Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Update
and Perspectives
Muscle
Aids*
1: The Inspiratory
Part
John
R. Bach,
M.D.,
on Noninvasive
Respiratory
Aids
F.C.C.P.
(Chest
1994;
vival
105:1230-40)
can
terms
B1PAP=bilevel
positive
airway
pressure;
CAH’chromc
alveolar hypoventilation;
CNEP=continuous
negative
extrathoracic pressure;
CPAP=continuous
positive
airway
pressure;
DMD=Duchenne
muscular
dystrophy;
EPAP=expiratory
positive
airway
pressures;
EPR
electrophrenic
respiration;
GPB=glossopharyngeal
breathing;
IAPVintermittent
abdominal
pressure
ventilator,
ffAP
inspiratory
positive
airway
pressures;
IPPBintermittent
positive
pressure
breathing;
IPPVintennittent
positive
pressure ventilation;
MI-E=mechanical
insufflation-exsufflation;
NPBVs=negative
pressure
body ventilators;
PCEF=peak
cough
expiratory
flows;
RTIs=
respiratory
tract
infections;
VCvital
capacity
I nadequacy
of inspiratory
from
primary
cage deformity,
and
muscle
neuromuscular
loss of respiratory
decreased
pulmonary
airway
disease,
some combination
function,
dysfunction,
exchange
compliance,
severe
sleep disordered
of the above,
leads
of life,
without
without
intrinsic
reversible
the excess
paralytic
pulmonary
oxygen,
dilators,
chest
and
oropharyngeal
obstructive
or
The
is usufor in-
or significant
use
of supplemental
problems
and effectively
of
reducing
clearing
the workload
of
airway
secretions.
The risk of pulmonary
morbidity
and mortality
from
acute
respiratory
failure
correlates
with
increasing
hypercapnia.8’9
When
atelectasis
is reversed’0
and
ventilation
normalized
by the
use of noninvasive
inspiratory
risk
5From
muscle
of pulmonary
the
Reprint
Newark,
1230
Hospital,
Institute
requests:
NJ
07103
blood
gases
complications
Department
University
and Kessler
aids,
of Physical
improve,4118
decreases,
Medicine
UMD-New
Jersey
Medical
for Rehabilitation,
West
Dr. Bach, UMDNJ,
191 South
the
and
sur-
and Rehabilitation,
School,
Orange,
Newark
NJ.
Orange
Avenue,
transient
also
peak
play
in
quality
savings
for
lung disease.
and mortality
muscle
weakness
a major
of patients
as well
patients
cough
role
in
with
as for
pulmonary
disease.19
The use of
mechanical
expiratory
muscle
in Part 2.
muscle
lar patients
trachecstomy
muscle
aids are
for patients
with
function
for
who switched
from
generally
preferred
switched
from
of noninvasive
preferred
sufficient
effective
speech
preferred
back.2’
from
including
the
overwhelmingly
use
the former
and generally
wished
to switch
In the same study the 59 patients
who switched
tracheostomy
IPPV
to up to 24-h
preferred
the
comfort,
appearance,
breathing
givers
yielded
similar
noninvasive
IPPV
latter
for speech,
sleep,
security,
use of glos-
(GPB),
ferred
it overall,
thus confirming
quality
of life benefits
in using
ods rather
than tracheostomy.
care
body ventilator
use to
the latter,
while those
a noninvasive
regimen
IPPV
to tracheostomy
sopharyngeal
breathing
(IPPB)
which
is often
used
periods
and at adequate
pressures
to
inspiratory
muscles
do not address
the
can
benefit
and swallowing.
Use of both inspiratory
and expiratory muscle
aids may be necessary
to avoid
pulmonary
complications,
intubation
and
tracheostomy,
and prolong
survival.’”#{176}
In one study, neuromuscu-
overwhelmingly
swallowing,
physical
therapy,
inhalants
and bronchomedications
delivered
by intermittent
positive
pressure
for inadequate
support
or rest
fundamental
breathing
disease.
morbidity
expiratory
those
with primary
manual
and especially
aids will be discussed
thoracic
membrane
greatest
function,
cost
adequate
(PCEF)
Noninvasive
respiratory
by and are most effective
breathing
to atelectasis,13
bronchospasm
to generate
flows
the
potential
concomitant
significant
Inability
increased
work for inspiratory
and expiratory
muscles,
and eventually
to chronic
alveolar
hypoventilation
(CAH).4
Hypercapnia
results from the resort
to shallow
breathing
to avoid overloading
inspiratory
muscles5
and
can in itself
decrease
respiratory
muscle
strength.6’7
dividuals
with
in respiratory
and
survival,
expiratory
whether
Current
preintubation
respiratory
management
ally limited
to interventions
of unproven
efficacy
be prolonged,4”
of improvement
and
unanimously
pre-
the patients’
perceived
noninvasive
IPPV methA survey
of the patients’
results.
Another
study
dem-
onstrated
200 percent
cost savings
by using noninvasive
ventilatory
support
methods
for patients
with no ventilator-free
time
by facilitating
community
placement
with 24-h personal
care attendants
rather
than nursing
care or long-term
institutionalization.2’
benefits
of noninvasive
interventions,
to be used
in few
centers,
iar with all of the techniques
ties in invasive
endotracheal
ingly
appreciated
account,
interest
can
only
Noninvaswe
and
few
clinicians
available.
approaches
and patient
in exploring
Despite
the
aids continue
such
preferences
noninvasive
are
famil-
As the difficulbecome
increastaken
into
alternatives
increase.
Respiratoly
Muscle
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
Aids: The
Inspiratory
Aids (John
R. Bad7)
WHAT
ARE
N0NINvAsIvE
RESPIRATORY
Although
MUSCLE
The respiratory
or mechanically
applying
mittent
pressure
to the
on the
ventilators
body
include
the negative
(NPBVs)
and oscillators
ratory
muscles
muscles
by
rectly
to the
body
can
be aided
by manually
to the body
or inter-
forces
airway.
The
creating
changes
around
the
lators
and exsufflation
devices
which
act
pressure
which
assist
atmospheric
thorax
and
devices
body
respi-
pressure
displace
which
to the
apply
airway.
Certain
positive
pressure
ventilators
the capacity
to deliver
continuous
pressure
(CPAP).
Likewise,
certain
or blowers
have
positive
airway
negative
pressure
and
alveolar
patency.
They
are
used
the presence
niques
alone
of hypercapnia,
the
is usually
inadequate.
pressure
(IPAP)
and no ventilator-free
time
otherwise,
use GPB successfully
for hours of ventilator-
IPPV,
safety
first
can
recognized
be useful
and
for the
is
(GPB)
described
in the
with
The
early
paralytic
“gulp.”
of 60
training
the
period,
to
of GPB
Glossopharyngeal
capped,
the
gulped
walls
of the
tube
afforded
to eliminate
aids.
ventilator
Body
in
GPB
are
favor
of
AIDS
Ventilators
and
create
subatmospheric
abdomen
to assist
described
by the
Scottish
pressure
is created
in
Co, Cambridge,
Mass)
physi-
pressure
by a piston
the iron lung
(Fig 2) by the
action
of a motorized
bellows.
The iron lung which
was perfected
in 1928,32
was the first body ventilator
1950s,
1600
tongue
and
effort
by
The glottis
be
1200
-
cc
so
0;so
60
41
36
24
12
0
SEC
moni-
1600
tored
by spirometrically
measuring
the milliliters
of
air per gulp, gulps per breath,
and breaths
per minute
(Fig 1). An excellent
training
manual
and video
are
available.’26
The
GPB
can provide
an individual
with
weak
inspiratory
muscles
and little or no measurable
vital
capacity
(VC)
or ventilator-free
time
with
normal
alveolar
ventilation
for hours
and perfect
safety
when
not using
ventilator
increasing
a ventilator
or in the event
failure
day
or night.20’27
Its
PCEF
and on cough
effectiveness
described
in
1956.28
or
effort.3#{176}Tank
ventilators
conor cylinder,
eg, the iron lung,
body
up to the neck.
The first
inspiratory
can
to
the
and pressures
of GPB. The
Dalziel
in 1882.’
The negative
by a pair of bellows
operated
Negative
H. Emerson
out
by effective
MUSCLE
intermittently
the thorax
was
air tends
and
tracheostomy
INSPIRATORY
Pressure
NPBVs
around
cian,
John
was created
One breath
usually
consists
100 ml each.
