Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
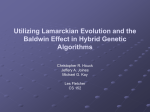
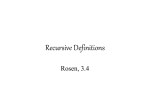
Genioplasty Introduction Chin plays an important role in facial appearance Indications The absolute size is not as important as the relative size and proportion of each structure on the face Facial harmony is the primary determinant of ideal facial appearance The face is balanced when the upper, middle and lower thirds are of equal size and the structures within each segment are proportional in size and prominence ANATOMY The chin is in the area below the labiomental fold esp when viewed lateral. The bony portion of the chin is the mandibular symphysis Embryology The two hemimandibular segments form independently from the first arch with the ossification centres appearing about the 6th week of gestation Intramembranous ossification continues to envelop and invade the much of Meckel’s cartilage and the two mandibular bodies meet at the mandibular symphysis between 4th -12th month after birth as ossification converts syndesmosis into a synostosis Anatomy Between the ages of 10 and 13 all the permanents erupt in the region of the mandibular symphysis and thus genioplasty should not be undertaken until after 15. Sensation of the lower lip and chin and lower incisors is via the mental nerve The mental foramen lies on the same vertical line defined by the pupil, infraorbital foramen and the second bicuspid tooth. After eruption of the permanent dentition the roots of the teeth can be expected to lie above the mental foramen and thus the bone below this level may be used for genioplasty Horizontal osteotomy should be placed 4- 6mm below the mental foramen and this will prevent injury to the mental nerve/ inf alv nerve The genioglossus, geniohyoid and anterior belly of digastric attach to the post portion of the inferior border of the symphysis and the genial tubercle is the point of tendinous attachment As the periosteum is usually stripped off anteriorly during genioplasty preservation of these muscle attachments provides a blood supply to the lower fragment after the horizontal osteotomy Mentalis: arises from the incisive fossa on the anterior aspect of the mandible. It inserts into the skin of the chin. It is innervated by the mandibular branch of the facial nerve (CN VII) (superficial surface) Two actions: 1 protrusion of the lower lip 2 elevation and wrinkling of the skin of the chin Cleft Chin Historically, chin implants attempted to form a cleft chin by placing a groove in the central portion of the implant. This was not successful. Furthermore, chin implants placed under existing chin clefts tend to efface the natural cleft by adding bulk to the soft tissue underlying the cleft. This occurs because of the anatomy underlying a cleft chin. A cleft chin is thin centrally at the cleft, with thicker soft tissue on each side of the cleft. In the cleft chin, the cleft is always the thinnest part of the chin pad, and it is a measure of central muscle deficiency. Normally, the paired mentalis muscles arise at the sulcus to pass transversely (at the fold) and inferoobliquely to insert into the skin of the chin pad. The septum between these muscles usually fades out, and the muscles converge or fuse in the midline to form the single chin pad. Thus, in most people, no central muscle deficiency, or cleft, exists. The mentalis muscles are analogous to two "megaphones" of muscle that usually fuse centrally as they proceed toward the chin pad. The megaphones fuse as they enlarge distally. When the muscles do not fuse centrally, a deficiency occurs or cleft develops (i.e., a muscle-free zone), not unlike that seen between the frontalis muscles. Thus, the cleft chin is the result of a lack of fusion of the insertions of the mentalis muscles or the result of a persistent septum preventing muscle fusion. The anatomy can produce varied forme frustes of chin clefting, ranging from a dimple to a vertical line. Furthermore, the cleft may be partial, involving only the superior or inferior aspects of the mentalis . Terms used to describe abnormal anatomy of the chin 1) microgenia – small chin with an overall deficiency of bone on all three planes 2) retrogenia – the chin is positioned more posteriorly a. pure retrogenia exists when the occlusion is normal b. If there mandibular retrognanthia the retrogenia is secondary 3) macrogenia- large chin If only a hypoplasia of the mandible exists, the term micrognathia is more accurate and should be used. When no skeletal malformation is present, the terms for a recessed chin include