Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
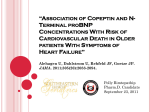
Clinical Chemistry 55:5 923–929 (2009) Proteomics and Protein Markers Variability of N-Terminal Probrain Natriuretic Peptide in Stable Chronic Heart Failure and Its Relation to Changes in Clinical Variables Lutz Frankenstein,1* Andrew Remppis,1 Joerdis Frankenstein,2 Georg Hess,3 Dietmar Zdunek,4 Karen Slottje,1 Hugo A. Katus,1 and Christian Zugck1 BACKGROUND: We investigated the variability of N-terminal probrain natriuretic peptide (NT-proBNP) and its relation to known confounding variables in patients with stable chronic heart failure who were on a stable optimized medication regimen. METHODS: At 4 sampling intervals (14-day, 1-month, 2-month, and 3-month) the results for NT-proBNP measurements and several clinical variables were measured in samples from 41 patients with chronic systolic dysfunction who met 21 prespecified criteria for stability. RESULTS: Mean within-person NT-proBNP variabilities expressed as percentage CV were 17.6%, 18.9%, 15.5%, and 16.2% at 14-day, 1-month, 2-month, and 3-month follow-up, respectively, and the corresponding reference change values were 34.6%, 52.5%, 43.1%, and 45.0%, respectively. Within-person variability of NT-proBNP was not found to be associated with renal function, weight, or waist circumference. Likewise, age, sex, baseline NT-proBNP, New York Heart Association functional class, and ejection fraction did not influence variability of NT-proBNP. The index of individuality ranged from 0.07– 0.15 depending on the time interval between test results. CONCLUSIONS: Although other reported studies have revealed variations in the range of 80%, in this prespecified stable heart-failure population variation of NTproBNP at 14-day, 1-month, 2-month, and 3-month follow-up was lower and was not related to renal function or weight. In view of the low index of individuality we observed, within-person variation is quite low compared to between-person variation. Consideration of these facts is important for the interpretation of clinical 1 Department of Cardiology, Angiology, and Pulmonology; University of Heidelberg; Germany; 2 Lehrstuhl für Pharmazeutische Biologie; Friedrich-AlexanderUniversität Erlangen-Nürnberg; Germany; 3 Roche Diagnostics, Mannheim, Germany; 4 Roche Diagnostics, Rotkreuz, Switzerland. * Address correspondence to this author at: Department of Cardiology, Angiology, Pulmonology, University of Heidelberg, Im Neuenheimer Feld 410, D-69120 Heidelberg, Germany. Fax 0049-6221-56-6547; e-mail Lutz. trials and the use of NT-proBNP in monitoring patients with heart failure. © 2009 American Association for Clinical Chemistry Serial measurement of natriuretic peptides in heart failure patients has been suggested to have utility both for the guidance of management strategies (1–5 ) and for improved prognostication (6, 7 ). This application, however, relies on knowledge about the corresponding biological variation at the respective follow-up interval chosen. To date, such intermediate-term variations are largely unknown because studies assessing biological variability in heart failure patients have either examined short-term (week-to-week) variations (8–11 ) or long-term (year-to-year) variations (12, 13 ). Because patients in the outpatient setting are rarely seen on a weekly or a yearly basis, this gap in knowledge of intermediate-term variability must be addressed. Results of prior studies suggest that short-term variability of natriuretic peptides is high (8–11 ) and reference change values (RCVs)5—the percentage of change of hormonal level considered to be of possible diagnostic or prognostic importance— have been found to exceed 100% of the initial value (11 ). These high values are controversial (12 ) because they appear to be related to the skewed distribution of measured hormonal values and improve after normalizing transformation of the data (13 ). Furthermore, the biological variation of brain natriuretic peptide (BNP) appears to be greater than that of N-terminal pro-BNP (NTproBNP) (14 ). Of those studies in which very large within-person variations were observed, only 2 (9, 11 ) have included patients with heart failure. Investigation of natriuretic peptide variations in heart failure patients is important [email protected]. Received June 5, 2008; accepted February 11, 2009. Previously published online at DOI: 10.1373/clinchem.2008.112052 5 Nonstandard abbreviations: RCV, reference change value; BNP, brain natriuretic peptide; NT-proBNP, N-terminal pro-BNP; NYHA, New York Heart Association; GFR, glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; IOI, index of individuality. 