During
the
efficiency
technique.
useful
in the presence
of an
tube.
It can not be used
as it is during
trachestomy
outer
versatility
Negative
tank
(J.
muscle
failure.
It involves
the use of the
pharyngeal
muscles
to add to an inspiratory
projecting
boluses
of air past the glottis.
closes
with each
of 6 to 9 gulps
when
support
the inspiratory
sist of either
a tank
which
envelopes
the
indirectly,
expiratory
muscle
by GPB.2#{176}This
technique,
patient
and
THE
rod.
and,
assisted
the
key reasons
noninvasive
the resulting
bilevel
positive
airway
pressure
(BiPAP)
assists
inspiratory
muscle
as a function
of the IPAP
EPAP
difference.
inspiratory
can be
even
to facilitate
the air
ventilators,
the
extremely
useful,
GPB
few healthcare
profes-
tracheostomy
site as airway
volumes
increase
during
the air stacking
process
expiratory
airway
pressure
(EPAP),
whether
by pressure
or volume-cycled
Both
activity
and
around
exceed
positive
delivered
Breathing
with
is also rarely
tracheostomy
tube is uncapped
The
pressure
airway
Glossopharyngeal
familiar
use of these
techOnce
inspiratory
positive
et a129
(DMD)
musculature
who could
leak
they
In
weakness
users who were very successful
at GPB. We
four DMD
ventilator
users and many
other
with moderately
involved
oropharyngeal
breathing
indwelling
when the
intermittent
the patient’s
own ventilatory
muscle
function,
but
do not directly
assist respiratory
muscle
activity.
muscle
of GPB,
Baydur
muscular
dystrophy
ventilator
have seen
individuals
sionals
respira-
generators
or ventilators
which
can be used to operate
a chest shell or tank-style
ventilator
can also increase
functional
residual
capacity
by creating
continuous
negative
extrathoracic
pressure
(CNEP).
Both CPAP
and CNEP
act as pneumatic
splints
to help maintain
airway
oropharyngeal
free time. Although
potentially
is rarely
taught
since
there
are
abdomen,
body ventiwhich
apply
force
di-
to mechanically
tory muscles,
and devices
pressure
changes
directly
severe
limit
the
usefulness
reported
two Duchenne
can
AIDs?
of sudden
benefit
on
was first
cc
:#{176}#{176}
6041
35
26.
12
0
SEC
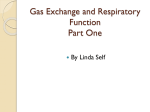
1. Top: maximal
GPB breaths
minute
ventilation
8.39
L/min,
GPB inspirations
average
1.67 L, 20 gulps,
84 mI/gulp
for
each
breath
in a patient
with
a vital
capacity
of 0 ml. Bottom:
same
patient
regular
GPB
minute
ventilation
4.76
L/min,
12.5
breaths,
average
8 gulps
per breath,
47.5 ml/gulp
performed
over
a 1-mm
period
(with
appreciation
to the March
of Dimes
for republication
of this illustration).
FIGURE
CHEST/105/4/APRIL,
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
1994
1231
The
chest
shell
style
ventilators
shell which
covers
the chest
first described
shortly
after
Negative
pressure
is cycled
action
of a negative
child-Huxley
chest
table
Respirator,
became
the first
tors.
They
sitting
can
support
2.
ventilator-free
FIGURE
Patient
with
time
for
lung
use with
mouth
during a respiratory
assist him in mobilizing
cup.
to receive
used
from
use
for both acute
and
1981 until the late
elsewhere,
effective
3) by the
ventilator.
FIGURE
measurable
PortaLung.
and
action
no
iron
and
in
used by
northern
is created
(Lifecare
of
was
the
main
a
Boulder,
Cob).
largely
supplanted
a
many
Italy
in the United
and
possibly
to be the
ventilatory
mainstay
support.’
in the more
portable
Inc. Lafayette,
Cob)
negative
3. Postpoliomyelitis
patient
vital
capacity
since
1955
pressure
with
using
pump
of
tank
(Fig
or
with
chest
Their
shell
by
introduced
chest
shell
shells
use
by the
for
patient
manufac-
for nocturPuritan-Ben-
daytime
more
the
FairPor-
in 1949,
ventila-
the
are
are used predominately
mc, Lafayette,
Cob;
nett,
aid
practical
abdominal
pressure
ventilator
IPPV
methods,
and GPB.36
has
inter-
(IAPV),
non-
The wrap style ventilators,
similar
in principle
and
function
to the chest
shell
ventilator,
are the most
recently
developed
and
now
the most
frequently
prescribed
NPBVs.
The prototype
wrap
ventilator
was
the Tunnicliffe
breathing
in 1955 and continues
wrap
ventilators
consist
covers
body
device
long-term
ventilatory
support
1950s.
Iron lungs continue
to
iron lungs continue
intensive
care
unit
Negative
pressure
style “PortaLung”
and
intermittent
positive-pressure
ventilation
tract infection. The resulting deep
breaths
airway
secretions
and expectorating
into
widespread
be manufactured
States.
In centers
1232
Duchenne
muscular
dystrophy
over
10 years
who is supplementing
the
ventilation
Similar
of a firm
ventilator.
The
and Monaghan
which
were
mass
produced
been
mittent
invasive
under
pressure
respirator34
or supine.
tured
today
and
nal aid (Lifecare
consist
and abdomen.
They were
the Dalziel
apparatus.3132
the
under
thorax
and abdomen.
it are covered
by
which
Negative
is sealed
pressure
pressure
under
time
than
consuming
chest shell
covering
The
jacket
which
was described
to be used in England.3
All
of a firm plastic
grid which
of the
evolution
around
the
ventilators
the
wrap
to don,
ventilators
and
The
grid
a wind-proof
neck
cycle
and
extremities.
subatmospheric
grid.
they can
because
and the
jacket
Although
be more
of more
thorax
and abdomen.
of NPBVs
was summarized
more
effective
complete
by Wool-
lam in 1976.3138
Since
1976, the major
advancements
have been in the material
used in the shells and wraps,
the length
and form
of the wrap
sleeves,
and in the
no
a
Noninvasive
Respiratory
Muscle
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
Aids: The
Inspiratory
Aids (John R. Bach)
negative
pressure
with its caudal
end
pelvis
has
perineal
but
the
care
there
ventilators
sealed
over
advantage
and greater
themselves.30
A wrap
the lower abdomen
or
of easier
patient
lower
extremity
is a tendency
for
the
wrap
access
for
mobility,
to slip
up
and
under
the grid.
This
decreases
comfort
and causes
leak,
especially
at pressures
exceeding-45
cm H20.
Wraps
that extend
down
the legs and are sealed
at the
thighs
or ankles
are easier
to seal, but some patients
complain
of the
sensation
of the
fabric
squeezing
their
legs during
use. A “Pulinobag”
(Lifecare
mc, Lafayette
GO) or “Pneumobag”
(New
Tech,
Palisades
Park, NJ)
is essentially
a full-length
wrap
ventilator
completely
sealing
the lower
extremities.
This decreases
leak and
facilitates
the
donning,
“‘squeezing”
but
of the
be uncomfortable.
permits
the escape
& Associates,
Inc.
the
dorsiflexion
legs that
of the
occurs
feet
during
and
use can
care
Inc. Lafayette,
Gob),
the wrap
is formed
into
arms and pants legs which
separately
seal each extremity, and there is a long anterior
air-tight
zipper
closure.
lower
extremity
mobility
and
stasis in the lower
extremities
for toileting.
“NEV-100”
“Maxivent”
latter
two
negative
(Lifecare
Inc.,
(Puritan-Bennett
ventilators
and
for patients
vasive
IPPV
can
positive
ventilators
Gambridge,
include
Mass)
the
the
Lafayette,
Gob)
and the
Inc., Boulder,
Gob).
The
alternatively
deliver
both
pressure.
This
who depend
on both
methods
at different
is especially
NPBVs
times
useful
and noninduring
the
day.
The
“NEV-100”
and
the
“33-GR”
permit
the
use of
CNEP
which,
like GPAP,
was first described
in the
1870s.3’
A GNEP
provides
the mechanical
effects
of
GPAP,
but does so by decreasing
thoracic
pressure.
A
flow or negative
pressure
sensor
at a nasal
cannula
permits
these
ventilators
to
assist-control
mode
ventilation
thoracic
ventilator’s
Negative
pressure
capture
pressure
provide
the option
of
from
a negative
extra-
baseline.
