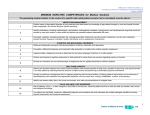
Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Age Related Conditions and Geriatric Assessment Alaa Mira, MD, CMD Chief of Geriatrics St. Luke’s University Health Network Disclosure Statement of Financial Interest I do not have financial relationships with commercial interests to disclose Learning Objectives • • • • Review common Geriatric syndromes Principles of Geriatric assessment Hazards of hospitalization of older adults Geriatric care models Older Adults are Hospitals’ CORE Consumers • Older adults 13% of the population: - But comprise 37% of hospital discharges and 43% of hospital days - Have longer lengths of stay (7.8 days vs. 5.4 days) - Higher rates of 30 day hospital re-admissions - Higher rates of functional decline and medical errors Risk Ratios for Activities of Daily Living Dependency 8 7 6 Risk Ratios 5 4 chronic diseases 3 2 1 0 1 2 >3 Number of chronic diseases Cigolle, C. T. et. al. Ann Intern Med 2007;147:156-164 Risk Ratios for Activities of Daily Living Dependency 8 7 6 Risk Ratios 5 geriatric condtions 4 3 chronic diseases 2 1 0 1 2 >3 Number of conditions/diseases Cigolle, C. T. et. al. Ann Intern Med 2007;147:156-164 Geriatric Syndromes • • • • • • • • • Dementia Depression Delirium Falls Sensory impairment Polypharmacy Incontinence Sleep disorders Weight loss Dementia: A Growing Epidemic Understanding Dementia • Dementia is a general term used to describe a decline in cognitive function • Progressive irreversible brain disease • No medication can cure dementia • Alzheimer’s disease is the most common form of dementia • Caregiver burnout Diagnostic Challenges • Is this “normal aging”? Is it a change? How Is Memory Affected By Aging • As we age, the brain loses some of its abilities that can lead to forgetfulness – This is normal, and begins after the age of 40 – Not progressive – No decline in activities of daily living – Productive and satisfying life Diagnostic Challenges • Is this “normal aging”? Is it a change? • Clinical presentations can be similar Conditions that Mimic Dementia Toxic/Metabolic • B12 deficiency • Hypothyroidism • Medications Systemic Illnesses • Infections • Cardiovascular disease • Pulmonary Other • Depression • Psychosocial stressors • Drugs Diagnostic Challenges • Is this “normal aging”? Is it a change? • Clinical presentations can be similar • Changes can begin up to 20 years before noticeable by self & others Stages of Dementia Normal Cognition Very Mild Cognitive Impairment Mild Cognitive Impairment Moderate Cognitive Impairment Severe Cognitive Impairment Stages of Dementia Normal Cognition Very Mild Cognitive Impairment Mild Cognitive Impairment Moderate Cognitive Impairment Severe Cognitive Impairment Is it worth screening for Alzheimer’s disease or MCI? “If there was treatment for AD, I'd recommend screening, but there is no disease-modifying therapy." “All older adults benefit from memory screening because it detects cognitive problems before memory loss is noticeable.” Healthy Aging, 2008; repost, 2010 “Memory Screening: Is it Worth It?” Reasons to Screen and Diagnosis Dementia Early • • • • • • Autonomy (right to know) Patient can participate in planning and decision making Lifestyle modification Advance directives Patient/caregiver education Access to information, programs, support, and other resources • Symptomatic and disease modifying therapies are more efficacious with early disease intervention • Medications Screening Tools For Dementia Name Mini-Cog Items/ Scoring 2 items Score = 5 Domains assessed Visuospatial, executive function, recall Web link (accessed Oct 2012) http://geriatrics.uthscsa.edu/tools /MINICog.pdf SLUMS 11 items Score = 30 Orientation, recall, calculation, naming, attention, executive function http://medschool.slu.edu/agingsuc cessfully/pdfsurveys/slumsexam_0 5.pdf MoCA 12 items Score = 30 www.mocatest.org Folstein MMSE 19 items Score = 30 Orientation, recall, attention, naming, repetition, verbal fluency, abstraction, executive function, visuospatial Orientation, registration, attention, recall, naming, repetition, 3-step command, language, visuospatial For purchase: www.minimental.com Clock Test Treatment • Non-pharmacologic treatment • Lifestyle modifications • Physical therapy and exercise • Socializing • Pharmacologic treatment • No medication can CURE dementia • Medication may slow down the dementia • Treatment should be individualized Delirium • Also known as – Acute mental status change – Acute confusional state – Altered mental status – Toxic or metabolic encephalopathy – Organic brain syndrome Delirium is most frequent complication of hospitalized elderly Yet it is underdiagnosed Prevalence • Hospitalized medically ill 10-30% • Hospitalized