Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
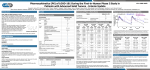
A Phase 1 Dose-Escalation Study of MEK Inhibitor MEK162 (ARRY-438162) in Patients with Advanced Solid Tumors J. Bendell1, K. Papadopoulos2, S. Jones1, E. Barrett3, J. Christy-Bittel3, K. Guthrie3, C. Kass3, K. Litwiler3, C. Napier3, A. Patnaik2 Available at www.arraybiopharma.com 1Sarah Cannon Research Institute (SCRI), Nashville, TN; 2START-South Texas Accelerated Research Therapeutics, San Antonio, TX; 3Array BioPharma Inc., Boulder, CO MEK162 (ARRY-438162): A Potent MEK1/2 Inhibitor The RAS/RAF/MEK/ERK pathway plays a major role in cell growth and survival, and is often aberrantly activated in many cancers. MEK162 is an orally bioavailable, potent, selective, ATP-uncompetitive inhibitor of MEK1/2. MEK162 has nanomolar activity against purified MEK enzyme (IC50 = 12 nM) and inhibits both basal and induced levels of ERK phosphorylation in numerous cancer cell lines (IC50 values ≥ 5 nM). In vivo, MEK162 has demonstrated efficacy in several xenograft tumor models in mice, including those harboring KRAS or BRAF mutations. In vivo, MEK162 enhances the activity of targeted therapies and standard cytotoxic agents in nonclinical tumor models. Methods The objectives of this completed Phase 1 open-label, dose-escalation study were to determine the maximum tolerated dose (MTD) and characterize the safety profile, pharmacokinetics (PK), pharmacodynamics (PD) and preliminary efficacy of MEK162 in patients with advanced solid tumors. Schedule and Doses of MEK162* In 21-day cycles: 30 mg BID 45 mg BID 60 mg BID 80 mg BID *single QD dose on Cycle 1 Day 1 only Safety Safety DLT and MTD AEs, clinical laboratory tests, physical exams, ECGs, ECHO/MUGA scans, ophthalmic exams AEs, clinical laboratory tests, physical exams, ECGs, ECHO/MUGA scans, ophthalmic exams Efficacy Plasma samples (Day 1 and Day 15) Tumor response via RECIST v1.1 (every 6 weeks) Biomarkers Tumor samples (archival), venous blood samples (Screening and predose on Days 1, 8, 15), skin punch biopsy (Screening and Day 15) Subsequent Cycles Cycle 1 Dose-escalation Phase (3 + 3 design) Patient Demographics N = 19 Median age (range), years ECOG (0/1), n Dose limiting toxicities (DLTs) occurred in 2 of 3 evaluable patients in the 80 mg BID dose cohort, thus 60 mg BID was declared the single-agent MTD. All DLTs resolved with interruption of dosing and upon rechallenge at a lower dose, patients tolerated continued treatment with MEK162. Patients (n) Evaluable (n) DLTs (n) 30 mg BID 4 4 0 45 mg BID 4 3 0 60 mg BID 7 7 0 80 mg BID 15/4 57 (33-79) 16/3 Median lines of previous chemotherapy for advanced disease (range), n 2 (0-8) Race (Asian/Black/Caucasian), n 1/1/17 Tumor type, n Colorectal Pancreatic Cholangiocarcinoma Other 7 3 2 7 Mutation status *, n Wild type on all loci tested NRAS KRAS BRAF PI3Kca Dual KRAS/PI3Kca Insufficient or no sample 2 2 5 1 1 1 6 * Archival tumor samples analyzed using Sequenom OncoCarta Panel and/or BEAMing digital PCR. Pharmacokinetics Management of MEK162 Adverse Effects 4 3 DLTs (type and grade) Central serous-like retinopathy (n = 1; G3) Dermatitis acneiform (n = 1; G3 despite maximal treatment measures) 2 Most Common Treatment-related AEs (> 2 Patients) Diarrhea, nausea and vomiting: Treated with standard antiemetic and anti-diarrheal medications; prophylactic treatment was not required. Rash events: Generally G1/2, not requiring dose modification and frequently treated with oral antihistamines and anti-inflammatory agents, topical and oral antibiotics and corticosteriods. G3 rash events required dose modifications. Creatine kinase (CK) elevations: Elevations in CK were asymptomatic, reversible, and did not require dose modifications. Elevations typically showed a rise beginning in Week 1 of dosing with a plateau around 3 weeks and a rapid decline when drug was held or discontinued. Retinal events: Symptomatic, reversible central serous-like retinal eye disorders were managed without specific treatment other than dose modifications. Symptoms included flashing lights/floaters, altered color perception and “darkened vision”. Retinal findings observed on fundoscopy and confirmed by OCT included macular edema/detachment, edema with subretinal fluid and multiple subretinal white lesions. Reasons for Study Termination MEK162 Dose Pharmacokinetics Gender (male/female), n DLTs and MTD 30 mg BID 45 mg BID 60 mg BID 80 mg BID Total n=4 n=4 n=7 n=4 N = 19, (%) Gastrointestinal disorders Diarrhea Nausea Vomiting Stomatitis/Mucositis Abdominal pain Dyspepsia 1 3 1 1 0 1 3 3 3 0 1 1 4 1 1 4 1 0 1 1 2 1 1 1 9 (47) 8 (42) 7 (37) 6 (32) 3 (16) 3 (16) Skin and subcutaneous tissue disorders Rash* Pruritis Dry skin 4 2 0 3 0 1 7 3 3 1 0 0 15 (79) 5 (26) 5 (26) General disorders and Administrative site conditions Peripheral edema Fatigue Retinal Events** 0 2 0 2 1 0 4 1 1 1 1 2 7 (37) 5 (26) 3 (16) Other