This
of the patient’s
sensors
also
should
improve
the
breathing
rhythm.
permit
the
patient
use of a NPBV
or rocking
bed with noninvasive
IPPV.
Until now synchronizing
the simultaneous
use of these
modalities
has been problematic.39
This combination
may be particularly
useful
in managing
patients
with
failure,
time
and
low
pres-
and
flow
pat-
terns
and thus the inspiratory/expiratory
ratio,
may
be particularly
useful
for managing
patients
with
respiratory
failure
due to obstructive
lung
disease.
The NEV-100
can also immediately
follow the negative
pressure
with
positive
pressure
to assist
expiration
when
used in conjunction
with a strapped-on
chest
shell
or a PortaLung.
and
pressure
the shell,
Maxivent
and
than
With
sensor
at the
or cylinder,
compensate
for
prevent
adequate
the Maxivent
does
deliver
sighs
blower
of the
negative
GNEP,
alarms,
models,
pressure
hose
into
the NEV-100,
33-GR, and
air leakage
which
might
Al-
an assist/control
operate
does
it
pressures.
have
not
automatically,
or provide
disconnect
the other
its high
insertion
wrap,
current,
on
have
is less expensive
and it has been
12 years.
Another
NPBV
with
similarities
ventilator
but
which
incorporates
direct
low pressure
and
used
simpler
reliably
for
provide
lation
GNEP
around
and high
a negative
or atmospheric
lator (Flexco,
zerland).
This
tive-negative
pressures
ventilator
shell
to
oscillation
ventipositive
pressure,
is the Hayek
AG, Zurich,
provide
alternating
can
negative
and
to assist alveolar
was recognized
to form
or
cm
seal.
oscilSwitposi-
oscillations
with
H20.
The capacity
positive
pressure
under
a
ventilation
and support
in 1939.40
The chest shell
is a light,
soft foam
a tight
chest
shell ventilator
adequate
negative
because
active,
frequency
pressure,
pressure
cycles
+100
to -100
of the Hayek
Oscillator
flexible
cuirass
with
closures
to a chest
the capacity
pressure
baseline
Medical
Instruments
from
of alternating
chest
shell
circulation
molded,
rubber
Besides
clear
and
plastic,
velcro
functioning
at normal
breathing
pressures
(-45
to -60
both inspiratory
and expiratory
the positive
pressure
expiratory
as a
rates
and
cm H20),
cycles
assist
can
may
be
be
useful
in limiting
the tendency
to increased
air trapping for patients
with obstructive
lung disease
using
ventilatory
support.
This device
has been
shown
to
be effective
at frequencies
up
to
increase
the depth
of or prolong
the inspiratory
assist
in a manner
similar
to that of a patient
using
IPPB.
This assist control
feature
facilitates
the simultaneous
ventilatory
failure
during
respiratory
tract
(RTIs)
(Fig 2). A sigh mode
has also been
into the NEV-100.
In addition,
the NEV-
has internal
failure,
power
alarms.
The ability
to vary inspiratory
though
mode,
to nylon
in the fabrication
of the wrap.
Cortex
makes
for a cooler,
more
flexible
wrap
and increases
both
comfort
and expense.
For the ‘“Red Poncho”
(J. H.
Emerson
Go, Gambridge,
Mass),
“Pneumosuit”
(New
Tech
mc, Palisades
Park,
NJ), or “NuMo”
Suit (Life-
The new negative
pressure
“33-GR”
(J. H. Emerson
Go.,
100
sure
otherwise
A wind-impermeable
cloth which
of humidity
(Goretex,
W.G. Gore
Elkton,
Md) is now an alternative
This design
optimizes
may discourage
venous
but it is inconvenient
paralytic
infections
incorporated
in assisting
alveolar
ventilation
approaching
60 Hz.41 It can
to 160 Hz.
The NPBVs
are
support
and
cular/paralytic
can
despite
frequent
the
mogbobin
airway
ness
to the
often
patients
desaturations
collapse.
of NPBVs,
more
suitable
for
adequately
with little
occurrence
due
noninvasive
episodes
of
and decreased
effectivehave had to be switched
IPPV
CHEST/105/4/APRIL,1994
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
ventilatory
ventilate
neuromusor no VG for decades
of transient
oxyhe-
to apparent
With aging
many
patients
effective
overnight
in humans
oscillate
at
methods
up
1233
Body Ventilators
the Body
These
Which
ventibators
IAPV.
support
Apply
include
Pressure
the
rocking
The rocking
bed has been
the ventilation
of patients
cyclically
to
bed
the
and
used since 193236
with poliomyelitis
and muscular
dystrophy.
The rocking
son Go, Gambridge,
Mass) rocks the
15#{176}
to 30#{176}.
Gravity
Directly
to
bed (J H Emerpatient
an arc of
displaces
the
abdominal
contents.
This
causes
diaphragmatic
excursion
and
assists
ventilation.
Although
this device
is adequate
for many
patients
with relatively
normal
pulmonary
compliance,
it is not as effective
as NPBVs.37
It, bike
the iron lung, however,
term basis by many.ss
The IAPV
involves
-
4. Patient
with spinal
cord injury
and no ventilator-f
ree
except by glossopharyngeal
breathing.
He was converted
from
tracheostomy
intermittent positive-pressure
ventilation to daytime
use of an intermittent
abdominal
pressure
ventilator,
pictured
here,
and nocturnal
mouth
intermittent
positive-pressure
ventilation.
FIGuRE
continues
the
to be used
intermittent
on a long-
inflation
of an
air sac or bladder
which
is contained
belt. The sac is inflated
by a positive
in a corset
or
pressure
venti-
lator.
McSweeney
The
prototype,
described
by
in
time
to 24
h a day
when
patient,
NPBVs
assisting
or “resting”
of time.
on the
nocturnal
gases
mum
necessary.’44
have
been
For
described
inspiratory
the
as
muscles
GOPD
useful
for
in
periods
There
have been many
uncontrolled
reports
success
of various
regimens
of daytime
or
NPBV
use in normalizing
arterial
blood
during
autonomous
breathing,
increasing
inspiratory
and expiratory
pressures,”’8
transdiaphragmatic
walking
distance,16
pressure,
respiratory
exercise
vanced
toberance,
and
GOPD
patients.’5
studies
studies
have
were
pliance,
a day),
disaffirmed
marred
by
relatively
and
use
quality
decreasing
Although
of
muscle
maximaximal
life,
12-mm
endurance,
dyspnea
for adthe few controlled
these
positive
difficulties
with
results,
patient
these
com-
short periods
of use (under
4 to 5 h
on few
patients
with
significant
hypercapnia.448
In general,
although
often less effective
than
NPBVs
are
noninvasive
less practical
and
IPPV methods,49
they
can be very
useful
during
tracheostomy
site
closure
when transferring
patients
from endotracheal
IPPV
to noninvasive
support
methods,27’5#{176} and as an
alternative
RTIs. Except
or
supplemental
for the iron
lung
are generally
scoliosis
and/or
not useful
extreme
also
-60
when
negative
as is often
the
shell
patient
common
cm H20
or
wrap
with
tive
apneas
can
be treated
style
significant
associated
method
of aid
and PortaLung,
in the
obesity.
must
using
by concomitant
exceed
a chest
particularly
for
back deformity.
The
with NPBV
use during
patient
to mechanical
oscillation
or tracheostomy
IPPV,
or most
vasive
IPPV.
1234
presence
of severe
Back discomfort
is
pressures
case when
ventilator,
during
NPBVs
CPAP,
at higher
practically,
the
obstrucsleep’42
switching
the
frequencies
to nonin-
1938,’
was
initially
Sweeney
soon
assisted
if the
applied
realized
belt
around
were
the
inspiration
that
placed
chest.
would
around
the
Mc-
be better
abdomen.
The modern
IAPV
(Exsuffiation
Belt, Lifecare
Inc,
Lafayette,
Gob)
consists
of an elastic
inflatable
bladder
incorporated
within
the patient’s
outer
moves
the diaphragm
an abdominal
corset worn beneath
clothing
(Fig 4). Bladder
action
upwards
causing
a forced
exsuf-
fation.
During
bladder
deflation,
the abdominal
contents and diaphragm
fall to the resting
position
and
inspiration
occurs
passively.
A trunk
angle
of 30#{176}
or
more
from the horizontal
is necessary
for its effectiveness. If the patient
has any inspiratory
capacity
or is
capable
of GPB,
he can add
his autonomous
tidal
volume
to the mechanically
assisted
inspiration.
