Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
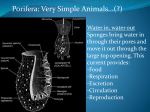
CASE REPORT Bladder Outlet Obstruction in a 5 Years Boy Badar Murtaza, Muhammad Akmal, Arshad Mahmood, Waqar Azim Niaz and Hussain Ahmad ABSTRACT We report a 5 years old boy with bladder outlet obstruction secondary to a fibroepithelial polyp of prostatic urethra. The micturating cystourethrogram showed a filling defect in the posterior urethra. Cystourethroscopy revealed a polyp in the prostatic urethra proximal to the verumontanum. Transurethral resection was done and histopathology confirmed fibroepithelial polyp of the urethra. Key words: Prostatic urethra. Polyp. Transurethral resection. Micturating cystourethrogram. INTRODUCTION Bladder outlet obstruction in children may result from a variety of causes. The common causes are posterior urethral valves, meatal stenosis, phimosis, prolapsing ureterocele or urethral diverticulum. Urethral polyps as a cause of bladder outlet obstruction are rare.1 Genitourinary tract polyps can occur anywhere from the renal pelvis to the urethra.2 These polyps are mostly found in the ureter and renal pelvis, rarely in the urethra. In children, the urethral polyps are mostly found in the first decade of life and histologically they are usually benign fibroepithelial polyps with no malignant transformation.3 These urethral fibroepithelial polyps are found more often in children than adults. Approximately 161 cases have been documented in the medical literature, this highlights the rarity of this condition.4 Fibroepithelial polyps of the urethra have often been described in boys while the occurrence in girls is exceptional. Ultrasonography and micturating cystourethrogram are useful in the diagnosis; however, cystourethroscopy remains the diagnostic procedure.1 The main aim of reporting this case was to emphasize it in the differential diagnosis for all children especially males presenting with bladder outlet obstruction. CASE REPORT pain, past history of trauma or any urethral intervention. On examination, he was a healthy boy with stable vital signs. He was neither pale nor jaundiced. The systemic examination did not reveal any abnormality. The complete blood count, urinalysis, serum urea/ creatinine and serum electrolytes were within normal limits. The ultrasound of the abdomen/KUB revealed normal sized kidneys with no hydronephrosis. The urinary bladder was also normal. He had a micturating cystourethrogram (MCUG) which showed a filling defect in the prostatic urethra (Figure 1). However, the patient was able to void with opacification of the anterior urethra as well. Accordingly, cystourethroscopy was planned under general anaesthesia. A 7.5 Fr cystoscope was used. This revealed a pedunculated polyp in the prostatic urethra, just proximal to the verumontanum, at the 6 O'clock position. Endoscopically the urethral polyp was excised with the help of the fulgration of the base of the polyp (transurethral resection). The specimen was removed, preserved in formalin and sent for histopathology (Figure 2). Foley catheter was retained. Postoperative course was uneventful. The catheter was removed the next morning and he passed urine without difficulty. The histopathology report confirmed a fibroepithelial polyp. On 3 months follow-up he was found asymptomatic with good urinary stream. A 5 years old boy reported with a 6 months history of difficulty in passing urine. According to the mother the child was asymptomatic about 6 months ago, when she noticed that the child had to strain in order to pass urine. The symptoms aggravated progressively, he started taking longer to forcibly empty the bladder. However, there was no episode of acute urinary retention. There was no history of fever, burning micturition, haematuria, Department of Urology, Armed Forces Institute of Urology (AFIU), Rawalpindi. Correspondence: Dr. Badar Murtaza, 614-C, Harley Street, Rawalpindi. E-mail: [email protected] Received February 01, 2011; accepted October 12, 2011. 