Increased creatine kinase Anorexia 0 1 1 1 2 0 0 1 3 (16) 3 (16) All Grades * “Rash” combined term includes events of rash, papular rash, macular rash, maculopapular rash, exfoliative rash, skin exfoliation, dermatitis acneiform and acne ** “Retinal Events” include retinopathy and chorioretinopathy Grade 3/4 Treatment-related AEs MEK162 dose 30 mg BID n=4 45 mg BID n=4 60 mg BID n=7 80 mg BID n=4 Total N = 19 Rash* 0 0 1 1 2 Palmar-plantar syndrome 0 0 1 0 1 Chorioretinopathy 0 0 0 1 1 Increased creatine kinase 0 0 2 0 2 * “Rash” combined term included events of rash and dermatitis acneiform MEK162 Dose 30 mg BID 45 mg BID 60 mg BID 80 mg BID Total n=4 n=4 n=7 n=4 N = 19, (%) Disease Progression 4 3 7 3 17 (90) Discretion of Investigator* 0 1 0 0 1 ( 5) Adverse Event 0 0 0 1 1 ( 5) * No benefit from treatment (patient had SD at time study drug was discontinued) Antitumor Activity Preliminary signs of clinical activity were observed in the 17 efficacy-evaluable patients; 15 of 17 had a (RECIST) target lesion at Baseline. Overall best response of PR was achieved in 1 patient (10.2 months duration). Stable disease was observed in 9 patients (7 in the 60 mg BID dose group) with a median duration of 3.9 months (min, 2.1; max, 13.8). The median number of drug administration cycles administered was 2 in both the 30 mg and 45 mg BID dose cohorts, 4 in the 60 mg BID dose cohort and 3 in the 80 mg BID cohort. Plasma PK of MEK162 were assessed on Day 1 and Day 15 of Cycle 1 for each patient. PK parameter estimates for MEK162: Cycle 1, Day 15 Parameter (Units) 30 mg (n = 4) 45 mg (n = 3) 60 mg (n = 6) Tmax (hr) 1.5 (1.5 - 3.83) 2 (1.07 - 2.87) 3 (0.533 - 7.12) Cmax (ng/mL) 417 (39.9%) 273 (64.7%) 493 (31.8%) AUCtau (ng*hr/mL) 1560 (70.6%) 1740 (35.6%) 2280 (16.6%) CL/F (L/hr) 19.3 (70.6%) 25.8 (35.6%) 26.3 (16.6%) Vz/F (L) 83.9 (67.7%) 152 (17.4%) 140 (35.5%) Accumulation 1.48 (25.9%) 1.51 (0.485%) 1.14 (7.54%) Values are geometric mean (%CV) for all parameters except Tmax which is median (min-max). Day 15 values for 80 mg BID dose group were not calculable due to low n. Exposure of MEK162 increased in a dose-proportional manner. MEK162 was absorbed quickly, on average reaching maximum concentrations in plasma within ~2 hours of dosing. The between-patient reproducibility of exposure was similar on Day 1 (31% CV) to that on Day 15 of dosing (40% CV). No indication of nonlinear PK; modest accumulation on repeat dosing (32% increase, 20% CV). Mean plasma concentrations of MEK162 were maintained above the in vitro IC50 for cell proliferation continuously at all dose levels studied with twice-daily dosing. These PK results, the first reported for MEK162 in an oncology setting, are equivalent to those observed in healthy subjects, suggesting minimal effect on PK due to disease state. MEK162 Day 15 Dose Proportionality MEK162 Day 15 Concentrations versus Time 60 mg 30 mg 45 mg In vitro IC50 Time (hr) MEK162 AUCinf (hr*ng/mL) AACR-NCI-EORTC, Nov 12-16, 2011, San Francisco, CA MEK162 Geometric Mean Plasma Concentration (ng/mL) Abstract # B243 MEK162 BID dose Case Study: Partial Response, Cholangiocarcinoma Pharmacodynamics Case history: 57-year-old male (ECOG 0) with metastatic intrahepatic cholangiocarcinoma, diagnosed in Jun 2005. Prior treatment included initial surgical resection then followed by partial hepatic resection with radiofrequency ablation in Dec 2006, treated with 4 previous lines of chemotherapy for metastatic disease (gemcitabine + cisplatin, capecitabine + radiation therapy, paclitaxel + lapatinib+ pazopanib, capecitabine + LBH 589). Baseline tumor sites in pancreas (target) and liver (non-target). MEK162 was initiated at 80 mg BID. Main AEs included: G3 facial and body rash events that required both dose interruptions and dose reductions within the first 3 months of study drug treatment. Total duration of treatment was 16.6 months. RECIST v1.1: PR, duration 10.2 months. Molecular profile: NRAS (Q61R) mutation (archival sample). Overall long-term sustained reductions in both TNFα and IL6 relative to baseline. Circulating TNFα levels sensitive to dosing interruptions. Preliminary data: Circulating cytokines: TNFα showed a consistent, roughly dose-responsive decrease with treatment. Skin biopsy markers: Substantial, but not dose-responsive, decreases in Ki67 were seen, consistent with inhibition of cell proliferation. A dose-responsive decrease in pERK was observed. Summary MEK162 had an acceptable safety profile at doses up to the MTD of 60 mg BID and showed preliminary signs of clinical activity. MEK162 displayed desirable PK properties with dose-dependent exposures and preliminary evidence of MEK-related PD marker changes. An expansion phase of the study is ongoing in order to further explore toxicity and PK in patients with biliary cancer and in patients with KRAS- or BRAF-mutant metastatic colorectal cancer. We Thank the Patients and Their Families