The
IAPV generally
augments
tidal volumes
by about
300
ml,
but
volumes
as
high
as
1,200
ml
have
been
reported.36
Patients
with less than
1 h of ventilatorfree time usually
prefer
to use the IAPV
when
sitting
rather
than use noninvasive
methods
of IPPV.36
The
IAPV
is often
or obesity.
THE
inadequate
EVOLUTION
Trendelenburg
tracheostomy
tube
ventilation
during
The
in the
popularized
the first to describe
with an inflated
cuff
anesthesia
of a human
intubation
support
ventilators
poliomyelitis
Noninvasrve
during
anesthesia
during
World
was
and the
support
War
this and the fact that tracheostomies
for managing
airway
secretions
by body
ventilators
were
not used for
before
made
this
epidemic
Respiratory
the use of a
for assisting
in 1869.52
Tracheostomy
for ventibatory
for anesthesia
patients
ventilated
tracheostomy
tubes
batory
IPPV
was
use of transoral
However,
despite
were often
placed
of scoliosis
TO TRACHEOSTOMY
described
soon afterwards.53
use of a mechanical
bellows
were
presence
Muscle
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
the
a
inadequate
necessity
jM
in
in the
ongoing
1940s,
ventisupply
of body
during
the
1952
in Denmark.
Aids: The Inspiratory
Aids (John
A. Bach)
During
94 percent
the Danish
epidemic,
the mortality
rate
for patients
with respiratory
paralysis
concomitant
those
bulbar
without
involvement
bulbar
and
28
invobvement.
was
and
percent
Three
for
involvement.’6
United
creases
due to more frequent
for those with severe
However,
States
also
in mortality
specialized
centers
reported
equally
by “individualizing”
required
ventilatory
support.
litis mortality
decreased
from
in 1952
for ventilatory
Los Angeles
support.
Although
many
General
Hospital,
particularly
bubbar
ment
polio,
had
of secretions
NPBVs,
in other
performed,
cent.56
tality
without
the
centers
where
mortality
also
few
eliminate
rates.57
A long
were
debate
factors
ensued
ventilators
In 1955,
posium
poor
tomy
decare.
at Los
percent
were
to about
an
defined
in
as to whether
the
indications
mortality
for ventilatory
Gonsensus
Symfor
tracheostomy
as
disturbances.56
If a patient
is going
VC, a tracheotomy
to be left
may
to get rid
of a tracheotomy
and there
is no power
who
has been
tube
treated
In 1958,
Forbes58
efficient
does
not
materially
must
migrate
accessible
sibility
to suction
of
these
bronchoscopy
mechanical
Forbes
access
the
in
it necessary
the
a VC
only
is
first
tracheotomy
the
lower
to provide
survive
of secretions
before
they
tube.
bronchial
indirect
and
patients,
which
become
The
inacces-
tree
even
means
noted
that
the
published
mortality
without
pharyngeal
paralysis,
figures
lower
with
IPPV,
and
respiratory
tracheal
to
for their
expulsion.”
also
dam-
patient
and
alveolar
respirators
mobility.
by
For
pressures,
Tracheostomy,
the
thus,
early
spread,
taught
prog-
noninva-
patients
with
tracheosof food
delivery,
became
the
control
high
were
of
technology
to follow.
standard
of care
in
1960s.
use of endotracheal
manually
in medical,
curricula,
ventilators.
more
over
were
oxygen
ventilation,
and the use of the
and alarm
systems
which
methods
assisted
nursing,
and clinicians
Noninvasive
became
coughing
was
and respiratory
wide-
no
lost familiarity
IPPV
methods,
longer
therapy
with
body
which
are
effective
than
body
ventilators
and preferred
tracheostomy
and body
ventilator
methods,2’
not to be described
until 1969, and their use was
in a significant
support
until the
population
1980s.
Further,
devices
patients
for 24-h
the only
had been for acute
with severe
intrin-
sic pulmonary
disease.57
The former
transient
population,
and the latter
was felt to be a
a population
for
which
the use of noninvasive
respiratory
muscle
aids
was problematic.
Although
MI-E devices
went off the
market
in the mid-1960s,
they continued
to be used
by patients
with access
to them.
More recently,
their
successful
use was
level quadriplegia,
and postpoliomyelitis,
use of noninvasive
With
widespread
to provide
in certain
in six studies
among
acute
patients
were
tank respiration
than
with tracheostomy
that with
tracheostomy
in patients
with
paralysis
a patient
figure.56
is designed
trachea
low
difficult
or 600 cc
500
can
of that
which
and
a very
as we all know,
the bronchi
bronchi
through
with
It is very
to the trachea
in ridding
upper
secretions
makes
from
with
“Tracheotomy,
and
assist
to the
whereas,
devices
wrote,
the VC
when
in a respirator
airway
cripple
disadvantage.
of coughing,
get out of all mechanical
a more
a respiratory
be a great
managed
patients
and
patients
with
severely
muscle
function
could
not effectively
inspiratory
muscle
aids. Tracheostomy
studies
of the use of MI-E
poliomyelitis
patients
and
the combination
of respiratory
insufficiency
with swallowing
insufficiency
and disturbance
in consciousness
or vascular
mechanical
for a worse
and saliva.
Intubation
and tracheostomy
also simplified intensive
care nursing
and equipment
needs.
It
provided
a closed system
for ventilatory
support
which
was amenable
to precise
monitoring
of ventibatory
not reported
ventibatory
tracheostomy
were
preferable
International
to patients
facilitated
As the
2 per-
high faof NPBVs
decreasing
and
made
bulbar
muscle
control,
intubation
or
with cuff inflation
decreased
aspiration
volumes
of bulbar
insufficiency
and aspiration
of
Better
nursing
care and attention
to mansecretions
including
the use of devices
to
them
or body
support.
the
for manageventilated
by
It was concluded
that the previously
rate was not because
of inadequacy
but because
secretions.
aging
airway
for IPPV
tracheostomies
decreased
(MI-E)
routine
methods.58
in
patients
at
those with
placed
were
loss of “the
compression”
by comparison
Uncooperative
affected
bulbar
use noninvasive
use of tracheostomy
tracheostomies
while
they
chest
and
However,
patient
life-styles
were
often
greatly
restricted
by NPBV
use, and elimination
of respiratory
tract secretions
was difficult
for patients
using NPBVs.
General
acute
poliomye12 to 15 percent
in 1948
to 2 percent
of
for GPB,
insufflation-exsufflation
use of
bubbar
significant
patient
From
1948 to 1952, 3,500 patients
were treated
Angeles
General
Hospital.
Fifteen
to 20
application
sive
decreased
from 80 to 41 percent,
or to about
7 percent
for the entire
acute
paralytic
poliomyelitis
population
was in part
particularly
loss of capability
nosis
hundred
forty-five
of 2,300 patients
(15 percent)
had ventilatory
failure
and/or
impaired
swallowing.
Lassenss
reported
that mortality
figures
for ventilator-supported
patients
overall.
This
tracheostomy,
age,
described
neuromuscular
for
populations
use
of
patients
with
high
ventilatory
failure,
ideally
suited
endotracheal
to the
methods,
numerous
reports
appeared
of complications
to tracheostomy
and long-term
tracheostomy
These
included
nosocomial
pneumonia
and
rebated
IPPV.
sudden
death
from
cardiac
arrhythmias,
mucus
plugging,
accidental
disconnections,
and other
causes.
Gramnegative
bacterial
colonization
is ubiquitous
and commonly
associated
with fatal mucus
plugging,
chronic
purubent
bronchitis,
granulation
formation,
and sepsis
from
stomal
infection
or paranasal
sinusitis.
Other
complications
include
tracheomalacia
CHEST/105/4/APRIL,
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
and
tracheal
1994
1235
perforation,
hemorrhage,
occurs
in
tracheoesophageal
changes,
plications
and
8 percent2’
to
tracheal
65
fistula,
stenosis
percent59
painful
which
of
patients,
hemorrhagic
and psychosocial
disturbances.
have
been
summarized
tube
These
comreferenced
and
lation.
Since
been
implanted
lation,
GOPD,
1972,
over
into
and
able success.70
Electrophrenic
800
phrenic
nerve
patients
with
central
high
level
respiration
pacers
quadriplegia
involves
have
hypoventiwith
the
vari-
transmission
elsewhere.Z6O
Another
rarely
described
but relatively
common
complication
of intubation
and possibly
tracheostomy
is the presence
of at least unilateral
vocal
of a radiowave
signal by an antenna
placed
on the skin
to an implanted
receiver.
