Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Preparation of Electrocardiographic Data for Analysis
by Digital Electronic Computer
BY HUBERT V. PIPBERGER, M.D., EDWARD D. FREIS, M.D.,
B.E.E.,
AND
HENRY
TABACK,
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Materials and Methods
Three corrected, orthogonal electrocardiographic
leads (Schmitt's SVEC III system)9' 10 were recorded simultaneously on magnetic tape through
FM (frequeney modulation) channels, with use of
a tape recorder.* Differential preamplification
with a gain of 1,000 and a frequency response
flat from 0.1 to 1,250 c.p.s. was used. A fourth
direct (voice) channel permitted recording of
verbal information including identification of each
From the Veterans Administration Hospital, the
Department of Medicine, Georgetown University
School of Medicine, and the National Bureau of
Standards, Washington, D.C.
Supported in part by a grant from the American
Heart Association.
Presented at the Thirty-Second Annual Scientific
Sessions of the American Heart Association, Philadelphia, Pa., October 25, 1959.
March 1960
LEONARD
MASON, SC.D.
orthogonal electrocardiographic leads into
curves of spatial magnitude and orientation.
Such a conversion does not necessarily lead
to automatic analysis, since the newly obtained tracings must be interpreted in fashion
similar to the original records. Although a
few specific procedures are readily and economically accomplished by analog computation, the examination of large quantities of
data for relationships that may never have
been precisely formulated seems a task better
suited to the digital computer. The problem
of interpreting electrocardiographic wave
forms is believed to be primarily one of recognition of pattern. Analog devices adapted for
this use are likely to be single-purpose, and
the probability is strong that a continuing
development of equipment would be needed
to meet drastic changes of processing procedures.
On the other hand, if the researcher has
access to a general purpose digital computer,
an almost infinite variety of measurement and
analysis can be had merely by writing a new
set of instructions for the machine. Then conversion of electrical heart signals to numbers
and their storage in a form acceptable to the
computers becomes an essential preliminary
step. In the present report, a pilot facility for
accomplishing this purpose automatically is
described.
DIGITALI electronic computers are finding
increasing applications in the analysis
of medical and biologic data. The principal
advantages are high speed, relatively great
accuracy, and extreme versatility, especially
for analytic operations that are too tedious
and time-consuming for routine clinical use.
Large amounts of data can be processed on a
completely objective basis in a relatively short
time. Thus computation by commercially
available machines should facilitate extensive
statistical studies, mass screening of the population, and the data handling of patient records in large organizations such as the Veterans Administration.
The electrocardiogram was choseni for a
pilot study in automatic data processing, since
it has important clinical applications as a
diagnostic aid. The electrical signals from
the heart are repetitive and relatively well
adapted for objective mathematical treatment.
Once the feasibility of the method is established in electrocardiography, only minor
modifications of the equipment would be
required in other applications such as phonocardiography, ballistoeardiography, hemodynamic pressure and flow curves, electroencephalography, and electromyography.
Several efforts have been made in recent
years to apply analog computers to the analysis of the electrocardiogram.1-8 For example,
MeFee,' Sayers et al.,5 and Abildskov et al.7
have proposed conversion of signals from 3
Circulation, Volume XXI,
L.
*Ampex
413
Corporation, Type
FR 104.
PIPBERGER, FREIS, TABACK, MASON
414
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
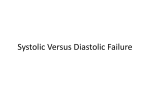
Figure 1
Equipmzeint for the neoni,ersion of electroc?ardiogralp)hic( data from th eir original analog
into dliitt..l form. Th/,u eontrol unit wiith a display osc-illosc,olpe is seen on)ri the right. The
elect.ocardiograp)hic signiaczls are r,etrieveed from the a-nalog tape recorder (on the left)
and re-recorded thr.oiigjh a digital magnetic tape re,order (second from the right, wvith
the analog- to -igital o)n,er,tehr in?iit .s lowui.er. sec(tion) The remainein q( ip)tnlent uSed
in the automiatic daitac eersion pracuss is bnilt inito the nnit which is seen secoand from
the left.
patient. The electtro(,cartdiograllphic tracings were
ca
oscilloscope )0th hemonitored on ai e,ttlhode-ranfore and during, recording. Calibration was ob
tained by recording leriodieally a 2-millivolt peaiksignal oni a,ill 3 FM clhanneXls
to-peak square
of the tal.pe -recorder. Tracingsi, of approxiima tely
<
2v0 cardiae elc>es from each of ahbout 100 patients
hlaive been recorded on eaeh tape teel.