retrogenia, microgenia, retruded chin, hypoplastic mentum, and horizontal mandibular hypoplasia. Macro and microgenia can be associated with mandibular prognathism Vertical abnormalities such as increased or decreased ht may also exist Abnormalities with chin sym localized exostoses and a variety of more unusual transverse chin abnormalities may also be present Anatomical Considerations Consider 1. soft tissue (lower lip, mentalis, labiomental fold) 2. bony structures (occlusion, mandible) The lower lip is influenced by 1) The position of the maxillary and mandibular incisors a. The relative amount of over bite and over jet 2) tone of the orbicularis and the mentalis a. The hyperactivity of the mentalis can lead to increase in the vertical height. Underactivity, gravitational ptosis, iatrogenic injury will lead to lower incisor exposure 3) The bony chin projection Soft tissue chin contour is affected by the 1) bony chin projection and length 2) mentalis muscle thickness 3) and the soft tissue chin depth The morphological landmarks are major determinant of the vector and the movement of chin the majority of pts who seek genioplasty for small chins actually had small mandibles and 51% had Class II skeletal deformity and further 40 % had had orthodontic treatment for excess over jet i.e. only 9% had class I occlusion The class of bite will also affect the labiomental fold and i.e. class II leads to lower lip being pushed out and down accentuating the fold. As the height of the lower face elongates the fold attenuates. The labiomental fold deepens as the chin is advanced surgically. The soft tissue of the chin advances on a 0.9:1 ratio with the underlying symphysis up to 8 mm. Beyond this length, muscular and soft tissue forces are thought to cause resorption. There is less predictability in vertical movements PREOP ASSESSMENT Eyeball assessment 1. lip eversion, 2. the anterior teeth 3. chin pad thickness 4. labiomental fold depth and height 5. dynamic chin pad motion with smile. Need to assess the frontal, vertical and transverse facial planes AP view The lower face can be divided into equal thirds by lines passing through the subnasale, stomion, the labiomental crease and the menton(the inferior most point on the soft tissue chin) Equal halves may be divided by lines passing thru the subnasale the muco cut jxn of the lower lip and the menton Facial midline assessed and this is compared with the mand and maxillary dental midlines to assess for asym of the chin Determine whether the cause of the decreased facial ht is secondary to vertical maxillary deficiency, chin deficiency or a combination of both The best method of assessing for maxillary deficiency is to assess the amount of upper incisor show when the lips are in repose Ideal incisor show is 2-3 mm and a pt with no incisor show with normal lip length is said to have a maxillary deficiency. In the absence of vertical maxillary deficiency the reduced facial ht can be attributed to vertical deficiency of the chin. A large no of pts with class II occlusion pattern will have a vertical chin deficiency and if are not candidates for orthognathic surgery will benefit from vertical augmentation Occlusion assessed Profile view(lateral view) The vertical reference line is drawn thru the subnasale and the nasofrontal junction The upper and lower lips should lie anterior to this and the lower lip slightly post to the upper soft tissue pogonion (most forward-projecting point on the anterior surface of the chin) of the chin should lie very close to this line From Yaremchuk: The inclination of the facial profile as defined by a line from the glabella to the pogonion. The broken line is drawn perpendicular to the Frankfort horizontal at an inclination of 0 degrees. The solid red line represents the mean inclination of the study group. The shaded area encompasses 1 SD. (Left) The mean inclination in 100 young North American white men was -3 ± 3.4 degrees. (Right) The mean inclination in 100 young North American white women was -4.1 ± 3 degrees (after Farkas, L. G., Hreczko, T. A., and Katic, M. J. Craniofacial norms in North American Caucasians from birth (one year) to adulthood. In L. G. Farkas (Ed.), Anthropometry of the Head and Face, 2nd Ed. New York: Raven Press, 1994. Appendix A.). In both men and women, note that the chin rests slightly posterior to the lower lip and the lower lip lies slightly posterior to the upper lip. Aesthetic systems A variety of aesthetic and cephalometric analysis have been made to assess the relative and size and shape of the chin 1) Gonzalez dropping a line perpendicular to the