The signal
is converted
to
electrical
impulses
which
are carried
to electrodes
in
cord
and
contact
delivered
paralysis
airway
airway
and hypopharyngeal
muscle
dysfunction
collapse.
The
resulting
chronic
upper
ohitruction
prevents
the
generation
of adequate
recruitment
unassisted
or assisted
PGEF
through
the upper
airway,
and thus,
prevents
tracheostomy
closure
even
in the
presence
of adequate
autonomous
ventilatory
function.
The presence
of a tracheostomy
tube necessitates
regular
bronchial
suctioning,
tracheostomy
site care,
and tube and tubing
changes.
fication
must
be provided
Swallowing
difficulties
occur
of upward
choring
laryngeal
of the
the neck.
increased
Supplemental
and
attended
as the result
movement
trachea
to the
and
strap
This results
in reduced
laryngeal
penetration
chances
of aspiration.
humidito daily.
of restriction
rotation
muscles
by an-
and
skin
gbottic
closure
thus increasing
Interference
with
of
and
the
relaxation
of
the cricopharyngeal
sphincter,
compression
of the
esophagus,
and changes
in intratracheal
pressure
can
add to the
tracheostomy
can
problem.61’62
In addition,
in many
is considered
an “open
wound.”
prohibit
community
living
without
also
prohibit
patients
with
“open
Tracheal
suctioning
causes
cretions,
may be accompanied
and
is at
airway
mucus
best
effective
part
nias
wounds.”
secretions.
Routine
tracheal
plugs
adherent
between
only
The
effect
stimulation
motion
was
tinued
1948,
when
Sarnoff
adequate
phrenic
Glenn00
nently
Despite
this,
the phrenic
long-term
studies
recorded
were
in EPR
phrenic
were
be obtained
In 1968,
a case in which
they
system
for electrical
phrenic
of
nerves.
which
nerve
The impulses
simulates
the
fibers
to
can be
natural
stimulate
the
diaphragm.
Valid
indications
for EPR are essentially
only high level quadriplegics
and patients
with severe
central
hypoventilation
with intact
phrenic
nerves
and
diaphragm.
Problems,
however,
include
operative
risks,
infection,
and
trauma
to the easily
damaged
phrenic
nerves.
The
inhospital
training
period
is at
least 4 to 6 weeks,
often much
longer,
and
costs
usually
exceed
$300,000.
Unilateral
causes
paradoxical
diaphragmatic
movement
total
initial
pacing
and mi-
croatebectasis.
Tidal
volumes
can
not
be routinely
modified
nor precisely
controlled,
and voice quality
is
poorer
than for patients
using noninvasive
methods
of
support
complemented
by
are also subject
to potential
GPB.
Patients
complications
using
from
EPR
their
tracheostomy.
A tracheostomy
is maintained
in at least
90 percent
of EPR
patients70
because
of the upper
airway
collapse
that occurs
during
sleep on EPR and
because
of common
sudden
operational
failure.7’
This
is particularly
dangerous
because
of the lack of internal
alarms
and the inability
to use GPB effectively.
Neuromuscular
fatigue
can also bead to irreparable
nerve and diaphragm
damage.71’72
In summary,
EPR has few indications
and
sive; extremely
expensive;
suboptimally
ineffective
for over 60 percent
of patients;z
complications
tracheostomy,
associated
with
thus
negating
phrenic
is: inva-
effective
or
and entails
having
an indwelling
the advantage
of in-
creased
portability
with this approach.
New impulse
delivery
methods
may increase
efficacy
and safety.
Electrophrenic
respiration
may
be useful
during
tracheostomy
site closure
for transition
to noninvasive
ventilatory
aids and for daytime
use for patients
using noninvasive
IPPV
overnight.
over
numerous
respiration
discon-
NPBVs
became
available.60
Then,
in
and his associates68
demonstrated
that
ventilation
could
nerve
stimulation.
reported
implantable
in
of pneumo-
of the
first
200 years
ago by Galdani.60
There
reports
of resuscitation
by electrophrenic
(EPR).60’67
bronchus
at least
RESPIRATION
of electrical
on diaphragm
misses
and
the
stem
This
accounts
for the fact that 70 percent
occur
in the left lung fields.M
nerve
superficial
suctioning
the tube
the left main
of the time.
ELECTROPHRENIC
1236
suctioning
and
of employment
irritation,
increases
seby severe
hypoxia,60
in clearing
tracheal
wall and misses
54 percent
to 92 percent
states a
This
prohibitively
expensive
nursing
care
for tracheal
wound
care.
Some schools
and places
with the phrenic
in a manner
by unilateral
Judson
and
used a permastimulation
of
nerve.
They
used EPR on an intermittent
basis for a patient
with primary
hypoventi-
NONINVASIVE
IPPV
Tossach
reported
mouth-to-mouth
insufflation
in
1743.
Noninvasive
IPPV
may
have
been
attempted first with a mechanical
device
by Paracelsus
who
ventilated
the lungs
via the mouth
with
a chimney
bellows
in 1530.
His
technique
was
used
through
the 19th
Positive
pressure
century.74
ventilators
able in the United
postpoliomyebitis
States
in 1956. At that
ventilator
users
with
measurable
Noninvasive
VG refused
Respiratory
Muscle
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
became
the advice
Aids: The
in Europe
widely
of their
Inspiratory Aids
time,
little
availmany
or no
physicians
(John A. Bach)
5. Patient
with
Duchenne
muscular
dystrophy
who has
used 24-h mouth
intermittent
positive-pressure
ventilation
for 9
years, now with less than 5 mm of ventilator-free
time. Mouthpiece
is kept adjacent
to the chin controls
for his motorized
wheelchair.
FIGURE
to undergo
ventilators
learned
tracheostomy
and continued
to use body
up to 24 h a day. Many
of these
patients
how
to receive
between
their
the mouthpiece
clamp
via
a mouthpiece
held
preferred
by either
to have
a metal
lips and teeth.
Others
fixed near the mouth
attached
to
the
controls
which
operate
and puff,
chin control,
mouthpiece
for IPPV
positive
IPPV
pressure
wheelchair
or
fixed
onto
the
the motorized
wheelchair
(sip
etc) (Fig 5). They
used the
as necessary.20
The Monaghan
ventilator
was
placed
on wheels
and
rolled
behind
the wheelchair.
Patients
were thus freed
from
their
body
ventilators
during
daytime
hours.
Dr. Augusta
Alba recognized
that patients
would
occasionally
nap
using
mouthpiece
ing out of their
patients
to use
several
relied
in one
while
sitting
IPPV
without
mouths.75
By
center
had
left
in
their
wheelchairs
the mouthpiece
1964,
a number
their
body
fallof
ventilators
7. Custom
lip seal.
FIGURE
and
with
body
ventilators
for 30 years
plates
and
devised
acrylic
mouthpiece
with
for up to 24-h
orthodontic
ventilatory
to increase
and
efficacy,
with
Thompson
Bennett
in 1972,
sleep
piece
comfort
mouthpiece
with
and
IPPV
could
With
regular
deep
1978,
with
eliminate
use
increasingly
the arrival
be delivered
during
the mouthfalling
out
portable
the option
insufflations
of
the advent
of
Boulder,
Gob)
less insufflation
leakage
around
with little risk of the mouthpiece
of the
mouth
(Fig
6). In
ventilators
became
available
ducing
and
bite
were
bong-term
became
with
Bantam
in 1968.
lipseal
(Puritan-Bennett,
plate
support
or more
(Fig 6).4.hl.13
Orthodontic
custom
fabricated
shells
(Fig
7)
the risk of orthodontic
deformity
(Fig 8).
Positive
pressure
ventilators
portable
in the 1960s,
especially
the
the
bite
(sighs)
volume
of proand
with
up to 24-h mouthpiece
IPPV.”20’76
Ultimately,
hundred
patients
have been described
who have
on this
technique
alone
or in combination
FIGURE
6. Patient
with
no measurable
vital capacity
using nocturnal
mouth
intermittent
positive-pressure
with
a lipseal
(Puritan-Bennett,
Boulder,
Cob).
since 1955
ventilation
FIGURE
intermittent
8. Orthodontic
positive
deformity
caused
pressure
ventilation
by 15 years of 24-h
without
a custom
mouth
bite
plate.