elderly 10-40% • Postoperative patients up to 50% • Near-death terminal patients up to 80% Risk Factors • • • • • • • Age Preexisting dementia Recent surgery Infections Visual/hearing impairment Polypharmacy Substance Abuse Types of Delirium • Hyperactive -Better recognized -More attention to treatment -Associated with improved outcome • Hypoactive -Little recognized -Depression is primary differential -Associated with poor outcomes • Mixed Clinical features • • • • • • • Prodrome Fluctuating course Attentional deficits Impaired cognition Sleep-wake disturbance Altered perceptions Affective disturbances Diagnosis of Delirium • • • • Delirium is a clinical diagnosis History and physical examination Mental Status Exam Confusion Assessment Method (CAM) • Standardized assessment tool • CAM ICU-non-verbal, ventilated patients • Identifies 4 features of the disorder -Acute onset or fluctuating -Inattention -Disorganized thinking -Altered level of consciousness Delirium: Management • Behavioral/Environmental Strategies – Reorientation, calendars, clocks – Room near nursing station – Lights on/off during day/night – Windows – Family/familiarity – Hearing aids, glasses – Avoid restraints Pharmacological Therapy • Nothing FDA-approved • Antipsychotics are treatment of choice for agitation compromising care or safety • Haloperidol best studied, widely used • Atypical Antipsychotics: Risperidone, Olanzapine, Quetiapine • Black box warning - Increased risk of death/CVA in patients with dementia Complications • Increased morbidity • Increased risk of cognitive decline • Increased risk of mortality • Nursing home placement Falls Aging and Falls • 30-40% of older adults fall every year • 20-30% of people who fall suffer moderate to severe injuries • 50% of fallers will report recurrent falls • 50-60% of falls happens in or around the home • Incidence of falling increases with age Central Processing Learning Experience Balance Sensory Input Visual Vestibular Somatosensation Motor Output Neural activation Muscle strength Range of motion Reflexes Falls are Multifactorial Intrinsic Factors Extrinsic Factors Age related changes Medications FALLS Medical conditions Environment Medication and Falls Risk Group Sedatives and hypnotics Antipsychotics Antidepressants Drugs with anticholinergic side effects Drugs for Parkinson’s disease Common Drug Names Contributing Factors Possible Actions for Prescribers Tricyclics - amitriptyline, dosulepin (Dothiepin), imipramine, lofepramine Other sedating – trazadone, mirtazepine Orthostatic hypotension, sedation which can last into the next day, lightheadedness, slow reactions, impaired balance, confusion orthostatic hypotension, confusion, drowsiness, slow reflexes, loss balance. Long term use - Parkinsonian symptoms. Double risk of falls Drowsiness, blurred vision, dizziness, orthostatic hypotension, constipation, urinary retention SnRI – venlafaxine and MAOI Orthostatic hypotension (OH) Dizziness, blurred vision, retention of urine, confusion, drowsiness, hallucinations. Sudden daytime sleepiness, dizziness, insomnia, confusion, low blood pressure, orthostatic hypotension, blurred vision. Temazepam, diazepam, lorazepam, nitrazepam Zopiclone, Zolpidem, chlordiazepoxide, chloral betaine (Welldorm), clomethiazole Chlorpromazine, haloperidol, lithium, promazine, trifluoperazine, quetiapine, olanzapine, risperidone SSRI – citalopram, fluoxetine Procyclidine, trihexyphenidyl (Benzhexol), prochlorperazine, oxybutynin, tolterodine Co-beneldopa, co-careldopa, rotigotine, amantadine, entacapone, selegiline, rivastigmine. Movement disorder with long term use Sedating, orthostatic hypotension ACE inhibitors/Angiotensin-II antagonists Ramipril, lisinopril, captopril, irbesartan, candesartan Vasodilators - Hydralazine Diuretics - bendroflumethiazide, bumetanide, indapamide, furosemide, amiloride, spironolactone, metolazone. Beta-blockers - Atenolol, bisoprolol, carvedilol, propranolol, sotalol Alpha-blockers - doxazosin, alfuzosin, terazosin, tamsulosin Low blood pressure, orthostatic hypotension, dizziness, tiredness, sleepiness, confusion, hyponatraemia, hypokalaemia Codeine, tramadol. Drowsiness, confusion, hallucinations, orthostatic hypotension, slow reactions Unsteadiness & ataxia if levels high Phenytoin – permanent cerebellar damage and unsteadiness in long term use Vestibular Sedatives Phenothiazines – prochlorperazine Cardiovascular drugs Analgesics Antihistamines- cinnarazine, betahistine Opiates – morphine, oxycodone. Anti-epileptics Carbamazepine*, phenytoin*, phenobarbitone*, primidone* sodium valproate*, gabapentin lamotrigine, topiramate, levatiracetam, pregabalin Bradycardia, hypotension, orthostatic hypotension, syncope Newer agents – insufficient data regarding