923 because patients with heart failure have much higher baseline hormonal values and when these patients are clinically stable, their within-person variability expressed in terms of CV would be expected to be substantially lower than that of healthy individuals. In patients undergoing treatment for heart failure, stability of medication and adherence to guidelines are important aspects to consider because, for example, administration of -blockers could significantly influence BNP levels (15 ). Furthermore, stability of clinical state—the prerequisite for determination of biovariability—might be difficult to ascertain in heart failure patients, especially with longer intervals between tests. Because adherence to guidelines has been incomplete in previous studies and stability of chronic heart failure has not always been confirmed by direct assessment, we prospectively investigated in an outpatient setting the intermediate-term variability of NTproBNP in patients with stable chronic heart failure who were undergoing treatment with individually optimized stable medication regimens. Materials and Methods This study constitutes the NT-proBNP arm of a multimarker project on neurohumoral pathways in chronic heart failure. The local ethics committee approved the project, which conforms to the principles of the declaration of Helsinki. Patients were recruited prospectively and continuously from the heart failure outpatient clinic of the University Hospital Heidelberg, Germany. Between September 2006 and June 2007, all patients being seen in follow-up visits to the clinic (n ⫽ 766 patients) were screened for eligibility. A total of 90 patients fulfilled the criteria for inclusion in the study described below. Of these, 43 patients consented to the study protocol. Two patients withdrew their consent after the first visit. Therefore, the final study population consisted of 41 patients. At 3-month-follow-up, 3 patients showed significant unexplained weight loss compared to 1-month follow-up. In accordance with the study protocol, they remained in the data set for 1-month follow-up because they were stable in all other parameters up to that time, but were excluded from further analysis at 2-month and 3-month follow-up, although they were stable according to all other criteria, including self-perceived clinical status. Therefore, at 3-month-follow-up the final study populations consisted of 38 patients. The diagnosis of heart failure was established according to published guidelines (16 ), and the etiology was confirmed by results of cardiac catheterization, which was performed in all patients during first contact with our clinic. Patients were eligible if they met all of 924 Clinical Chemistry 55:5 (2009) the following criteria: (a) chronic heart failure known for at least 1 year followed at our clinic; (b) stable clinical condition with no hospitalization attributable to worsening heart failure within the previous 6 months; (c) New York Heart Association (NYHA) functional class I–III; (d) subjectively stable clinical condition since the last visit to the outpatient clinic, as judged both by the patient and the physician; (e) ischemic or idiopathic dilated cardiomyopathy as the etiology of heart failure; (f) in case of ischemic origin, no revascularization performed within the previous 6 months and no revascularization planned during the next 6 months; (g) age ⬎18 years; (h) complete adherence to guidelines of medical treatment regarding class of drugs; (i) individually optimized doses of guidelinerecommended drugs for at least 4 weeks before study inclusion; (j) no recent involuntary change of weight exceeding 2 kg within 4 weeks before inclusion; and (k) serum sodium levels within reference intervals, indicating euvolemic state. Patients were excluded if they met 1 or more of the