The equipmenit for conversion of analog-to-dig,ital data was operlited by a technician sitting at the
control un-iit (figs. 1 and 2). The electrical hea rt
signals were ietrieved,as voltages fronti the magnetie tape by usingi the play-back mechanism of
the analog recorder. The operator examined these
records nit aall oscilloscope screen, ac high-speed
eleetrolic switch providing hint with sinmculta neous
dispLays of all 3 leads automatically tinted to the
heart rlate and synclhronized successively to show
similar intervals of a,is many beats a,s 111ig-ht be
desired. In (ca-ises witlh uinoai l sins rhlythm,i each
cycele will comiiprise the familiar P-QTiS-T eonp)lex. The operaitor, after viewing severa.l cycles
to clheck the essential uniformaitv of successive
complexes, pressed a "irecor.d' switch that initiated
the coinversion of the next cycle, and moniitored
it on the osc,illoscope. [f it al)lpeaxed to be nontypical (e.g.,an extr(asystole), lie backed up tlhe
analog--. tape drive and recorded an earlier (ycle.
Circulatton, Volume XXI, March 1960
COMPUTER FOR ELECTROCARDIOGRAPHIC DATA
415
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
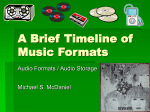
ANALOG TO DIGITAL CONVERSION SYSTEM FOR
ELECTROCARDIOGRAPHIC DATA
Figure 2
Block diagram of the equipment used for the analog-to-digital data conversion for electrocardiograms.
The remainder of the process was completely automatic, requiring no further manipulations by the
operator.
The control unit first sets the digital tape transport into motion. After a brief delay to bring
the tape up to proper speed, the format control
is activated. This apparatus fulfills several functions: (1) by controlling the analog switch it
samples each of the 3 leads X, Y, and Z 1,000
times a second; (2) it initiates the operation of
the analog-to-digital converter' which converts
the analog voltages to binary digits represented
by sets of pulses, and feeds these pulses to a
buffer which amplifies them and feeds them back
to the format control unit; (3) the latter delivers
them serially to the digital "write" electronic unit
for re-recording on digital nmagnetic tape.
The digital write electronic unit provides proper
data form and power level for energizing the
"record" heads of the digital tape recorder. At
the end of a cardiac cycle the conversion equipment receives a stop signal from the control unit,
*Epsco '"Datrac. '
Circulation, Volume XXJ, March 1960
and is then ready for the next patient's record.
Records of 1 cardiac cycle of each of approximately 1,000 patients can be stored on one reel
of digital magnetic tape.
The digital tape format was designed to be
compatible with one of the digital computers available at the National Bureau of Standards." Consequently, the information thus stored can be fed
directly into any digital computer of this type
for further processing and analysis of the electrocardiographic data as may be desired.
Results
Records of 988 patients with a variety of
electrocardiographic abnormalities were proc-
essed through the described analog-to-digital
conversion equipment and a digital computer.* An obvious test for the proper functioning of the automatic equipment is the
conformity between the original records and
graphs of the 3 processed electrocardiographic
*IBM Type 704.
416
416))
PIPRGER
FREIS, TlA\l3iCIK
MASON
1^~
:---
.1
---
--
-.
ill,--------
11
C
---f
.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
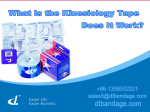
Figure 3
RecordI.4ooi fi gure 1 uif./ j JJt ti through
'('it 479v
) e+ll((Jic)tu'' itt and dljital 'ou iputer. The
trueciug wos printed ouit Min nit Oi(tn c(td furorm a0(d ye
]plotted 01 hleIvusis o f 1/is dligitail inf ot motion.
A tii}JilttidfC1ftQJ5,C
44(47 (
, ((461( tiite re Ititiotishipweire titonitoined s/eisfetrdteJ. Thisi, ti(me slto is.
ct poi tf? 4
d47t10 i'(
1l
/Il 1lt fJof/
-.
lactas ott tIil basis of Ithe digitl i)tiilt-out received froim tle coin-puter. FigTure 3 is a graphi.
of a 3-1lcatl cletrteardiogratu (pcatient C-21 )
after its conversin from tle anialogo record o07
ma-gtnetic tape, Its recad-in to tlhe diogital eorniputer, and its p)r'ini.t -otut as a colutIn of numiihers at millisecond interivals. Except where
greater resolution was reqluired acecurately to
delineate thIe ctirve oilly every fifth iiumber.