CHEST/105/4/APRIL,
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
1994
1237
Nasal
IPPV
can
be delivered
by portable
cycled
or pressure-cycled
ventilators
recently
released
BiPAP
S/TD
machine
Murrysvilbe,
Pa). The latter
is essentially
limited
blower
delivered
is only
without
up
to a pressure
and
FIGURE
9. Patient
with
to kyphoscoliosis
who
interface for nocturnal
lation.0
safety
alarms
and
other
on
IPPV
via
patients
volume
alarm,
care
severe chronic
alveolar
hypoventilation
uses a low
profile
custom
acrylic
nasal intermittent
positive
pressure
unit
which
features.
systems
nervous
which
system
tion leakage
the patient’s
add
rely
reflexes
during
adaptation
considerable
“resting”
the
inspiratory
support
for
100 ml and
GPAP
and
cost
central
insuffla-
can hamper
Alarms
also
to the
and
for
oximethese
monitoring
effi-
muscles
United
delivering
available
design
of
applies
muscular
IPPV
via
positioned
into the nostrils.
first used for 24-h ventilatory
patient
time.79
became
commercially
and were
first used
nasal
CPAP
French
delivered
with a VG of
In 1984,
nasal
available
as interfaces
in the
for
styles
Nasal
age into
of these
the eyes
generic
1238
nasal
IPPV
a mouthpiece
is indicated
because
or
inadequate
jaw
neck
movement
with
opening
or
to grab
severe
Although
lip and
initially,
as an alternative
for
since
effective
by either
nasal
mouthpiece
plugged
oral-nasal
by
Strapless
tion have
oral-nasal
interfaces
been
used in Europe
described
pledgets
have
in
the
and
not
are common
models.
Such
complaints
difficulties
with several
resulted
in
in New
Jersey
(Fig
9)60
unable
ACKNOWLEDCMENT:
Dr.
Augusta
Alba
medical
Mr.
provided
is
be a
some
muscle
was used
patients
with
diseases
with
for long-term
used
mouth
or nasal
interfaces
support
IPPV,
the nose
IPPV
with
tape,
been
strap
retained
widely
used.
with
bite-plate
since
1985
literature
to independently
are
for
ventilatory
or mouthpiece
who
contact
leak-
there
even
lung
to expel
important
on alternate
nights
to vary skin
bridge
pressure
and insufflation
when
Oral-nasal
interfaces
were described
supported
ventilation
in 1989.60 These
strap
retention
systems
like those
for
cotton
interfaces
to use
use,4’36
use.
nevertheless,
other
thrust
is adequate
retention
is also
paranasal
and
little
a mouthpiece.2#{176}
to intubation
pressure
to the
acute
patients
with
neuromuscular
it is now being
increasingly
cystic
fibrosis,
COPD,
and
ventilatory
insufficiency.84’85
IPPV.
However,
could be provided
or when
necessary,
It
flows
with
oropharyngeal
nasal
IPPV
not only provide
delivery
of IPPV,
differently
to adjust
patients
nasal IPPV
can,
to tracheostomy
almost
exclusively
for
ventilatory
insufficiency,
first
with
for those
who can
of oral muscle
weak-
These
interfaces
tight seal for the
the
preparation
of custom-molded
nasal
interfaces.4’79’8
Custom-molded
nasal interfaces
can now
be obtained
both
commercially
(SEFAM
Company,
distributed
by Lifecare
Inc,
Lafayette,
Cob)
and
individually
for
IPPV.00’8’
There
are now commercially
masks
from
several
companies.
Each
area.
It is impossible
to predict
which
model
will be
preferred
by any particular
patient.
Many
patients
use
different
pressure.
capacity
direct
current.
in providing
support
insufficient
used
ventilators.
alarms
of pulse
for introducing
a multiple
sclerosis
no ventilator-free
masks
States
Daytime
not retain
patients
weakness.4
part
excessive
the
Since
patients
generally
prefer
IPPV
or the IAPV
for daytime
is most practical
only for nocturnal
on
large
DeLaubier’8
urinary
drainage
catheters
In 1984, nasal IPPV
was
or no VC.
mouthpiece
nasal
IPPV
in
prevent
have
ventilatory
Twenty-four-hour
viable
alternative
biofeedback,
patients,
do not
and nasal
are usually
cacy of noninvasive
aids including
IPPV during
sleep.77
In 1982, as an alternative
to mouthpiece
IPPV
for
dystrophy
devices
long-term
ness
it very
1120
pharynx
causes
patients
of the high initial
inspiravolume-cycled
ventilators,
they
do not operate
off
Nasal IPPV can be effective
of mouthpiece
and nasal IPPV
saturation
useful
alarms
for
all intensive
makes
sleep.4
The alarms
to these methods.
weight
The oxyhemoglobin
try are the most
techniques,
to
for
expiratory
into
ventibators,
use
useful
the
is incorporated
volume-cycled
difficult
to introduce
the
IPPV.
Further,
mouthpiece
open
Although
tracheostomy,
due
nasal
venti-
of 15 cm
volumes
plateauing
at greater
pressures.
5.42 kg (12 lb) and is useful
for air delivery
high and low pressure
alarms.
On occasion,
airflow
against
the posterior
to gag. This occurs
because
tory cycle flow rates. Unlike
these
volume-
including
the
(Respironics,
a pressure-
but
in
retenwere
1989.86
an essentially
air
but simple
tongue
them.87
The
bite-plate
for patients
living
alone
don
C McPherson
Figure
straps.’3
provided
Figure
7 and
8.
REFERENCES
1 Bergofsky
EH.
Cor
hypoventilation.
2 O’Donohue
pulmonale
Prog
WJ.
of pulmonary
Maximum
atelectasis.
3 Estenne
M, De Troyer
wall statistics.
Am Rev
Noninvasive
Respiratory
Muscle
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
in
Cardiovasc
volume
Chest
the
Dis
syndrome
1967;
IPPB
1979;
The
alveolar
for
the management
76:683-87
A. The effects
of tetraplegia
Respir
Dis 1986; 134:121-24
Aids:
of
9:414-37
Inspiratory
on chest
Aids (John A. Bach)
4 Bach
JR,
lation
by
5 Begin
Alba
AS. Management
nasal
P, Crassino
hypercapnia
Respir
DF,
7 Stubbing
1985;
DC,
mechanics
Dis
1973;
56:297-306
HK
JLC,
disease.
NL.
with
chronic
1952;
JR,
Bach
JR.
positive
Pulmonary
LB,
Beabe
Apgar
correction
J,
airflow
29
1993;
Arch
NMT,
Marino
respiratory
Chest
15 Cropp
1984; 85:595-605
A, Dimarco
AF.
ventilation
obstructive
1987;
M,
F. Alternative
methods
MM,
J,
J
Am
lungs.
ventilation
improves
in patients
with
Respir
in patients
with
Am
Respir
Rev
Dis
blood
sure
and
34
severe
36
Dis
L, Rampulla
pressure
in
cuirass
muscle
strength
hypercarbia.
38
by
muscle
as-
Chest 1990; 98:857-65
A, Corini
M, Schiavina
function
with
39
pneumowrap:
with negative
COPD.
severe
pres-
Chest
1990;
40
RJ,
collapse
J,
Mead
Knudson
to supramaximal
Bach
Alba
JR,
AS,
Glossopharyngeal
agement
1987;
21
DE.
expiratory
Contribution
J
flows.
of airway
Physiol
AppI
1974;
41
of post-polio
JR.
natives
22
and
Bach
JR,
Bach
JR.
patients:
Dail
F, Alba
CW,
Angeles:
Evangelists,
analysis
in-home
FJ,
Schultheiss
aids
insufficiency.
M.
in the
Birth
J
ventilatory
of the patient
man-
42
Defects
support
and care
Am
Ventilator
Affeldt
1954
I. The
Chest
K. Electrophrenic
Paraplegia
use
an update.
Department
AS, Holland
alter-
giver.
C, Del
Arch
JE.
by
Phys
muscular
Med
versus
1992;
48
173-97
for
(1) 1882-1918.
The
evolution
type.
intermittent
Anaesthesia
of iron
Cambridge,
C, Fabbri
failure
diseases:
Mechanical
Ventilation,
prise
Rhone
Alpes
The
Council
with
1976;
respirators
JH
Emerson
in
a series
lung
[abstract
Conference
March
3-5,
cuirass
1993.
JR, Alba
Medicine.
AS. Total
JMK,
Spalding
Opiel
Woollam
CHM.