falls risk Stop if possible Long term use will need slow, supervised withdrawal No new initiation Review indication and stop if possible (may need specialist opinion/support) Reduce dose/frequency if unable to stop Review indication (do not use amitriptyline as night sedation) Stop if possible, may need slow supervised withdrawal Populations studies show increased falls risk with SSRI but mechanism unclear, probably safest class to use Review indication Reduce dose or stop Check L&S BP, drugs and PD itself can cause OH Poorly controlled PD can cause falls It may not be possible to change the medication Do not change treatment without specialist advice Do not use long term – no evidence of benefit Check L&S BP Review indication, use alternative if possible, especially for alpha blocker Reduce dose if possible Symptomatic OH + LVF – if systolic LVF then try to maintain ACEi and β Blocker as survival benefit clear. Stop nitrates, CCB, other vasodilators and if no fluid overload reduce or stop diuretics. Seek specialist advice if needed Start low, go slow, review dose and indication regularly Consider indication (many used for pain or mood) May need specialist review *Consider Vitamin D supplements for at risk patients on long term treatment with these drugs Never stop or withhold medication without agreement from the medical team Adapted from © The Ipswich Hospital NHS Trust, April 2014.Dr Julie Brache. All rights reserved. Not to be reproduced in whole, or in part, without the permission of the copyright owner. Medication and Falls Risk All patients who present with a fall must have a medication review with modification/withdrawal (NICE CG 161) Whilst any medication changes will be finally decided by the doctor (GP or consultant) anyone working in falls can help to make this review as useful as possible: Take a comprehensive list of all medications currently taken (NB this should be what they actually take, not what has been prescribed!). Anyone on FOUR or more medications are at increased risk of falls. Check the patient’s understanding of their medication and how they take them. Consider concordance and compliance aids. Check lying and standing BP (5 mins lying down, check BP, stand, check BP then every minute for 3 minutes). A drop of 20 systolic or 10 diastolic is abnormal. Record any symptoms experienced and send this in to the doctor who is doing the medication review. Look for high or moderate risk drugs – see chart and highlight these for the doctor. Medication review: Is it still the right drug? (eg methyl dopa should no longer be used for hypertension) Is it still necessary? (eg analgesia given for acute flare OA, now resolved) Is it a moderate or high risk drug (see chart)? If so what is the risk/balance ratio? Is there a safer alternative? Could the dose be reduced? (eg 5mg bendroflumethiazide no significant increase in antihypertensive effects, but significant increase in side effects compared with 2.5mg) Should they be on calcium and vitamin D? – Ca and Vit D (800iu daily) reduce falls by up to 20% by improving muscle function and reducing body sway. Consider vitamin D level in patients with falls over age 65 (see pathway for management of deficiency). Consider supplements in all people who fall and are housebound or in residential or nursing homes. Don’t forget osteoporosis risk assessment / treatment. Stopping or reducing medication isn’t always easy and requires commitment and understanding by the prescriber and patient. Advice on complex cases is always available from the consultant geriatricians at Ipswich Hospital, in the community sessions or via the Rapid Assessment Falls Clinic. The attached table is provided as a guide to medication review in falls only. Each patient must be assessed as an individual and the risk/benefit for each drug considered and discussed and a decision made by the prescriber in consultation with the patient. Higher risk drugs Moderate risk drugs Never stop or withhold medication without agreement from the medical team Adapted from © The Ipswich Hospital NHS Trust, April 2014.Dr Julie Brache. All rights reserved. Not to be reproduced in whole, or in part, without the permission of the copyright owner. Subjects in the Intervention and Control Groups Who Had Multifactorial Intervention to Reduce the Tinetti M et al. N Engl J Med 1994;331:821-827 Risk of FallingtagesO Effect of Vitamin D on Falls • Meta-analysis included 5 RCTs with 1237 elderly individuals treated with different vit D analogues for 2 months to 3 years • Vitamin D supplementation reduced the risk of falls among the elderly by 22% • Improved the body sway by 9% and musculoskeletal function by 11% • 400 IU of vit D may not be clinically effective • Trials used 800 IU of vit D did