following criteria: (a) pregnancy, (b) significant renal dysfunction as identified by a creatinine concentration ⬎176.8 mol/L (2 mg/dL), (c) unstable renal function as identified by a change in creatinine ⬎20% since the last visit, (d) thyroid dysfunction, (e) history of pulmonary disease, (f) valvular heart disease, (g) inability to cooperate or to comprehend the study protocol, (h) active listing for cardiac transplantation, (i) primary pulmonary hypertension, (j) in cases of ischemic origin: angina, angina-equivalent, or ischemia-induced changes in the electrocardiogram during bicycle exercise testing of at least 7 MET (metabolic equivalent test). Blood samples for NT-proBNP analysis were taken from an indwelling venous catheter after patients had rested for a period of 30 min. The time of sample collection was between 2 and 4 PM, because NTproBNP has been demonstrated to be stable during the afternoon (9 ). After the initial visit (T0), patients were seen again after 2 weeks and 4 weeks (T1 and T2) and again after 12 weeks (T3). For T1 and T2, a delay of 2 days was allowed, and for T3, a delay of 4 days. EDTA Vacutainer tubes were used, and samples were centrifuged at 4 °C immediately after collection to separate the plasma, which was frozen at ⫺20 °C. NT-proBNP was measured by use of a fully automated Elecsys® Roche Diagnostics 2010 analyzer. Assay precision, analytical sensitivity, interferences, and stability for this method have been previously described (17, 18 ). To minimize the analytical variance, all samples were analyzed together in 1 run. We determined within-run imprecision by using samples from our study patients and synthetic controls. The CVs for analysis of 21 aliquots of each sample—again, all sam- Biovariability of NT-proBNP in Stable Heart Failure ples within 1 assay run—were 1.6% (sample mean, 137 ng/L), 1.8% (sample mean, 150 ng/L), 1.0% (sample mean, 581 ng/L), 1.2% (sample mean, 1222 ng/L), and 1.5% (sample mean, 5239 ng/L), giving a total variation of 1.4%. NT-proBNP results are presented in nanograms per liter. To convert to picomoles per liter, multiply results by 0.118. NT-proBNP was considered as a continuous variable for all calculations. Renal function was assessed both by serum creatinine concentrations and glomerular filtration rate (GFR) as estimated by the simplified Modification of Diet in Renal Disease (MDRD) formula (19, 20 ). The total CV (CVt) and the analytical CV (CVa) provided the basis for calculating the individual biological CV (CVi) where CVi ⫽ (CVt2 – CVa2)[1/2]. The CV was calculated as CV ⫽ 100 ⫻ (SD/mean). RCVs were calculated from median CVt values, according to the formula: RCV ⫽ Z ⫻ 2[1/2] (CVa2/na ⫹ CVi2/ns)[1/2], where Z ⫽ 1.96 (i.e., the Z-score for 95% confidence with a 2-tailed P ⬍ 0.05); na is the number of replicate assays; and ns is the number of patient samples to estimate each of the 2 homeostatic set points. The index of individuality (IOI) was calculated as: IOI ⫽ (CVa2 ⫹ CVi2)[1/2]/CVG (⫽ intraindividual variance⫹analytical variance/interindividual variance) (21, 22 ). Here, a low IOI (⬍0.48) is considered to reflect strong individuality, which in turn indicates that an individual patient should be assessed with respect to his or her individual hormonal level. In contrast, a high IOI (⬎1.4) indicates that this patient should be assessed with respect to population-derived reference intervals (21 ). Continuous data were tested by use of the 2-sample Wilcoxon test, Kruskal–Wallis-test, and 1-way ANOVA, as appropriate. Univariable and multivariable linear regressions were performed by using uncorrected or log-transformed values for the dependent variable, as appropriate, and the Spearman method was used to assess correlations between variables. The relation between relative change and hormonal level was assessed according to the method proposed by Bland and Altman (23, 24 ). An arbitrary level of 5% statistical significance (P ⬍ 0.05; 2-tailed) was assumed throughout. Calculations were performed with SAS version 9.1. Results Our patients represent the average population at a tertiary reference center. Dilated cardiomyopathy was the predominant clinical presentation in this population, which included 80% men with a mean age of 61 