frankforts horizontal thru the nasion should intersect the pogonion 2) rickets drawn a line from the nasal tip to the pogonion and the upper and lower lips should lie 4 and 2 mm away from this line – this however is significantly affected by the tip 3) fig E Holdaways related the nasion B point to form a angle of 7-9 degrees with the tangent to the upper lip and chin Investigations 1) photographs- frontal lateral oblique and submental to delineate the soft tissue contour and facial relations 2) lateral cephalogram 3) OPG to visualize the teeth apices and position of the mental nerves 4) CT scan 5) Assess the nose If class II and Class I occlusion consider orthodontic and orthagnathic referral Operations History 1942: Hofer first described the sliding horizontal osteotomy of the mandibular symphysis for microgenia 1950: Gillies – jumping genioplasty, external approach 1957: Trauner/Obwegeser coined the term genioplasty 1964: Converse/Wood-Smith horizontal osteotomy McCarthy devised an algorithm based on the size and shape of the chin in those with normal occlusion Size was classified as small, large, and small/large Shape was characterized abnormal in the horizontal, vertical and horizontal vertical dimension Goals creating an aesthetically pleasing facial contour establishing proportionate facial height. Preserve mental nerve, mentalis function. Contraindications: When considering a mandibular reduction or a sliding osteotomy, carefully evaluate the teeth and the height of the mandible prior to surgery. Having long teeth with a short mandibular height is a relative contraindication for an osseous genioplasty or an aggressive bony reduction. Principles Intraoral/extraoral(submental) approach Subperiosteal dissection create pocket(mentoplasty)/osteotomy(genioplasty) Rigid Fixation – plates better than wires Protect mental nerve Resuspend Mentalis Osseous Genioplasty vs Alloplastic Mentoplasty Autografts such as iliac crest and rib cartilage have been used more frequently for chin augmentation in the past. Nasal bone and cartilage have been used as well. Other options include autogenous or homologous (cadaveric) cartilage or bone, although these latter materials have a higher infection rate than is observed with autografts. Historically, various materials have been used to augment the chin, including paraffin, ivory and methylmethacrylate. Common Alloplastic implants include Supramid, gortex, silicone, polytetrafluoroethylene, Mersiline and polyester mesh have gained a great deal of popularity through the years as a result of patient and surgeon satisfaction. The depth of the labiomental fold may dictate which technique is used. Alloplastic implants tend to deepen the sulcus, which may be particularly unattractive in female patients. With osseous genioplasty, the fold generally increases with advancements and/or vertical shortening and becomes more effaced with vertical lengthening. Alloplasts - easy to place - are less time consuming than a sliding genioplasty (can be done with LA) - limited to the mild to moderately retruded chin, shallow labiomental groove - primarily address deficiencies in the sagittal dimension at the pogonion and width deficiencies immediately lateral to the symphysis. No simple implant reliably changes the vertical dimension of the chin, - complications 1) dehiscence, 2) bone resorption, 3) infection, 4) extrusion, 5) overprojection or underprojection, 6) asymmetry, 7) displacement/migration, 8) capsular contraction(smooth implants), 9) lower-lip retraction, 10) chin ptosis. - Resorption occurs to some extent in many, if not all, patients. One study showed up to 5 mm of resorption at 48 months after surgery. Resorption has been attributed to subperiosteal placement of the implant. Tension in the soft tissue pocket due to pressure from the overlying skin or mentalis musculature has been thought to cause this pressure resorption. The overall soft tissue profile, however, is not usually affected by this bone resorption. Osseous Genioplasty - abnormalities in 3 dimensions can be addressed, making it a more versatile procedure (ie including vertical microgenia with and without retrogenia, vertical macrogenia with retrogenia, and prognathia) - Complications o Mental nerve injury, malunion, nonunion, irregularities, step-type deformities, lip drop, and overcorrection or undercorrection have been reported. Of note, undercorrection is better accepted than overcorrection in which the chin placed forward to the lower lip can yield a disharmonious profile. Pattern of bone remodelling Bone remodelling after genial segment advancement