The
negative
pressure
808
cases
11]. In: Book
on Home
France:
Acceptability
Enter-
support
Chest
274:613-
development
respiration
Portable
by the intermittent
with
the Tunnidliffe
15
of apparatus
(2)
Fair-
143:1157
1991; 99:630-36
respiration
1958;
of the
1950;
The Monaghan
1949; 139:1273
ventilatory
L. Artificial
Lancet
Lyon,
JAMA
ventilator.
jacket.
of
and
1998
respirator.
pressure
of
pulmonary
results
International,
on Physical
M. Treatment
chronic
with
iron
International
The Council
on Physical
Medicine.
Respirator
acceptance
report.
JAMA
Bach
lungs:
Ma:
M, Schiavina
in patients
ventilated
of the 4th
Goldberg
Pfrommer
for
1919-1976.
AL,
M.
Cane
RD,
Childress
D,
Combined
nasal intermittent
ventilation
and
rocking
nocturnal
ventilatory
intermittent
Anaesthesia
1976;
Eisenmenger
MR,
in
oscillator.
Chest
Bach
1992;
breathing
College
a different
45
association
73:179-83
[video].
respiratory
a disabled
Blair
KE,
respiratory
insufficiency:
at
person
Bach
Alba
Bach
home.
respiratory
JR. Inappropriate
with
Saporito
wall
the
Hayek
3/9/93
negative
paralytic!
99:1386-98
L,
Lee
M.
Mouth
in the management
and late
traumatic
81:807-
Chest
chronic
1991;
1987;
Chest
weaning
with
LR.
Rejected
ventilation
insufficiency.
its action
1939;
complicating
Chest
C,
pressure
belly:
utilizing
apnea
in patients
Bohatiuk
AS,
Kline
publication)
sleep
dysfunction.
positive
individuals
PC,
for
support
ventilatory
the
failure
Obstructive
ventilatory
restrictive
over
Wochenschr
Med
Fiehler
(submitted
J.
pressure
Wein
acute
JR, Penek
JR,
and
[Cermanj
oscillation
Ambrosino
N,
Rampulla
dystrophy
of
H. Suction
12
Bennett
of
in chronic
onset
quadriplegia.
of
91:859-64
ventilatory
failure
Paraplegia
1993;
31:430-38
14:9-17
Rehabil
Education,
44
rehabili-
bed
support
Y, Vesely
LC,
positive-pressure
Wu
1991; 99:627-29
intermittent
101:26-30
ventilation:
Soc 1991;
Cbossopharyngeal
of Visual
JA.
Bufabo
respiratory
pressure
Chest
ventilator-assisted
of institutionalization
management.
O’Connor
sup-
homecare.
1978
post-polio
cost
perspective.
25
Curran
non-invasive
of long-term
the perspective
(in press)
BachJR,
lntintola
tation
24
E,
and
respiratory
A comparison
from
individual:
23
Bodofsky
breathing
23:99-113
Bach
Loynes
and application
36:653-67
20
Gunella
Chest
97:322-27
19 Knudson
Intensive
of apparatus
respiration
Chest
of ventilatory
eds.
1992;
development
body-encasing
breathing
Am
C. Diaphragmatic
ventilation
patients
Askanazi
assisted
dystrophy.
31:666-86
and COPD
patients.
F, Duranti
H, Spineili
ventilation
JH,
the
abdominal
138:617-23
in ventilatory
Med
A. Decline
long-term
muscular
& Wilkins,
The
child-Huxley
Weekly
inspiratory
limitation
N, Zocchi
sessment
in normal
18 Scano C, Gigliotti
Changes
gases and
air-flow
1988;
negative
rest during
C, et al.
T, Contreras
chronic
5, Ambrosino
17 Nava
M.
on
pressure
disease.
Emerson
mechanically
of Abstracts
for
function
pressure
acute
limitation.
negative
negative
Company,
1990;
rest
airflow
CHM.
thoracopulmonary
interfaces
Duchenne’s
Williams
Woollam
of
dystrophy.
intermittent
in the
J
N Engl
31:537-47
of
Rehabil
in advanced
Baltimore:
37
Beroiza
with
Beltrame
Med
mechanism
M, Fischer
experience
Rothkopf
185:1056-61
16 Gutierrez
W, Carlson
and
In:
muscular
chronic
I, Prentice
function
JR,
35
muscle
A, Cilgoff
port.
33
of intermittent
pulmonary
Baydur
Bach
oral-nasal
with
Effects
on respiratory
chronic
Rev
in patients
coughing
70:18-20
JL. Glossopha-
in a respirator.
in
AS. Management
Effect of daily
WD.
muscles
to the
poliomyelitis
function
of disease.
1991;
NS, Wilson
97:884-89
in animal
Phys
Talner
as an aid
chronic
Association
of the traumatic
Rehabil
1990;
71:908-11
14 Braun
breathing
DC,
Med
Rev
positive
pressure
to tracheostomy
for
in Duchenne
Strapless
Dickinson
with
J Phys
Am
Am
103:174-82
I.
CI,
Staff
in the rehabilitation
quadriplegic.
Feigelson
Gbossopharyngeal
1979
disease.
CJ. Pressure-time
Beck
H, Alba
ventilation.
approaches
Inc,
ventilation
10:177-82
McDermott
pressure
level
Hospital
HV.
Professional
1956; 254:611-18
32
failure
1987;
JR. New
high
Adkins
Calif:
TR.
of atelectasis
Krotenberg
Los Amigos
Bach
V,
Snow
to stage
V,
Guess
Downey,
AR,
PJ Jr. Pulmonary
related
M,
manuaL
ryngeal
81
respiratory
Nerve
Rev
10:593-602
O’Brien
end stage
Am
28
80
dystrophy
safe
Rodgers
in respiratory
pulmonary
Vignos
ventilator users. Chest
Muscle
27
49:511-15
Bach JR, Alba AS, Saporito
LR. Intermittent
ventilation
via the mouth
as an alternative
Bach
Rev
inspira-
Jones
subjects
Jr, North
AM,
in the
Pediatrics
13
in
1980;
Goodfellow
relations
Morse
Physiol
FC,
muscular
1974;
C,
of Rancho
108:1373-83
Duchenne
Dail
patient
obstructive
Med
257
Am
of maximal
pulmonary
exercise
Appi
in chronic
R,
and chronic
disease.
Determinants
LD,
SR, Oldenburg
10 Day
12
Pengelly
J
Prognosis
Respir
26
breathing
dysfunction
pulmonary
obstructive
SF, Thompson
9 Inkley
hypoventi-
97:52-7
132:42-7
during
obstruction.
11
NMT.
in chronic
Dis
8 Boushy
muscle
obstructive
Braun
pressure
Respir
alveolar
1990;
1991; 143:905-12
6 Rochester
tory
Chest
A. Inspiratory
in chronic
Dis
of chronic
ventilation.
improvement
Eur
Los
of Medical
pressure
disease.
T,
SH,
1989;
Ernst
A,
Brega
ventilation
tolerance
of COPD
S, Fracchia
C,
induces
long
term
patients
[abstract].
2:363s
P, Cray-Donald
ventilation
Lancet
Negri
pressure
of exercise
J
Respir
46 Shapiro
Montagni
C. Negative
in severe
1992;
K, et al. Effect
chronic
obstructive
pulmonary
340:1425-29
CHEST/105/4/APRIL,
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
of negative
1994
1239
47
Zibrak
JD,
Hill
Evaluation
tion
in
patients
Celli
B, Lee
negative
H,
MJ,
Am
muscles
Bach
JR, Alba
ratory
52
Respir
Kuei
1990;
high
CJ. The
of external
severe
1989;
71
chronic
the
of
Chest
pulsator
support
1990;
98:613- 19
in treatment
of
W.
Clinical
tubes
BMJ
74
respi-
HCA.
1952.
H Soc Med
Proc
of poliomyelitis
1954;
Poliomyelitis
pincott,
1955;
Barach
AL,
J
Forbes
59
chanical
Pingleton
Rev
63
Sci
Respir
JB Lip-
Smith
RH.
Mechanical
the capacity
production
of human
coughing.
paralysis
using
79
JA. Evaluation
and treatment
College-Hill
Press
Bonanno
P. Swallowing
Surg 1971; 174:29-33
non-invasive
Annual
techniques
Atlanta,
Association.
Fishburn
in acute
spinal
LH
cord
blood
with
injury.
Johnson
Arch
disorders.
tracheostomy.