years. The majority of patients fell into NYHA functional classes I and II. For complete characteristics see Table 1. At all 4 sampling intervals, patients were stable with Table 1. Patient characteristics at study inclusion. Parameter Value Patients, n 41 Men, n (%) 33 (80) Age, y 61 ⫾ 10 Ischemic heart disease, n (%) 17 (41) NYHA I, n (%) 9 (22) NYHA II, n (%) 29 (71) NYHA III, n (%) 3 (7) LVEF,a % 33 ⫾ 10 Body mass index, kg/m2 28.2 ⫾ 4.6 102.5 ⫾ 11.1 Waist, cm Systolic blood pressure, mmHg 111 ⫾ 17 Diastolic blood pressure, mmHg 72 ⫾ 10 Heart rate, beats/min NT-proBNP, ng/L 68 ⫾ 11 597 (257–1306) 139 ⫾ 3 Sodium, mmol/L Creatinine, mol/L 108.0 ⫾ 25.7 MDRD-estimated GFR, mL/min 59 ⫾ 17 Medication a ACEI or ARB, n (%) 41 (100) -Blocker, n (%) 40 (98) Aldosterone antagonist, n (%) 28 (68) Diuretics, n (%) 25 (61) LVEF, left ventricular ejection fraction; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker. regard to weight (P ⫽ 0.99), waist circumference (P ⫽ 0.94), renal function (P ⫽ 0.94 for creatinine; P ⫽ 0.90 for MDRD-estimated GFR), serum sodium concentration (P ⫽ 0.71), blood pressure (P ⫽ 0.82 for systolic; P ⫽ 0.17 for diastolic), heart rate (P ⫽ 0.47), and NTproBNP (P ⫽ 0.99). No changes in medication or NYHA functional class occurred. For a complete data profile according to sample interval, see Table 2. In this population of stable heart failure patients, NT-proBNP showed biological variability of 11.3% to 18.9% depending on the time interval between tests. Corresponding RCVs were between 31.4% and 52.5%. The indices of individuality ranged from 0.07– 0.12. More detailed results are available in Table 3. CVs for the 4 test intervals showed a variable pattern of intercorrelation. Whereas 2-month coefficients did not correlate with other coefficients (r ⫽ 0.17, P ⫽ 0.28 vs 14-day; r ⫽ 0.21, P ⫽ 0.20 vs 1-month; r ⫽ 0.22; P ⫽ 0.17 vs 3-month), all other coefficients were found to be intercorrelated: 14-day coefficients correlated with 1-month (r ⫽ 0.66, P ⬍ 0.001) and 3-month (r ⫽ 0.45, P ⬍ 0.01) coefficients and 1-month coefficients correClinical Chemistry 55:5 (2009) 925 Table 2. Patient characteristics during serial sampling.a Parameter Initial visit 14-days 28-days 90-days NYHA I, n (%) 9 (22) 9 (22) 9 (22) 9 (22) NYHA II, n (%) 29 (71) 29 (71) 29 (71) 29 (71) NYHA III, n (%) Body mass index, kg/m2 3 (7) 3 (7) 3 (7) 3 (7) 28.2 ⫾ 4.6 28.2 ⫾ 4.7 28.2 ⫾ 4.7 28.3 ⫾ 4.9 102.5 ⫾ 11.1 102.4 ⫾ 11.3 101.1 ⫾ 11.3 100.7 ⫾ 11.3 Systolic blood pressure, mmHg 111 ⫾ 17 112 ⫾ 17 110 ⫾ 17 111 ⫾ 18 Diastolic blood pressure, mmHg 72 ⫾ 10 69 ⫾ 8 67 ⫾ 10 69 ⫾ 11 Heart rate, beats/min 68 ⫾ 11 67 ⫾ 9 67 ⫾ 11 68 ⫾ 9 NT-proBNP, ng/L 597 (257–1306) 582 (272–1538) 590 (286–1183) 520 (215–1494) Sodium, mmol/L 139 ⫾ 3 139 ⫾ 3 140 ⫾ 3 140 ⫾ 3 108.0 ⫾ 25.7 109.0 ⫾ 24.8 106.0 ⫾ 23.3 109.0 ⫾ 28.0 59 ⫾ 17 58 ⫾ 15 60 ⫾ 15 59 ⫾ 26 14.1 ⫾ 1.2 13.9 ⫾ 1.3 14.0 ⫾ 1.4 14.2 ⫾ 1.5 ACEIb or ARB, n (%) 41 (100) 41 (100) 41 (100) 41 (100) -Blocker, n (%) 40 (98) 40 (98) 40 (98) 40 (98) Aldosterone antagonist, n (%) 28 (68) 28 (68) 28 (68) 28 (68) Diuretics, n (%) 25 (61) 25 (61) 25 (61) 25 (61) Waist, cm Creatinine, mol/L MDRD-estimated GFR, mL/min Hemoglobin, mg/dL Medication a b No statistically significant differences were noted for any of the parameters across any of the test intervals. ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin-receptor blocker. lated with 3-month coefficients (r ⫽ 0.33, P ⬍ 0.05). We did not find any correlation between relative interval change in NT-proBNP and the corresponding interval changes in weight or waist circumference, renal function (as indicated by either serum creatinine or MDRD-estimated GFR), or heart rate at any of the 4 sampling intervals (data not shown). For hemoglobin, only the relative interval change at 3-month follow-up correlated with relative interval change in NT-proBNP (r ⫽ 0.49, P ⬍ 0.01), with no correlation found at the other sampling intervals. Regression analyses did not reveal any significant influence of baseline NT-proBNP concentrations on the corresponding change values (P ⫽ 0.38, P ⫽ 0.69, P ⫽ 0.18, and P ⫽ 0.48 for 14-day, 1-month, 2-month, and 3-month values, respectively). Consequently, no further subdivision according to NT-proBNP grouping was