always occurs to a degree and thought to be related to the blood supply and the commonest location is of remodelling (ie absorption and deposition) is at the anterosuperior angle of the advanced segment Zide’s Mentoplasty Principles 1. Standard Chin to Nose Analysis A large nose will make the chin look smaller, and vice versa. Any augmentation that disrupts the chin-nose relationship by creating an excessively large chin may be more acceptable to men, but rarely to women. This is especially true when the labiomental fold is high. The key: always undercorrect women and realize that a sagittal augmentation will also make the chin look longer. Removal of a large implant (without replacement) makes the final configuration of the chin pad a matter of chance. Contraction of a prior pocket under the pad will yield unusual chin pad configurations, which are difficult to correct. Replace with smaller implant 2. Lower Lip Analysis On profile examination, the lower lip should lie slightly posterior to the upper lip, and the most anterior lower lip white roll should be in the same anteroposterior plane as the soft tissue chin point. The advanced, new position of the soft-tissue chin point (that will exist after the placement of the implant) relative to the lower lip on profile view must be considered. When the chin pad soft-tissue thickness is normal (8 to 11 mm), the anterior surface of the implant should not project beyond the labial surface of normally positioned lower incisors. Lower lip eversion may be due to a skeletal deep bite, lower tooth procumbency, or excess lip weight and bulk, as occurs with vascular enlargement of the lower lip. In addition, any anterior tooth position in which a large overjet occurs may also be associated with lower lip eversion. Eversion of the lower lip deepens the labiomental fold and may spuriously advance the lower lip white roll. Often, the bony chin is retropositioned but the existing lip position results in a white roll in close to proper position. Sagittal augmentation in these cases will only decrease the labiomental angle or deepen the labiomental fold. The harmonious relationship between the lower lip white roll and soft tissue pogonion is disturbed. The best operation in these cases is a mandibular advancement. 3. Labiomental Fold Analysis The role of the labiomental fold is crucial to determine the appropriate treatment for microgenia/retrogenia. The labiomental fold is analyzed to determine its height, depth, and distinctness. Its position and depth do not really have normative values. A key point is to analyze what percentage of lower facial height is related to the lip-tomenton chin pad height versus lip-to-labiomental fold height. If the labiomental fold is high or close to the lower lip, the pad percentage is high, and vice versa. In women with a high pad percentage (high or indistinct labiomental fold), an alloplastic chin augmentation can be an aesthetic disaster (Fig. 6). If the fold is very indistinct or high, the chin appears to consist primarily of soft-tissue pad after augmentation. This effect of augmentation is overwhelming, as it appears to enlarge the entire lower face, as opposed to just the chin pad. In contrast, only the chin pad, and not the entire lower face, will look larger after chin augmentation in patients with a very distinct lower labiomental fold. Thus, if the fold is located more inferiorly, augmentation will accentuate only the chin pad. In these cases, augmentation rarely looks too large. 4. Dynamic Chin Pad Analysis It is important to ask the patient to smile. This is critical because ptosis of the softtissue chin pad can occur with smiling. 5. Dynamic Analysis of the Lip/Chin Appearance Examine the patient during smiling and central lip elevation. This part of the physical examination focuses on the lip muscles as they affect chin appearance. Dynamic side view analysis of the patient will demonstrate the degree of soft-tissue effacement and even inferior displacement that may occur with smiling. A malpositioned implant will also be visible during effacement of the soft tissue over the chin prominence. In like manner, an extremely thin chin pad will reveal the underlying bony prominence. The mentalis muscle is carefully examined during the dynamic analysis. By having the patient elevate his or her lower lip, mentalis muscle function and chin pad fasciculations can be seen, and they must be documented. In patients with an active mentalis muscle, as evidenced by a highly animated chin in long face syndrome and one with frequent fasciculations, alloplastic chin augmentation must be