartile range. UOS=upper oesophageal sphincter. SEMS=self-expanding metal stent. TOF=tracheo-oesophageal fistula. AT&M=Advanced Technology and Materials Company. Table includes all patients with follow-up (n=334). Table 3: Univariate analysis of variables potentially affecting median survival 243 Articles Hazard ratio (95% CI) Coefficient (SE) p value Z value Age ≤ 50 years (yes/no) 1·26 (0·87–1·83) 0·23 (0·19) 1·24 0·217 Perforation (yes/no) 0·62 (0·30–1·26) –0·49 (0·37) –1·32 0·186 Women (yes/no) 0·63 (0·46–0·87) –0·48 (0·16) –2·85 0·004 TEF at time of presentation (yes/no) 1·09 (0·57–2·07) 0·08 (0·33) 0·25 0·799 TEF=tracheo-oesophageal fistula. Table 4: Cox proportional hazard analysis for all clinical and endoscopic factors with p<0·1 in univariate analysis Women Men 1·00 Proportion surviving 0·75 0·50 0·25 Median survival Women=303 days Men=216 days 0 0 200 400 600 800 1000 1200 3 0 2 0 1400 Follow-up (days) Number at risk Women Men 127 206 63 74 22 15 7 3 5 0 Figure 2: Kaplan-Meier analysis of survival for all patients with follow-up, by sex median of 144 days after SEMS placement (IQR 79–251). 30 patients elected to have an additional stent placed, and four of these underwent placement of a third stent for a second obstruction or overgrowth. The effects of clinical and endoscopic variables on long-term survival are shown in tables 3 and 4. In the univariate analysis (table 3), age less than or equal to 50 years (p=0·015) and male sex (p=0·037) were both associated with a shorter median survival. In a Cox proportional hazards model, male sex was the only variable predictive of shorter median survival (table 4). Survival curves by sex are shown in figure 2. Discussion This cohort study provides both early and late complications and survival data for a large, consecutive series of patients with symptomatic, inoperable oesophageal cancer who were treated with SEMS placement as sole therapy. This study also includes a large, single-centre experience with SEMS placement for two important complications of oesophageal cancer: tracheo-oesophageal fistula and iatrogenic perforation. The median survival of patients with follow-up data was 250 days. 244 Although staging with CT or endoscopic ultrasonography is not available in our region, most patients had obstructive malignancies that prevented the passage of a 9·8-mm diameter video endoscope. Previous studies have shown that 85% of such patients have locally advanced T3–4 or N1 disease.12 Furthermore, in patients deemed operable at our institution, 71% had T3–4 or N1 disease, or both, at the time of resection. Thus, the likelihood exists that almost all of our inoperable patients treated with SEMS alone had stage 3 or 4 disease. Survival of patients with oesophageal cancer is often poor, even with the best available therapy. In developed countries, 5-year survival is less than 30% for patients with localised disease who undergo definitive radiotherapy and chemotherapy5 and less than 40% for those undergoing surgical resection with or without neoadjuvant therapy.13 Survival is substantially worse for the subset of patients with locally advanced, T3–4 or N1 disease, for whom median survival is 15–19 months, whether treated with surgery, with or without neoadjuvant therapy, or radiotherapy and ongoing chemotherapy.13,14 Patients with metastatic disease and those unable to undergo intensive therapy have an even worse survival. Worldwide 5-year prognosis of oesophageal cancer is less than 10%.1,2 Although SEMS have no direct antitumour activity, they probably extend the survival of symptomatic, inoperable patients by improving nutritional intake and preventing starvation, dehydration, and aspiration. Most studies of SEMS from developed nations assess patient populations who have failed previous treatment or are unfit for chemotherapy and radiotherapy, and hence report shorter median survivals for patients undergoing SEMS placement. Median survival after SEMS placement ranges from 49 to 186 days in European and North American series,15–25 and is often less than half the survival time we noted. A nonrandomised, case–control study compared chemotherapy and radiotherapy with SEMS placement alone in 72 patients with locally advanced disease.26 The investigators reported an improved median survival (11 months vs 4 months) and 5-year survival (15% vs 0%) in the patients receiving radiotherapy and chemotherapy compared with those receiving SEMS alone. Because patients and their physicians chose between treatment modalities in the aforementioned study, the likelihood exists that those who were frailer and less fit received SEMS. Our data avoid this bias and present a closer estimate of the expected survival for inoperable patients with symptomatic oesophageal cancer treated with SEMS alone. Unfortunately, data collected prospectively during the study did not include