performed. The corresponding graphs can be Table 3. Analytical and biological variation, reference change values, and index of individuality of NTpro-BNP according to sampling interval.a Measurement interval 14 Days (A) 14 Days (B) 14 Days (comb) 28 Days 62 Days 90 Days b 14.2 ⫾ 0.5 13.9 ⫾ 0.9 14.1 ⫾ 0.6 28.1 ⫾ 1.2 63.4 ⫾ 2.9 91.5 ⫾ 2.9 CVt, % 18.5 (9.6–29.2) 11.4 (5.3–27.2) 17.7 (10.9–25.0) 19.0 (9.2–28.7) 15.6 (6.5–26.0) 16.3 (7.2–36.9) CVi, % 18.4 (9.5–29.2) 11.3 (5.1–27.2) 17.6 (10.8–25.0) 18.9 (9.1–28.7) 15.5 (6.3–26.0) 16.2 (7.1–36.9) RCV, % 51.1 31.4 34.6 52.5 43.1 45.0 tact, days IOI 0.11 a 0.07 0.11 0.12 0.09 0.10 No statistically significant differences were noted for CV values and IOI across any of the test intervals CV values are given as median (interquartile range); (A), first 14-day interval between measurements; (B), second 14-day interval between measurements; (comb), both 14-day intervals combined. b tact, Actually achieved time interval between measurements; CVt, total CV; CVi, individual biological CV. 926 Clinical Chemistry 55:5 (2009) Biovariability of NT-proBNP in Stable Heart Failure Fig. 1. Bland–Altman plot for NT-proBNP values of the 4 sampling intervals. The dotted lines indicate 1.96 ⫻ SD of the mean of the differences (95% confidence with P ⬍ 0.05). seen in Fig. 1. Likewise, NYHA functional class, sex, age, weight or waist circumference, heart rate, hemoglobin levels, and ejection fraction were not found to significantly influence the different change values (data not shown). Renal function, as indicated by either serum creatinine or MDRD-estimated GFR, was found to have a small but significant relationship with 14-day change values (-coefficient, ⫺0.18; SE, 0.08; intercept, 0.42; SE, 0.1; r 2, 0.12; residual SD, 0.13; P ⫽ 0.03 for creatinine; -coefficient, 0.003; SE, 0.001; intercept, 0.02; SE, 0.09; r 2, 0.12; residual SD, 0.13; P ⫽ 0.04 for MDRD-estimated GFR) with no significant relationship with the other change values (P ⫽ 0.29, P ⫽ 0.60, and P ⫽ 0.14 for 1-month, 2-month, and 3-month values of MDRD-estimated GFR, respectively). Discussion We determined the intermediate-term biological variation of NT-proBNP in stable chronic heart failure and its relation to change in known confounding variables. Importantly, we did so in an outpatient setting in patients who were on individually optimized stable medication regimens. We found that patients with stable chronic heart failure and on stable medication had NTproBNP biological variation of 11% to 20% with sampling periods ranging from 14 days to 3 months. We also found that the corresponding indices of individu- ality for these sampling periods ranged from 0.07– 0.15 and indicated high individuality of values. Lastly, the individual biological variability of NT-proBNP does not appear to be influenced by known confounders for NT-proBNP itself, such as NYHA functional class, sex, age, weight or waist circumference, hemoglobin levels, ejection fraction, or renal function. We chose to investigate NT-proBNP because it is more stable than BNP and its variation appears to be lower (14 ). Also, to the best of our knowledge, this is the first study to address biovariability of natriuretic peptides during intermediate follow-up intervals and only the second study to address indices of individuality in chronic heart failure. In patients the confounding effects of clinical stability and titration of drugs must be controlled to assess true biological variability. In this context it is interesting to note that only approximately one-ninth of patients attending our clinic were eligible – or inversely, about 90% of patients in an outpatient setting presented some degree of clinical instability. Previous reported studies on short- or long-term variability found RCVs around 100% (8, 9 ) (11 ), others found CVs between 20% and 30% (10, 12, 13, 25, 26 ). The key to understanding these results is the rigidity of the definition of stability of heart failure. In studies that expended large efforts to ascertain stability (12, 25, 26 ) the CVs found were lower than in studies with less strict criteria (9, 11 ). Consequently, we found Clinical Chemistry 55:5 (2009) 927 CVs for NT-proBNP to be around 20%. Our study is a valuable extension to current