Abstracts
Cord
Med
83
Rehabil
LMA.
Cited
to non-cardiac
by Schecter
disorders.
DC. Application
Bull NY Acad
of electroMed
1970;
46:932-51
66
67
Phelps
stimulation
of the
Duchenne
C. Cited
RH,
Smythe
ventilatory
J
HS,
Sci
69
Judson
JP, Clenn
ration:
long-term
Am
with
pacing
Neurosurg
by Vanderlinden
RC,
LD.
electrical
by electrical
198,5;
Epstein
17:974-84
SW,
Management
Hyland
86
of chronic
diaphragm
pacing.
J
Physiol
WWL.
application
E, Whittenberger
1948;
JL.
to a patient
87
electrophrenic
with
primary
respihypoven-
Noninvasive
Duchenne
respiratory
1992;
3:239-69
respiratoire
chronique
Memoires
et
de
certificat
readaptation
1984:
fonction-
1-124
A. Intermittent
nasal
access
in
Chest
1987;
the
positive
management
of
92:168-70
CE. Treatment
with neuromuscular
through
a nose mask.
of
Am
135:148-52
SK. Nocturnal
positive
pressure
Rev Respir
Dis 1987; 135:738-40
lung
JR. Parker
or chest-wall
C, Sortor
positive
disease.
Respir
S. Custom-fabricated
pressure
1992;
failure. Chest
Girault
ventilation
in
C, Faure
acute
ventilation.
J
Int
Spatfolgen
nach
Nocturnal
hypercap-
102:846-50
C, Portier
respiratory
patients.
Chest
1992;
A. Uberdruckbeatmung
102:912-17
durch
Poliomyelitis:
F, Muir
failure:
JF.
Mundstuck.
Chronische
Nasal
experience
In:
in
Frehse
Unterbeat-
Lebensfuhrung
Pfennigparade
eV,
149
Viroslav
ventilation
1991;
for
by
R, Delaubier
intermittent
D,
elderly
Ratzka
1989;
life
Med
mung
und
Moglichkeiten
selbstbestimmter
Schwerbehinderter.
Munchen,
Germany:
Electrophrenic
155:1-9
Radiofrequency
1971; 200-13
of
In:
17th
1969.
AJ, ParkerS,
Torzillo
PJ, Sullivan
CE, Bye FTP.
IPPV stabilizes
patients
with cystic fibrosis
and
U, ed.
Can
of the
Conference,
1989; 2:224-33
Benhamou
mask
15:63-7
SJ, Hardenbergh
respiration.
nerve.
Vanderlinden
1988;
Sarnoff
Diaphragmatic
phrenic
insufficiency
Neuro
68
1240
ML.
York:
J, Gerard M, Robert D. Home
positive
via nasal mask for patients
with neuromus-
I, Bach
for
nic respiratory
85
WWL,
Glenn
nasal
Injury
Rehabil
or restrictive
McDermott
Piper
New
34:73-9
Prosthodont
84
Caldani
therapy
weakness
The
dystro-
of respiratory
considerations
ventilation
1987;
ed.
muscular
0-436-398,
Mayer
LS, Pingleton
via nasal mask. Am
1989;
interfaces
71:197-
1990-.
positive-pressure
Care
of
noninvasive
AH,
diseases.
Bye PTP, Bruderer
JW, Sullivan
failure
during
sleep in patients
Dis
of
Proceedings
Cord
H Descarte,
via
Leger F, Jennequin
pressure
ventilation
and pneumonia
In:
reeducation
insufficiency.
cular
Academy
Management
musculaires.
ventilation
use
other
de linsufflsance
A, Mosher
82
14th
resuscitation
the
prolongation
Phys
de
Kerby
CR,
ventilation
In jury
102
JF. Atelectasis
Rev
81
by
Digest:
Spinal
1988;
of high
insufficiency
FS.
Office
Universite
Respir
resuscitation
National
aspects;
lesions.
the
superieures
Ellis ER,
respiratory
modern
Kutscher
and
Spinal
dystrophies
disease,
Ann
gas monitoring
In:
80
on
rehabilitation
Crit
Paris:
of
medical
cord
A. Traitement
JF, Alba
Rev
respiratory
Phys
in
200
65
aids.
Bach
ed.
(in press)
Printing
nelles.
5th
108
In:
Trainor
dystrophy:
pressure
119
of the American
RJ, Ditunno
MJ, Marmno
1983;
[abstract].
Meeting
complications
after
M. Sleep
patients
Scientffic
Am
39:596-600
of swallowing
Inc.
dysfunction
5, Sipski
quadriplegic
failure.
M,
JR. Pulmonary
les
by distending
observations.
DC:
sclerosis,
Administration
respiratory
Stauffer S. Respiratory
J Neurosurg
1973;
FW,
Logemann
JR, Sortor
a “me-
and
in spinal
Delaubier
1771;
Sittipong
1979; 54:662-68
recovered
and
perspective
lateral
A, Solomon
dans
37:1463-93
quadriplegia.
Diego:
78
Proc
evolution
of Thanatobogy
d’etudes
of respiratory
1988;
H, Pitts
of
Clin
alternatives.
amyotrophic
muscular
226:241-48
traumatic
Bach
Philadelphia:
Bach
Mayo
30:118-22
HM,
7-32
US Covernment
77
1980;
Marsh
Washington,
psychosocial
Veteran’s
Surg
Neuro-
implantable
AS, ed. Cardiopulmonary
A historical
insufficiency
RD.
using
DR.
Baffour,
ventilatory
11:2121-27
Hamilton
Thorac
essays
and
support
muscle
CJ,
1953;
Dis
Alba
J
&
proceedings.
JR.
D,
in appearance
History
1966;
1988;
Gracey
Medical
In: Cordon
Foundation
in Copenhagen,
cough’
respirator. BMJ
1958; 1:798-802
SK. Complications
of acute
respiratory
cervical
64
R Soc
47:67-71
Conference.
JA. Management
Bellamy
San
62
Proc
91-113
Beck
Med
58
61
AS.
phy,
anesthesia.
Hodes HL. Treatment
of respiratory
difficulty
in poliomyelitis.
In: Poliomyelitis:
papers
and discussions
presented
at the Third
Am
Gordon
ventilator:
tracheotomy
dead
In:
T Cadell
ventilatory
of
2:122-24
expiratory flow rates surpassing
60
introduction
of performing
of endotracheal
epidemic
Man
Fundamental
for chronic
experience
Ann
DC,
respiration.
London:
Sciences,
76
The
International
57
1880;
the
Halverson
a 5-year
stimulators.
air.
conference
an den Luft1871; 12: 121-
22:83-8
1928;
Lassen
on
instead
1W. Development
Magill
Med
56
observations
by the mouth
or laryngotomy.
55
W.
with
B, et al.
study. FACE
CB,
JC, Piepgras
Tossach
Dentz
of the diaphragm
failure:
nerve
McMichan
75 Bach
MacEwen
Wilmot
techniques.
Trendelenburg
F. Beitrage
zur den Operationen
wagen 2: Tamponnade
der Trachea.
Arch Kiln Chir
tracheal
54
DD,
lungs
1:1206-07
1938;
RT,
in pacing
H. Electrophrenic
respi-
233
53
72
73
quadriplegic.
203:1033-37
Brouillette
respiratory
phrenic
R. Efficacy
ventilatory
Oakes
genic
140:1251-56
in unloading
for
1968;
insufficiency: a multicenter
Shadmehr
options
Bragg-Paul
BMJ
paralysia
Dis
JH,
JAMA
WWL,
considerations
98:850-56
level
tilation.
70 Glenn
pulmonary
with
ventilation
pressure
Chest
McSweeney
Rev
C.
ventila-
trial
in patients
CW,
O’Donnell
138:1515-18
et al. Controlled
AS. Noninvasive
of the traumatic
51
C,
SL,
obstructive
1988;
ventilation
Son Hon
ratory
Kwa
negative-pressure
chronic
Dis
Criner
positive vs negative
50
severe
obstruction.
Belman
EC,
long-term
Respir
pressure
airflow
49
Federman
with
Rev
disease. Am
48
NS,
of intermittent
J,
Sortor
S, Rosenblatt
in high level SCI
H. Alternatives
to tracheostomy
[abstract].
J Am Paraplegia
Soc
14:87
Respiratory
Muscle
Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21693/ on 06/19/2017
Aids: The
Inspiratory
Aids
(John
A. Bach)