780 Figure 1: Filling defect seen in the posterior urethra on micturating cystourethrogram. Figure 2: Excised specimen of fibroepithelial urethral polyp. DISCUSSION Fibroepithelial polyps are rare; however, they are the most common benign mesodermal tumours of the Journal of the College of Physicians and Surgeons Pakistan 2011, Vol. 21 (12): 780-781 Bladder outlet obstruction in a 5 years boy Multiple urethral polyps are however, a rare entity.1 These fibroepithelial polyps can be successfully excised by transurethral resection.3 Due to the proximity of the lesion to the verumontanum, care is required to avoid damage to the external sphincter. Other cystoscopic options are Bugbee fulguration of the polyp and laser excision. In some cases, especially in children with large polyps, transvesical approach is preferred.10 urinary tract. They are composed of a fibrous core covered with normal urothelium.5 Most fibroepithelial polyps occur in the ureter, then in renal pelvis and a small number in posterior urethra and bladder.4 Fibroepithelial polyps do not show malignant transformation. However, the urethral polyps having prostatic glandular tissue can undergo transformation and exhibit recurrence.6 Fibroepithelial polyps of the upper urinary tract are usually mistaken for the transitional cell carcinoma, frequently resulting in more extensive surgery than would otherwise be required for the diagnosis and treatment. REFERENCES The etiology of urethral fibroepithelial polyp remains controversial. Some consider it as a congenital anomaly. However, there are some patients who present in adulthood, thus it seems to be less likely to be congenital. There are various other hypotheses regarding the origin of these lesions. Some consider fibroepithelial urethral polyp as developmental error in the invagination process of submucous glandular material of the inner zone of the prostate gland, an abnormal protrusion of the urethral wall or epithelial changes secondary to the maternal estrogen. The fibroepithelial polyps are covered with transitional epithelium. This layer can show squamous, intestinal or rarely gastric metaplasia as well.7 Fibroepithelial polyps predominantly develops in childhood including the neonates, but may also occur in adults.8 The commonest symptoms are of bladder outlet obstruction, like urinary obstruction, urinary hesitancy or even urinary retention. In this case, the most notable symptoms were straining on micturition with prolonged act of micturition. Other symptoms like dysuria, haematuria, enuresis, urinary tract infection and flank pain may also be seen.8 Dilatation of the upper urinary tract, vesical calculus disease9 and even reflux has been documented. l l l l l 1. Jain P, Shah H, Parelkar SV, Borwankar SS. Posterior urethral polyp and review of literature. Indian J Urol 2007; 23:206-7. 2. Aita GA, Begliomini H, Mattos D. Fibroepithelial polyp of the urethra. Int Braz J Urol 2005; 31:155-6. 3. Issac J, Snow B, Lowichik A. Fibroepithelial polyp of the prostatic urethra in an adolescent. J Pediatr Surg 2006; 41:29-31. 4. William TR, Wagner BJ, Corse WR, Vestevich JC. Fibroepithelial polyps of the urinary tract. Abdom Imaging 2002; 27:217-21. 5. Brady JD, Korman HJ, Civantos F, Soloway MS. Fibroepithelial polyp of the renal pelvis: nephron sparing surgery after false positive biopsy for transitional cell carcinoma. Urology 1997; 49:460-4. 6. Mustafa M. Capillary haemangioma of verumontanum: case report and review of the literature. Inter Urol Nefrol 2006; 38:493-4. 7. Jaidane M, Hidoussi A, Slama A, Hmida W, Sorba NB, Mosbah F. Gastric metaplasia of posterior urethral polyp: a case report. Cases J 2009; 2:9119. 8. Tsuzuki T, Epstein JI. Fibroepithelial polyp of the lower urinary tract in adults. Am J Surg Pathol 2005; 29:460-6. 9. Kouranloo J. Congenital polyp of the posterior urethra and bladder stone in a 21 months old boy. Pak Paed J 2002; 26:203-5. 10. Demicran M, Ceran C, Karaman A, Uguralp S, Mizrak B. Urethral polyps in children: a review of the literature and report of two cases. Int J Urol 2006; 13:841-3. O l l l l l Journal of the College of Physicians and Surgeons Pakistan 2011, Vol. 21 (12): 780-781 781