knowledge because intermediate-term variation must be quantified to aid interpretation of trials targeting guidance of medical therapy or routine application as they relate to normal follow-up duration in outpatient settings. Important points must be considered with regard to estimation of CVs for NT-proBNP. The skewed distribution of NT-proBNP values can be converted by log-transformation to a normal distribution (12, 25 ), a process that results in lower CVs and eliminates the problem of a paradoxical decrease ⬎100%. It must be emphasized, however, that CVs derived by this approach would apply only to log-transformed values, thus limiting clinical applicability. After retransformation as suggested by Fokkema et al. (27 ), the CV borders are comparable to those derived by use of nontransformed values. In addition, the CV of logtransformed values is not independent of the scale of the values, necessitating strict adherence to scale. A more important consideration is that the concept of biological variation around a homeostatic set-point might not hold for NT-proBNP (14 ). This could be the case because CVs for natriuretic peptides do not represent random variation, but rather the close balance between hemodynamics and neuroendocrine regulation vs counterregulation (28 ); pulsatile secretion of BNP (and consequently NT-proBNP) has already been demonstrated in healthy individuals (29 ). The interpretation of IOI has been reported previously (21 ) and is detailed above. So far, only 1 reported study (25 ) has included data on IOI in heart failure patients. As in the present study for intermediate follow-up, the earlier study demonstrated that IOIs of week-to-week variations were relatively low, paralleling our findings indicating that NT-proBNP shows high interindividual variation with relative stability of values for the individual patient. This relative stability of NT-proBNP in the individual patient compared to between-patient variability further strengthens the notion raised above that NT-proBNP might not vary randomly and could be an explanation for the difference between high CVs observed in stable patients vs small differences in serial NT-proBNP concentrations when these indices are successfully used in therapy-guiding trials (1, 2 ). Recently it has been suggested that the additional prognostic value of serial evaluation might be more related to a categorical change with respect to a cutoff concentration (6, 7 ) than to the use of relative or absolute changes in concentration. Despite the widespread use of natriuretic peptides, there is a paucity of data on possible confounders for serial measurements in patients with stable heart failure. We confirmed the only 2 available studies regarding the absence of influence of age, sex, and renal func928 Clinical Chemistry 55:5 (2009) tion on short-term (25 ) and long-term (13 ) variations of NT-proBNP and have extended these findings to important confounders such as NYHA functional categories and obesity as represented by weight and waist circumference. More importantly, we did not find any relationship between change of NT-proBNP and changes in renal function (either for serum creatinine or MDRD-estimated GFR) or body weight (as indicated by weight or waist circumference) at any of the 4 sampling intervals. Only medium-term, but not shortterm, changes in hemoglobin were found to be related to changes in NT-proBNP. Because hemoglobin influences NT-proBNP concentrations, it is possible that the short-term changes in hemoglobin measured here reflect biovariability or smaller changes in fluid intake that would not exert sizeable influence on NT-proBNP levels, whereas medium-term changes in hemoglobin might be a reflection of more slowly developing patterns (e.g., evolving anemia), which could influence NT-proBNP. These findings are important in clinical practice, in which change of NT-proBNP will be interpreted in light of other variables. Furthermore, such findings again provide indirect support for the notion that NT-proBNP does not vary randomly. Our study has several limitations. The relatively small number of patients included may hinder adequate statistical analysis, but the size of our study population is comparable to previous, related