Wx as plotted. ''lhe origillnal electrocardiogram
was a sequelnee of 22 successive beats but the
l)attern of figure 3 was suifficienitly distinctive
to perllmit a sing{le tbeadit to be seleete(l from
the orig,itl recorli of 22 ceardiae eve les. Wlhe
the graphi was overlaid by the filmri recoi.cl of
that ori cinl enlarged 1 2 timles as in figure 4.
the amiplituides of the 2 (lliagralmlls were founid
to Coeille(le Withinl a trlace width a (discrel)aney far less than the heat-to-beat variabilitx
Figure 4
SttnipbJI 47e<es( off a 01[ii oyoiioi 4(1)01it'ciioljr'pin
7 front to]) to bottouit) ieployed Ifrom
Z
Icads (X.,
unulog)(J t}itoyit C?tic' to rind1)110t]ioto i'ttphir(1 front all
suc i os eo pe seercn.
of alln average11 eel ltclLogtai. A n umber
of other diatients (liitizedl records. )lotteCl1
a1t 10-mlillist leod intervals, showeed eqiuallv
coodclorrespondene. Thlins, it hias been dentrou.stcateh thalt tlhe faeility used for eonversro
and lligital storagi)e of eleearlliographie
data performs satisfactorily an1d eliably.
Discussion
As i)oilnted otut above, logical anid miathe-mcatical operattionis Oni electrocardiogralphic
dlata in digital formn afford a high degree of
fiexibilitv O nce the sitgllnls are stored on digital magnetli tape iii a suiitable format, onlyl
ptroper progriamming of a digital eomnputer is
requirll tto pr.ovide a great xariiety of anialytic
procedrles. rT is flexibility appears espeeially
iiutporta i-t for the establishlment of clinlic(al
norms and the discovery of inew diagnostic
Circulation, Volume XXI, March 1960
COMPUTER FOR ELECTROCARDIOGRAPHIC DATA
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
procedures. Wheln these have been tested by
experience, a special-purpose computer for
electrocardiographic data might then be designed, to replace the general purpose equipment described in this report. The size and
cost of the required apparatus might then be
brought down within the reach of an average
hospital.
Objective data analysis with computers
could provide a considerable increase in diagnostic accuracy, since subjective and descriptive criteria for electrocardiographic interpretation can be replaced by quantitative
statements. Rather elaborate analytic and statistical procedures take only a few seconds
on a digital computer and so pose no major
problems. Also the electrocardiographic information can be supplemented by salient
facts from the patient's history and physical
examination, which can be entered into the
digital computer on punched cards. There are
no instrumental limitations, therefore, for
providing a more broadly based computer program as an aid in electrocardiographie diagnosis. The total information thus available
would greatly facilitate statistical correlations
of various parameters.
Magnetic tape provides a convenient medium for recording and storing electrocardiographic tracings. The original analog tape can
be used at any time for the display of old
records either on an oscilloscope in scalar or
vectorial form or, if so desired, for re-recording old tracings on paper. Considerably less
storage space is required for magnetic tape
than for conventional recording media.
The described equipment requires only
minor changes to make possible the inclusion
of other diagnostic methods for cardiac evaluation. Modifications for phonocardiography,
respiratory volume curves, and pulse tracings
are presently being made.
Summary
A pilot facility for automatic processing of
electrocardiograms leading to their analysis
by digital computer has been described. Wave
forms from orthogonal electrocardiographic
leads were recorded on magnetic tape. By
Circulation, Volume XXI, March
1960
417
means of newly designed conversion equipment these records have beern converted from
their original analog form into digital form.
The further processing and analysis of the
data thus becomes feasible through the use of
commercially available digital electronic computers. It has beeln demonstrated that the
electrocardiographic tracings as recorded
from patients can be reproduced from the resulting numerical print-outs in their original
and undistorted formn. The further analysis
of these records theii requires only proper
programming of a digital computer. The same
equipment with minor modifications can be
used for automatic processing of other analog
data such as phonocardiograms, pulse tracings, and ballistocardiograms.