performance scores for most patients to assess this theory. The median survival in this series of 8·4 months compares favourably to other reported palliative modalities for advanced disease, including photodynamic therapy (4·8 months),27 laser therapy (4·1–4·6 months),28,29 and single-dose brachytherapy (4·9–7·9 months).15,30–32 It is likely that these other palliative modalities would also do better when not used as salvage therapies or for the www.thelancet.com/oncology Vol 10 March 2009 Articles least fit patients. Single-dose brachytherapy seems to be better than SEMS in randomised trials, with a lower frequency of complications and better quality of life.15,33 In one study, median survival was 145 days after SEMS placement, and was similar after brachytherapy.15 The group of Dutch investigators suggested that SEMS are nevertheless a better option for patients with severe dysphagia, short life expectancy, and with a need for quick relief of symptoms.15 Most patients in this series meet these criteria (mean dysphagia score of 3·3 in our setting vs 2·8 in the Dutch study). SEMS provided excellent and life-long palliation of dysphagia for most patients in this series. 16% of patients (54 of 334) developed symptomatic stent obstruction or migration needing repeat endoscopic intervention. In these patients, symptoms typically responded well to placement of a second SEMS. An additional 6% of patients (54 of 951) developed early complications. Procedure-related mortality was 0·3% (three of 951). These complication frequencies are within ranges previously reported by other investigators.34–37 2% of patients (eight of 334) developed a tracheo-oesophageal fistula after SEMS placement, typically at the proximal flange of the SEMS. These tracheo-oesophageal fistulas were probably caused by the indwelling SEMS, in combination with disease progression, and were difficult to treat effectively. This cohort study shows that SEMS placement is an effective treatment strategy for patients with iatrogenic perforation of their oesophageal tumours, and those presenting initially with tracheo-oesophageal fistula. These have traditionally been considered morbid complications of oesophageal cancer, and have been associated with high 30-day mortality. In this series, patients treated for iatrogenic perforation with immediate SEMS placement had a median survival of 283 days (9·4 months), very similar to the survival of the entire cohort. Those presenting with a tracheo-oesophageal fistula had a median survival of 142 days (4·7 months) after SEMS placement. This shorter survival was not significant, but determination of statistical significance was limited by the small number of patients. Although complete data were available regarding early complications, long-term follow-up data were only obtained in 35% of patients (334 of 951) undergoing SEMS placement, which presents a major source of potential bias in our study findings. The absence of long-term follow-up data for 65% of patients could potentially result in either increased or decreased complication frequencies and life expectancy. We made systematic, prospective attempts to obtain follow-up data. All patients with an address were contacted by post, all those with phones were contacted by a phonecall, and home visits were arranged for patients living within the two surrounding districts (about a 75-km radius). Mobile phones became widely available in Kenya near the end of the study period. Tenwek Hospital is a referral centre for oesophageal disease, and many patients travel a long distance to obtain www.thelancet.com/oncology Vol 10 March 2009 treatment at the hospital. Because travel costs are high and most patients have limited resources, many patients do not return to the hospital clinics for routine follow-up visits, and might not be able to return even if symptoms recur or complications develop. Tenwek Hospital is located in a region populated largely by ethnic Kalenjins. The finding that median survival was not statistically different between Kalenjin versus non-Kalenjin patients, or between those with follow-up by mobile phone versus home visits, could suggest that patients living at greater distances from the hospital did not have substantially different survival compared with those living in the hospital region. More comprehensive follow-up data are needed, and future studies could improve the evidence base. Risk-factor analysis showed only age and sex as significant determinants of survival (p<0·05). Age 50 years or less was associated with a decreased median survival. This surprising finding could be due to different tumour biology, aetiology, or stage, or possibly to delays in seeking medical care for younger patients. No difference in survival between young and old patients with oesophageal cancer was seen in Turkey,38 Philadelphia (PA, USA),39 or Los Angeles (CA, USA),40 although younger patients typically had more advanced disease at the time of presentation. Conversely, Chinese investigators showed that younger patients with squamous-cell cancer had more aggressive tumour histology and a poorer prognosis than older patients.41 This finding deserves further study. When assessing potential risk factors in multivariate analysis, only male sex was a significant risk factor. SEMS are an appropriate palliative technology for resource-limited settings. In a single outpatient intervention, most patients with inoperable oesophageal cancer receive durable palliation of their major symptom. In our experience, survival after SEMS placement in such patients is substantially longer than reported in studies from resource-rich nations. SEMS placement requires flexible gastroscopy equipment and an experienced operator, but does not require fluoroscopy or the more extensive medical infrastructure needed to deliver intensive chemotherapy and radiotherapy. Two additional hospitals within Kenya have recently implemented SEMS treatment for inoperable oesophageal cancer. We believe this technique, with appropriate training, can be adapted for use in many resource-limited settings. Contributions REW and MT were responsible for the conception and design of the study. REW, ZK, and MT were responsible for the stent placement procedures. REW and ZK supervised data collection and assembly. REW, RKP, and JWF were responsible for data analysis. All authors contributed to data interpretation and writing of the manuscript. Conflicts of interest The authors declared no conflicts of interest. Acknowledgments We gratefully acknowledge Boston Scientific Corporation, Natick, MA, USA, which donated the Ultraflex oesophageal stents used in this study. We also thank Advanced Technology and Materials Company, Beijing, China, for supplying SEMS at reduced cost. 245 Articles References 1 Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: 74–108. 2 Pisani P, Parkin DM, Bray F, Ferlay J. Estimates of worldwide mortality from 25 cancers in 1990. Int J Cancer 1999; 83: 18–29. 3 White RE, Abnet CC, Mungatana CK, Dawsey SM. Oesophageal cancer: a common malignancy in young people of Bomet District, Kenya. Lancet 2002; 360: 462–63. 4 White RE, Kasepoi Z, Harewood GC, Ng T, Cioffi W, Topazian M. Experience with 1,345 esophageal cancer patients seen at a single mission hospital in western Kenya. Gastrointest Endosc 2006; 63: AB124. 5 Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). JAMA 1999; 281: 1623–27. 6 Kmietowicz Z. Tackle cancer in Africa now to prevent catastrophe, say health activists. BMJ 2007; 334: 1022–23. 7 Baron T. Expandable metal stents for the treatment of cancerous obstruction of the gastrointestinal tract. N Engl J Med 2001; 344: 1681–87. 8 Conio M, Repici A, Battaglia G, et al. A randomized prospective comparison of self-expandable plastic stents and partially covered self-expandable metal stents in the palliation of malignant esophageal dysphagia. Am J Gastroenterol 2007; 102: 2667–77. 9 White RE, Mungatana C, Topazian M. Esophageal stent placement without fluoroscopy. Gastrointest Endosc 2001; 53: 348–51. 10 White RE, Mungatana C, Topazian M. Expandable stents for iatrogenic perforation of esophageal malignancies. J Gastrointest Surg 2003; 7: 715–20. 11 Ogilvie AL, Dronfield MW, Ferguson R, Atkinson M. Palliative intubation of oesophagogastric neoplasms at fiberoptic endoscopy. Gut 1982; 12: 1060–67. 12 Pfau PR, Ginsberg GG, Lew R, Faigel DO, Smith DB, Kochman ML. Esophageal dilation for endosonographic evaluation of malignant esophageal strictures is safe and effective. Am J Gastroenterol 2000; 95: 2813–15. 13 Schwer AL, Ballonoff A, McCammon R, Rusthoven K, D’Agostino RB, Schefter TE. Survival effect of neoadjuvant radiotherapy before esophagectomy for patients with esophageal cancer: a surveillance, epidemiology, and end-results study. Int J Radiat Oncol Biol Phys 2008; 72: 449–55A. 14 Bedenne L, Michel P, Bouche O, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol 2007; 25: 1160–68. 15 Homs MY, Steyerberg EW, Eijkenboom WM, et al. Single-dose brachytherapy versus metal stent placement for the palliation of dysphagia from oesophageal cancer: multicentre randomised trial. Lancet 2004; 364: 1497–504. 16 Vakil N, Morris AI, Marcon N, et al. A prospective, randomized, controlled trial of covered expandable metal stents in the palliation of malignant esophageal obstruction at the gastroesophageal junction. Am J Gastroenterol 2001; 96: 1791–96. 17 Hills KS, Chopra KB, Pal A, Westaby D. Self-expanding metal oesophageal endoprostheses, covered and uncovered: a review of 30 cases. Eur J Gastroenterol Hepatol 1998; 10: 371–74 18 Xinopoulos D, Dimitroulopoulos D, Tsamakidis K, et al. Palliative treatment of advanced esophageal cancer with metal-covered expandable stents. A cost-effectiveness and quality of life study. J BUON 2005; 10: 523–28. 