Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
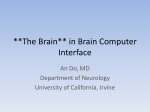
CASE REPORT ISSN 1738-5520 ⓒ 2007, The Korean Society of Circulation Korean Circulation J 2007;37:449-452 Brain Tumor is a Rare Cause of both Bradycardia and Seizure Ki-Hoon Park, MD, Sung-Ho Her, MD, Jong-Min Lee, MD, Hee-Jeoung Yoon, MD, Jung-Yeon Chin, MD, Jun-Han Jeon, MD, Ye-Lee Park, MD, Kyong-Rock Do, MD, Yun-Hwa Jung, MD and Seung-Won Jin, MD Division of Cardiology, College of Medicine The Catholic University of Korea, Daejeon, Korea ABSTRACT The association between brain tumors and cardiac asystole has rarely been reported in the medical literature. This potentially life-threatening symptom has usually been observed to arise from left temporal lobe brain tumors. Yet previously published papers have shown that cardiac asystole and bradycardia, as manifestations of epilepsy, originate from the frontal lobe of the brain. Although syncope is a common presenting symptom of a brain tumor, bradycardia and complete atrioventricular (AV) block, as the first signs of a brain tumor, have been only sporadically documented in the literature. We report here on a patient with recurrent complete AV blocks that were followed by syncope as an expression of seizures that may have arose from a brain tumor; this tumor was most likely a meningioma in the right frontal lobe. The patient required the subsequent placement of a permanent pacemaker. In conclusion, cardiac asystole may be a potentially life-threatening symptom of frontal lobe lesion of the brain. The frontal lobe may play a role in the autonomic regulation of cardiovascular responses. (Korean Circulation J 2007;37:449-452) KEY WORDS:Brain tumor;Heart block;Seizures. Introduction sient complete AV blocks that were followed by syncope as an expression of seizures, and these seizures may have arose from a brain tumor in the right frontal lobe. A patient with a brain tumor can present with a diversity of symptoms or signs, including seizures, headache, nausea, vomiting, focal neurological deficit and an altered mental function.1) It is often difficult to differentiate between the cardiac and neurological etiologies of syncope. To complicate matters, primary cardiac abnormalities can cause secondary neurological signs and vice versa. The causes of syncope range from benign to lethal conditions. The distribution of the causes of syncope in the population of the Framingham heart study(7814 participants) was cardiac causes 9.7%, seizure disorders 5.0%, vasovagal causes 21.2%, orthostatic causes 9.3%, medication 6.7%, unknown causes 36.3% and other causes 11.8%.2) Bradycardia and cardiac asystole sometimes lead to life-threatening syncope for which implanting a demand pacemaker may be useful.3-6) We report here on a patient with recurrent and tran- Case A 78-year-old right-handed man, who was without any relevant medical history and he was not taking any medication except aspirin, was admitted to the emergency room of our hospital with loss of consciousness. He’d had brief paroxysmal episodes that were characterized by behavioral arrest with loss of consciousness during eating breakfast. On arrival at the hospital, the patient had an alert mentality, a blood pressure of 170/100 mmHg and a regular pulse rate of 71 bpm. The cardiovascular and pulmonary examinations did not reveal any abnormalities. Further neurological examination revealed no abnormality of the cranial nerves. The initial electrocardiography (ECG) showed a normal sinus rhythm and no prolonged QT interval(0.414 second). A chest X-ray demonstrated no abnormality. Blood analysis showed no abnormalities, including the electrolytes and the CK-MB and Troponin -T levels. The thyroid function tests were also within normal limits. Contrast computed tomography(CT) of the brain showed a 1.4×2.0 cm sized brain mass in the right Received:May 23, 2007 Revision Received:June 22, 2007 Accepted:July 4, 2007 Correspondence:Sung-Ho Her, MD, Division of Cardiology, College of Medicine The Catholic University of Korea, 520-2 Daeheung-dong, Jung-gu, Daejeon 301-723, Korea Tel: 82-42-253-9505, Fax: 