studies. In addition, the numerous and strict selection criteria should give this study even greater value, although these criteria might also adversely impact on clinical variables and patient selection, effectively reducing the number of individuals included in the study and possibly the clinical transferability of the findings. We think that RCVs should be established only in clinically stable patients to allow later application to more unstable settings. Loss of individuals from the study due to patients dropping out could have introduced possible bias to the study. We cannot completely rule out the presence of hidden hemodynamic changes; it is possible that undetected intermittent changes of rhythm contributed to the large variability seen in some patients and might explain some of the discrepancy between obvious clinical stability and large changes in measured marker values. Because we did not perform invasive testing or long-term Holter follow-up, we can only speculate about this possibility. Consequently, despite the rigorous definition of stability used in our study, it is still possible that we did not measure pure biological variability but that to a certain extent clinically undetected variations in phenotype may have been included in our determinations. In conclusion, despite previous reports of values around 80%, variation of NT-proBNP at 14-day, 1-month, 2-month, and 3-month follow-up is lower in Biovariability of NT-proBNP in Stable Heart Failure a prespecified population of patients with stable heart failure and is not related to changes in renal function or weight. In view of the low index of individuality we observed, within-person variation is quite low compared to between-person variation. Consideration of these facts is important for the interpretation of trials and the use of NT-proBNP in monitoring patients with heart failure. Author Contributions: All authors confirmed they have contributed to the intellectual content of this paper and have met the following 3 requirements: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; and (c) final approval of the published article. Authors’ Disclosures of Potential Conflicts of Interest: Upon manuscript submission, all authors completed the Disclosures of Potential Conflict of Interest form. Potential conflicts of interest: Employment or Leadership: G. Hess, Roche Diagnostics; D. Zdunek, Roche Diagnostics. Consultant or Advisory Role: None declared. Stock Ownership: None declared. Honoraria: C. Zugck, Novartis, Astrazeneca, PHTS, and Roche. Research Funding: C. Zugck, PHTS, Roche, and AOK. Expert Testimony: None declared. Role of Sponsor: The funding organizations played no role in the design of study, choice of enrolled patients, review and interpretation of data, or preparation or approval of manuscript. References 1. Troughton RW, Frampton CM, Yandle TG, Espiner EA, Nicholls MG, Richards AM. Treatment of heart failure guided by plasma aminoterminal terminal brain natriuretic peptide (N-BNP) concentrations. Lancet 2000;355:1126 –9. 2. Jourdain P, Jondeau G, Funck F, Gueffet P, Le Helloco A, Donal E, et al. Plasma brain natriuretic peptide-guided therapy to improve outcome in heart failure: the STARS-BNP Multicenter Study. J Am Coll Cardiol 2007;49:1733–9. 3. Lainchbury JG, Troughton RW, Frampton CM, Yandle TG, Hamid A, Nicholls MG, Richards AM. NTproBNP-guided drug treatment for chronic heart failure: design and methods in the “BATTLESCARRED” trial. Eur J Heart Fail 2006;8: 532– 8. 4. Bettencourt P, Friões F, Azevedo A, Dias P, Pimenta J, Rocha-Gonçalves F, Ferreira A. Prognostic information provided by serial measurements of brain natriuretic peptide in heart failure. Int J Cardiol 2004;93:45– 8. 5. Miller WL, Hartman KA, Burritt MF, Grill DE, Rodeheffer RJ, Burnett JC Jr, Jaffe AS. Serial biomarker measurements in ambulatory patients with chronic heart failure: the importance of change over time. Circulation 2007;116:249 –57. 6. Latini R, Masson S, Wong M, Barlera S, Carretta E, Staszewsky L, et al. Val-HeFT Investigators. Incremental prognostic value of changes in B-type natriuretic peptide in heart failure. Am J Med 2006;119:70.e23–30. 