find significant reductions in observed fractures Heike et al. JAMA 2004; 291;1999-2006 Comprehensive Geriatric Assessment • Multi-disciplinary team approach • Address the unique needs of older adults • Work collaboratively with PCP and other specialists • Patient and family centered care • Improve satisfaction and quality of life St. Luke’s Senior Care Services • • • • Center for positive aging Acute Care for the Elderly (ACE) Geriatrics surgical program Nurses Improving Care of Healthsystem Elders (NICHE) Center for Positive Aging • Comprehensive Geriatric assessment • Multi-disciplinary approach • Social worker • Driving issues • Pre-operative assessment • Family care conference • Recommendations to PCP Acute Care for the Elderly (ACE) ACE Model Concepts • • • • • • • • Specialized model of care Address the needs of hospitalized older adults Evidence based best practice Multi-disciplinary team approach Prevent functional decline and NH placement Reduce iatrogenic complications Decrease hospital length of stay and costs Improve outcomes and satisfaction ACE Consult Criteria • • • • • 65 years or older Acutely ill Co-morbid conditions At risk of functional decline Identification seniors at risk (ISAR) tool St. Luke’s ACE Outcome Data 2014 • Ativan orders decreased by 33% • Benadryl orders decreased by 13% • LOS decreased by 10% • Delirium rate decreased by 60% Geriatrics Surgical Program • Pre-operative geriatric assessment • Nurse navigator • 65 years or older • Elective surgery • Geriatric assessment • Update anesthesiologists and surgeons Nurses Improving Care for Healthsystem Elders (NICHE) • NICHE is a program of the Hartford Institute at the NYU College of Nursing • NICHE is the only national geriatric nursing program that addresses the needs of hospitalized older adults • There are approximately 680 hospitals in more than 40 states as well as Canada with NICHE designation NICHE Program • Goal – Achieve systematic nursing change that will benefit hospitalized older adults • Vision – Provide geriatric sensitive and exemplary care to all hospitalized older adults • Mission – Import principles and tools to stimulate change in the culture of healthcare facilities to achieve patientcentered care for older adults Nurses are Positioned to Paly a Central Role • Nurses are the primary caregivers for older patient in hospitals • Nurses are generally not fully prepared to care for older patients • Nursing models can improve older patients’ care and decrease hospital complications • Nursing can be the focal point for stimulating interdisciplinary care NICHE Resources • Start-up tools – NICHE planning and implementation guide – Leadership training program • Measurement – Geriatric Institutional Assessment Profile (GIAP) – Clinical outcomes – Program self-evaluation • Clinical management tools – Organizational strategies and clinical improvement models • Training and education programs – Care curricula: for nurses, patient care techs (CNA), other disciplines and general staff – – – – Webinars and in-service materials Educational resources for patients and families Conferences Geriatric Resource Nurse (GRN) • National community Geriatric Resource Nurse (GRN) • Certified GRN • Assist staff in evaluating, planning and implementing geriatric care • Disseminate information about geriatric care • GRN core screening tool (SPICES) • Geriatric assessment rounding NICHE Outcomes • Enhance nursing knowledge and skills regarding the treatment of common geriatric syndromes • Increase patient satisfaction • Decrease length of stay • Reduce readmission rates • Reduce costs associated with elder care St. Luke’s Network and NICHE Program • St. Luke’s became NICHE designated in Jan 2014 • RNs and Patient Care Assistants completed the NICHE Geriatric Resource Education and St Luke’s older adult sensitization • Non-nursing staff received NICHE information and sensitization experiences • Network-wide Geriatric Institutional Assessment 70% completion rate • St. Luke’s NICHE Program video viewed by over 1100 employees St. Luke’s Network Performance Improvement Activities • Reducing polypharmacy in older adults • Effective ambulation and reducing deconditioning • Reducing pressure ulcers • Reducing delirium Fall Rate Outcomes 4.5 Network Fall Rate/1000 pt days 4 3.5 3 2.5 2 1.5 1 0.5 0 2013 2014 Fasical Year 2015 Conclusions • Multidisciplinary team approach is recommended to coordinate the care of older adults • Geriatric syndromes are prevalent • Geriatric assessment improves outcomes • Geriatric care models (ACE/NICHE) decrease functional decline, falls, polypharmacy, LOS and increase satisfaction “In the end, it’s not the years in your life that count. It’s the life in your years.” Abraham Lincoln “Thank You”