82-42-220-9504 E-mail: [email protected] 449 450·Korean Circulation J 2007;37:449-452 Fig. 1. Brain MRI revealed a 1.4×2.0 cm sized slight high signal mass (white arrow) in the right frontal lobe on T2-weighted axial image. MRI: magnetic resonance imaging. frontal lobe. Magnetic resonance imaging(MRI) of the brain revealed a 1.4×2.0 cm sized, slightly high signalintensity mass that was most likely a meningioma in the right frontal lobe(Fig. 1). The patient was admitted to the Department of Neurosurgery for further evaluation. The EEG recordings revealed no definite epileptic discharges. On the 7th hospital day, he had a seizure and then lost consciousness again. During the syncope event, the ECG showed a progressive decrease of the heart rate to 28 bpm and complete AV block(Fig. 2A), and the blood pressure decreased to 60/30 mmHg. Cardiac massage was initiated and some minutes later patient recovered an alert mentality with a normal sinus rhythm of 78 bpm(Fig. 2B) and a blood pressure of 90/60 mmHg. Some 6 hours later, he had another seizure and then he experienced complete AV block(Fig. 2C) with a blood pressure of 60/50 mmHg, but he did not lose consciousness. Some minutes later, the patient completely recovered spontaneously with a normal sinus rhythm and blood pressure. The patient was transferred to the Department of Cardiology for the further evaluation. Transthoracic echocardiography revealed good regional wall motion with A B C D Fig. 2. The ECG showed a complete AV block during the first syncope event in the hospital (A), recovered the normal sinus rhythm after the first syncope (B), redeveloped a complete AV block (C) and setted ventricular rate over 60 bpm by permanent pacemaker (D). ECG: electrocardiography, AV: atrioventricular, bpm: beats per minute. Ki -Hoon Park et al:Brain Tumor that Caused Bradycardia and Seizure·451 a left ventricular ejection fraction of 67%. A Holter test revealed frequent APCs and rare VPCs, but it didn’t reveal complete AV block. The coronary angiogram showed no definite abnormality. We still noted intermittent seizures with complete AV block for 5-10 seconds until the 12th hospital day. Thus, we decided to implant a permanent pacemaker. During the following days after permanent pacemaker implantation(the VVI type), we set the ventricular rate over 60 bpm, and this resulted in no bradycardia and no complete AV block or seizure(Fig. 2D). The patient did not experience any seizure and syncope attacks during the 20 days after implantation of the permanent pacemaker. Discussion Many previously published papers have shown that cardiac asystole and bradycardia, as manifestations of syncope or seizure, originate from the temporal lobe.7-9) Several studies have suggested a frontal lobe influence on the autonomic cardiovascular regulation.10-13) We report here on a patient with a complete AV block that was followed by syncope as the first sign of a right frontal brain tumor. Although we didn’t perform simultaneous ECG/EEG recordings during a period of bradycardia, we believe that the origin of the bradycardia was a brain tumor in the frontal lobe. Electrical stimulation of the cingulated gyrus and orbitofrontal cortex has produced changes in the heart rate, and cases of ictal bradycardia related to orbitofrontal lobe seizures have been reported on.14-16) The insular cortex, the central nucleus of the amygdala and some structures of the hypothalamic(paraventricular nucleus, the lateral hypothalamic area and dorsomedial nucleus) belong to the central autonomic network, which controls the pre-ganglionic sympathetic and parasympathetic visceromotor outputs. The mesial, temporal and frontal areas are interconnected to the central autonomic network so that ictal discharges arising from or spreading to these regions are more likely to induce autonomic changes.11)17) Many different regions of the nervous system are involved in the cardiovascular control(brain stem, thalamus, hypothalamus, amygdale and insular cortex). Pathology in these regions can give rise to various types of cardiac dysfunction. For instance, cortical stimulation