carefully considered because it can result in an exaggeration of the dimples and corrugations produced in patients with already excessively strong mentalis muscles. In addition, patients with aberrant muscle motion may experience an exacerbation of this problem after removal of the implant. Often an elderly patient will present with dentures. In such cases, the lower alveolar ridge has been resorbed due to trauma. The mentalis origin may have been pushed down and, thus, chin pad ptosis will ensue. Reduction of this ptosis may, in fact, make the chin look shorter. Furthermore, continued wearing of the dentures will cause recurrence of any correction you perform. Implant Removal Chin augmentation in women should be conservative. If it is not, female patients will nearly always complain of a chin implant that is too large and request removal. The surgeon may decide it is a simple matter to remove it. Nothing can be further from the truth. The insertion of the mentalis muscle into the soft tissue is splayed over the top of the implant. If the implant is removed and no longer supports the soft tissue, two things may occur. Either the implant capsule contracts, drawing with it the overlying soft tissues to which it is attached, resulting in a "ball" or fasciculations below), or excess tissue may result in chin pad droop. To avoid and prevent the ball phenomenon, a smaller implant should be placed after removing a chin implant that is too large. The new implant will support the soft tissues and reduce this phenomenon. Alternatively, excess soft tissue, skin fat, and muscle may require excision from below, or a "vest over pants" method should be used to redrape the muscle after implant removal. Repositioning Proper positioning of the implant ensures that it rests on the pogonion. This position produces the most aesthetically pleasing result and reduces erosion into bone. Unfortunately, some patients present postoperatively with a nonpogonion implant position. Experience shows this predominantly occurs after transoral placement. To avoid this technical error, transcutaneous revision is recommended. Preventing secondary implant movement is key when the implant is removed. In such cases, the pocket is usually too big. If the implant needs additional fixation to prevent displacement, this is best performed from a submental approach. When faced with this situation, secure fixation of the implant in the desired position will be required to stabilize the implant. The following four possibilities can be used in this situation: (1) permanently suture the new implant to the periosteum or soft tissue at the lower border of the mandible in two places; (2) use transpad fixation with either sutures or a needle temporarily; (3) skewer and impale the pad with Kirschner wires permanently; or (4) use a tissue-adhering implant with fixation (i.e., Porex, Gore-Tex, or HTM) Lip Numbness after Chin Augmentation Lip numbness after insertion of an implant must be resolving or improving by 2 to 3 weeks postoperatively; if not, the implant should be removed and trimmed superiorly or the wing position must be lowered. Leaving an implant in situ for 8 or more weeks with numbness may result in some permanent loss of sensation by fascicular pressure; this may necessitate nerve repair. It is best to adjust these implants early, i.e., by 4 weeks postoperatively at the latest. Outcomes Complications 1) poor healing of tissue with scarring in the sulcus and retraction of periodontal tissue from their attachment to the teeth 2) functional disturbances of the lip 3) infection 4) hematoma – may get secondarily infected – usually respond tio aspiration and infection 5) dehiscence – thus important to leave an adequate soft tissue cuff attached to the superior margin 6) ptosis of the chin may occur if the if the soft tissues are stripped from the inferior aspect of the chin during the degloving of the mandible or if mentalis not resuspended 7) avascular necrosis – if a cuff of soft tissue not left attached at the posterior aspect 8) injuries to the mentalis muscle – bizarre dimples on the pogonoin that are most pronounced with animation 9) injuries to the inf alveolar nerve(IAN) – rare if osteotomy made 6mm below level of mental foramen 10) paraesthesia of the IAN occur in most pts and resolve over weeks 11) traumatic myositis ossificans (bone formation in mucle that has been injured) 12) over correction and under correction 13) post op drooling 14) implant exposure 15) non-union 16) dental trauma Patient satisfaction 96 % pt satisfaction for genioplasty and 87 % with alloplastic implants