7. Masson S, Latini R, Anand IS, Barlera S, Angelici L, Vago T, et al. Val-HeFT Investigators. Prognostic value of changes in N-terminal pro-brain natriuretic peptide in Val-HeFT (Valsartan Heart Failure Trial). J Am Coll Cardiol 2008;52:997–1003. 8. Wu AH, Smith A. Biological variation of the natriuretic peptides and their role in monitoring patients with heart failure. Eur J Heart Fail 2004; 6:355– 8. 9. Bruins S, Fokkema MR, Römer JW, Dejongste MJ, van der Dijs FP, van den Ouweland JM, Muskiet FA. High intraindividual variation of B-type natriuretic peptide (BNP) and amino-terminal proBNP in patients with stable chronic heart failure. Clin Chem 2004;50:2052– 8. 10. O’Hanlon R, O’Shea P, Ledwidge M, O’Loughlin 11. 12. 13. 14. 15. 16. 17. 18. C, Lange S, Conlon C, et al. The biologic variability of B-type natriuretic peptide and N-terminal pro-B-type natriuretic peptide in stable heart failure patients. J Card Fail 2007;13:50 –5. Wu AH, Smith A, Wieczorek S, Mather JF, Duncan B, White CM, et al. Biological variation for N-terminal pro- and B-type natriuretic peptides and implications for therapeutic monitoring of patients with congestive heart failure. Am J Cardiol 2003;92:628 –31. Cortes R, Rivera M, Salvador A, Bertomeu V, de Burgos FG, Rosello-Lleti E, et al. Variability of NT-proBNP plasma and urine levels in patients with stable heart failure: a 2-year follow-up study. Heart 2007;93:957– 62. Schou M, Gustafsson F, Kjaer A, Hildebrandt PR. Long-term clinical variation of NT-proBNP in stable chronic heart failure patients. Eur Heart J 2007;28:177– 82. Clerico A, Carlo Zucchelli G, Pilo A, Passino C, Emdin M. Clinical relevance of biological variation: the lesson of brain natriuretic peptide (BNP) and NT-proBNP assay. Clin Chem Lab Med 2006;44:366 –78. Takeda Y, Fukutomi T, Suzuki S, Yamamoto K, Ogata M, Kondo H, et al. Effects of carvedilol on plasma B-type natriuretic peptide concentration and symptoms in patients with heart failure and preserved ejection fraction. Am J Cardiol 2004; 94:448 –53. Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M, et al. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): the Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J 2005;26:1115– 40. Yeo KT, Wu AH, Apple FS, Kroll MH, Christenson RH, Lewandrowski KB, et al. Multicenter evaluation of the Roche NT-proBNP assay and comparison to the Biosite Triage BNP assay. Clin Chim Acta 2003;338:107–15. Clerico A, Prontera C, Emdin M, Passino C, Storti S, Poletti R, et al. Analytical performance and diagnostic accuracy of immunometric assays for the measurement of plasma B-type natriuretic peptide (BNP) and N-terminal proBNP. Clin Chem 2005;51:445–7. 19. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999;130:461–70. 20. Levey AS, Greene T, Kusek JW, Beck GJ. A simplified equation to predict glomerular filtration rate from serum creatinine [abstract]. J Am Soc Nephrol 2000;11:A0828. 21. Petersen PH, Sandberg S, Fraser CG, Goldschmidt H. Influence of index of individuality on false positives in repeated sampling from healthy individuals. Clin Chem Lab Med 2001;39:160 –5. 22. Iglesias N, Petersen PH, Ricós C. Power function of the reference change value in relation to cutoff points, reference intervals and index of individuality. Clin Chem Lab Med 2005;43:441– 8. 23. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307–10. 24. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res 1999;8:135– 60. 25. Schou M, Gustafsson F, Nielsen PH, Madsen LH, Kjaer A, Hildebrandt PR. Unexplained week-toweek variation in BNP and NT-proBNP is low in chronic heart failure patients during steady state. Eur J Heart Fail 2007;9:68 –74. 26. Troughton RW, Richards AM. BNP for clinical monitoring of heart failure. Heart Fail Clin 2006; 2:333– 43. 27. Fokkema MR, Herrmann Z, Muskiet FA, Moecks J. Reference change values for brain natriuretic peptides revisited. Clin Chem 2006;52:1602–3. 28. Clerico A, Recchia FA, Passino C, Emdin M. Cardiac endocrine function is an essential component of the homeostatic regulation network: physiological and clinical implications. Am J Physiol Heart Circ Physiol 2006;290:H17–29. 29. Pedersen EB, Pedersen HB, Jensen KT. Pulsatile secretion of atrial natriuretic peptide and brain natriuretic peptide in healthy humans. Clin Sci (Lond) 1999;97:201– 6. Clinical Chemistry 55:5 (2009) 929