19 Johnson E, Enden T, Noreng HJ, et al. Survival and complications after insertion of self-expandable metal stents for malignant oesophageal stenosis. Scand J Gastroenterol 2006; 41: 252–56. 20 Riccioni ME, Shah SK, Tringali A, et al. Endoscopic palliation of unresectable malignant oesophageal strictures with self-expanding metal stents: comparing Ultraflex and Esophacoil stents. Dig Liver Dis 2002; 34: 356–63. 21 Christie NA, Buenaventura PO, Fernando HC, et al. Results of expandable metal stents for malignant esophageal obstruction in 100 patients: short-term and long-term follow-up. Ann Thorac Surg 2001; 71: 1797–801. 22 Gevers AM, Macken E, Hiele M, Rutgeerts P. A comparison of laser therapy, plastic stents, and expandable metal stents for palliation of malignant dysphagia in patients without a fistula. Gastrointest Endosc 1998; 48: 383–88. 246 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 Cwikiel W, Tranberg KG, Cwikiel M, Lillo-Gil R. Malignant dysphagia: palliation with esophageal stents—long-term results in 100 patients. Radiology 1998; 207: 513–18. De Palma GD, Galloro G, Sivero L, et al. Self-expanding metal stents for palliation of inoperable carcinoma of the esophagus and gastroesophageal junction. Am J Gastroenterol 1995; 90: 2140–42. Winkelbauer FW, Schöfl R, Niederle B, Wildling R, Thurnher S, Lammer J. Palliative treatment of obstructing esophageal cancer with nitinol stents: value, safety, and long-term results. AJR Am J Roentgenol 1996; 166: 79–84. Wong SKH, Chiu PWY, Leung SF, et al. Concurrent chemoradiotherapy or endoscopic stenting for advanced squamous cell carcinoma of esophagus: a case control study. Ann Surg Oncol 2008; 15: 576–82. Litle VR, Luketich JD, Christie NA, et al. Photodynamic therapy as palliation for esophageal cancer: experience in 215 patients. Ann Thorac Surg 2003; 76: 1687–93. Dallal HJ, Smith GD, Grieve DC, Ghosh S, Penman ID, Palmer KR. A randomized trial of thermal ablative therapy versus expandable metal stents in the palliative treatment of patients with esophageal carcinoma. Gastrointest Endosc 2001; 54: 549–57. Spencer GM, Thorpe SM, Blackman GM, et al. Laser augmented by brachytherapy versus laser alone in the palliation of adenocarcinoma of the esophagus and cardia: a randomized study. Gut 2002; 50: 224–27. Harver JC, Fleischman EH, Bellotti JE, Kagan AR. Intracavitary radiation in treatment of advanced esophageal carcinoma: a comparison of high dose rate vs low dose rate brachytherapy. J Surg Oncol 1993; 52: 101–04. Sur RK, Donde B, Levin VC, Mannell A. Fractionated high dose rate intraluminal brachytherapy in palliation of advanced esophageal cancer. Int J Radiat Oncol Biol Phys 1998; 40: 447–53. Sur RK, Levin VC, Donde B, Miszczyk L, Nag S. Prospective randomized trial of HDR brachytherapy as a sole modality in palliation of advanced esophageal carcinoma—an International Atomic Energy Agency study. Int J Radiat Oncol Biol Phys 2002; 53: 127–33. Bergquist H, Wenger U, Johnsson E, et al. Stent insertion or endoluminal brachytherapy as palliation of patients with advanced cancer of the esophagus and gastroesophageal junction. Results of a randomized, controlled trial. Dis Esophagus 2005; 18: 131–39. Cwikiel W, Stridbeck H, Tranberg K, et al. Malignant esophageal strictures: treating with a self-expanding nitinol stent. Radiology 1993; 187: 661–65. Adam A, Ellul J, Watkinson A. Palliation of inoperable esophageal carcinoma: a prospective randomized trial of laser therapy and stent placement. Radiology 1997; 202: 344–48. Siersema PD, Hop WC, van Blankenstein M, et al. A comparison of 3 types of covered metal stents for the palliation of patients with dysphagia caused by esophagogastric carcinoma: a prospective, randomized study. Gastrointest Endosc 2001; 54: 145–53. Mayoral W, Fleischer D, Salcedo J, Roy P, Al-Kawas F, Benjamin S. Non-malignant obstruction is a common problem with metal stents in the treatment of esophageal cancer. Gastrointest Endosc 2000; 51: 556–59. Turkyilmaz A, Eroglu A, Subasi M, Karaoglanoglu N. Clinicopathological features and prognosis of esophageal cancer in young patients. Is there a difference in outcome? Dis Esophagus 2008; published online November 12. DOI:10.1111/j.1442-2050.2008.00890.x. Hashemi N, Loren D, Dimarino AJ, Cohen S. Presentation and prognosis of esophageal adenocarcinoma in patients below age 50. Dig Dis Sci 2008; published online November 23. DOI:10.1007/s10620-008-0565-7. Portale G, Peters JH, Hseih CC, et al. Esophageal adenocarcinoma in patients < or = 50 years old: delayed diagnosis and advanced disease at presentation. Am Surg 2004; 70: 954–58. Lu JP, Xian MS, Hayashi K. Morphologic features in esophageal squamous cell carcinoma of young adults in north China. Cancer 1994; 74: 573–77. www.thelancet.com/oncology Vol 10 March 2009