studies in humans have shown depressor responses and bradycardia upon stimulation of the left insular cortex, whereas the converse applied for the right insular cortex.18) In humans undergoing temporal lobectomy with amygdalo-hippocampectomy for epilepsy, bradycardia and hypotension have occurred during manipulation of the amygdale and hippocampus.19) Critchley et al.20) conducted functional MRI experiments, and they reported changes in the heart rate for both cognitive and motor performance that was related to the strength of activation in the anterior cingulated cortex. In particular, the activity observed in the anterior cingulated cortex was related to sympathetic modulation of the heart rate, and this was dissociable from cognitive and motor-related activity. In conclusion, our case confirms that cardiac asystole may be a potentially life-threatening symptom during the partial seizures that were caused by right frontal brain tumor. We can also hypothesize that seizures originating in the fronto-mesial structures may disrupt a complex neural system involving the fronto-temporal-insular regions, and these regions have been implicated in the autonomic regulation of the cardiovascular responses. REFERENCES 1) van der Sluijs BM, Renier WO, Kappelle AC. Brain tumour as a rare cause of cardiac syncope. J Neurooncol 2004;67:241-4. 2) Soteriades ES, Evans JC, Larson MG, et al. Incidence and prog- nosis of syncope. N Engl J Med 2002;347:878-85. 3) Kim WJ, Kim JY, Ju HS, et al. A case of torsades de pointes indu- 4) 5) 6) 7) 8) 9) 10) 11) 12) 13) 14) 15) 16) 17) ced by complete atrioventricular block and hypokalemia. Korean Circ J 2004;34:220-3. Cha KS, Park TH, Lee CJ, et al. Torsade de pointes in advanced atrioventricular block: a cause of syncope. Korean Circ J 1998; 28:626-31. Liedholm LJ, Gudjonsson O. Cardiac arrest due to partial epileptic seizures. Neurology 1992;42:824-9. Reeves AL, Nollet KE, Klass DW, Sharbrough FW, So EL. The ictal bradycardia syndrome. Epilepsia 1996;37:983-7. Locatelli ER, Varghese JP, Shuaib A, Potolicchio SJ. Cardiac asytole and bradycardia as a manifestation of left temporal lobe complex partial seizure. Ann Intern Med 1999;130:581-3. Frysinger RC, Harper RM. Cardiac and respiratory correlations with unit discharge in epileptic human temporal lobe. Epilepsia 1990;31:162-71. Wilder-Smith E. Complete atrio-ventricular conduction block during complex partial seizure. J Neurol Neurosurg Psychiatry 1992;55:734-6. Mascia A, Quarato PP, Sparano A, et al. Cardiac asystole during right frontal lobe seizures: a case report. Neurol Sci 2005;26: 340-3. Tinuper P, Bisulli F, Cerullo A, et al. Ictal bradycardia in partial epileptic seizures: autonomic investigation in three cases and literature review. Brain 2001;124:2361-71. Leung H, Schindler K, Kwan P, Elger C. Asystole induced by electrical stimulation of the left cingulated gyrus. Epileptic Disord 2007;9:77-81. Sebastiani L, Ghelarducci B. Medial prefrontal cortex early lesion effects on classical conditioned bradycardia. Exp Brain Res 2002; 147:264-7. Oppenheimer SM, Cechetto DF, Hachinski VC. Cerebrogenic cardiac arrhythmias: cerebral electrocardiographic influences and their role in sudden death. Arch Neurol 1990;47:513-9. Pool JL, Ransohoff J. Autonomic effects on stimulating rostral portion of cingulated gyri in man. J Neurophysiol 1949;12:385-92. Wall DP, Davis GD. Three cerebral cortical systems affecting autonomic function. J Neurophysiol 1951;14:507-17. Benarroch EE. Overview of the organization of the central autonomic network. In: Bennaroch EE, editor. Central Autonomic Net- 452·Korean Circulation J 2007;37:449-452 work. Armonk (NY): Futura Publishing; 1997. p.3-28. epilepsy surgery. J Neurosurg Anesthesiol 2001;13:329-32. 18) Oppenheimer S, Gelb A, Girvin JP, Hachinski VC. Cardiovascu- 20) Critchley HD, Mathias CJ, Josephs O, et al. Human cingulated lar effects of human insular cortex stimulation. Neurology 1992; 42:1727-32. 19) Sato K, Shamoto H, Yoshimoto T. Severe bradycardia during cortex and autonomic control: covering neuroimaging and clinical evidence. Brain 2003;126:2139-52.