Summario in Interlingua
Es describite un arrangiamento de dispositivos pro
le manipulation automatic de electrocardiogrammas
preparatori a lor analyse per medio de un computator
digital. Formas de unda ab orthogone derivationes
electrocardiographic esseva registrate in bandas magnetic. Per medio de un novemente elaborate dispositivo de conversion iste registratioiies esseva convertite
ab lor forma original analoge a in un forma digital.
Le cetere processage e le analyse del datos deveni
assi effectuabile per le uso de commercialmente disponibile computatores electronic digital. Il ha essite
demonistrate que le registrationes electrocardiographic
obtenite ab le patientes pote esser reproducite ab le
resultante configuration numeric in lor forma original
sin ulle distorsion. Le ainalyse additional de iste
registrationes require alora solmente le appropriate
programmation del computator digital. Le mesme
apparatura con minor modificationes pote esser usate
pro le processage automatic de altere datos analoge
como per exemplo illos del phonocardiogramma, de
registrationes de pulso, e del ballistocardiogramma.
References
1. MCFEE, R.: A trigonometric computer with electrocardiographic applications. Rev. Scient.
Inst. 21: 420, 1950.
2. JOHNSTON, F. D., MCFEE, R., AND BRYANT, J.
M.: An integration circuit for measurement
of the areas of the wxaves in the electrocardiogram. Circulation 2: 5, 1950.
3. BRILLER, S. A., MARCHAND, N., AND KOSSMANN,
C. E.: A differential vectoreardiograph. Rev.
Scient. Inst. 21: 805, 1950.
4. SIMONSoN, E., SCIIMITT, 0. H., DAHL, J., FRY,
PIPBERGER, FREIS, TABACK, MASON
418
D., AND BAKKEN, E. E.: The theoretical and
experimental bases of the frontal plane ventricular gradient and its spatial counterpart.
Am. Heart J. 47: 122, 1954.
5. SAYERS, B. MCA., SILBERBERG, F. G., AND DURIE,
D. F.: The electrocardiographic spatial magnitude curve in man. Am. Heart J. 49: 323,
1955.
6. NEWMAN, E. V., McGOVERN, J. F., AND ARNOLD,
T. G.: The important recent advances in
electrocardiography. Arch. Int. Med. 96: 591,
1955.
7. ABILDSKOV, J. A., INGERSON, W. E., AND HISEY,
B. L.: A linear time scale for spatial vectorcardiographic data. Circulation 14: 556, 1956.
8. BRILLER, S. A.: The integrated electrocardiogram. Ann. New York Acad. Se. 65: 894,
1957.
9. SCHTUITT, 0. H., AND SIMONSON, E.: The present
status of vectorcardiography. Arch. Int. Med.
96: 574, 1955.
10. PIPBERGER, H. V.: Current status and persistent
problems of electrode placement and lead systems for vectoreardiography- and electrocardiography. Progress in Cardiovase. Dis. 2: 248,
1909.
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Dollery, C. T., Harington, M., and Kaufmann, G.: The Mode of Action of Chlorothiazide in Hypertension. Lancet 1: 1215 (June 13), 1959.
In a series of experiments it was demonstrated that chlorothiazide potentiates the
ganglion-blocking agents (as exemplified by pentolinium) by causing a reduction in
plasma volume. A negative sodium balance was observed in 11 patients, but the extent
of this did not correlate well with the development of increased sensitivity to pentoliniuim.
There was better correlation with the changes in plasma volume. In 8 of 13 patients
studied, 3 days' treatment with chlorothiazide produced a fall in plasma volume and all
of them showed an increased sensitivity to pentolinium. In 4 out of 5 in whom there
was no significant change in plasma volume, the effect of pentolinium was unchanged.
Replacement of the calculated loss in plasma volume with salt-free Dextran in 7 patients
was followed by reduction in sensitivity to pentolinium to about the pre-chlorothiazide
level in all except 1. It was thought unlikely that chlorothiazide had any direct hypotensive action, since no change in blood pressure nor potentiation of ganglion blockade
was observed after intravenous injection of large single doses. The sensitivity to pentolinium did not develop until the second day. This was not true with the non-quaternary
ailmonium compounds such as Mecamylamine and Pempidine. Since there was a slight
shift of the urinary pH toward the alkaline side on first giving chlorothiazide, there
was a resultant reduction in the renal excretion of these latter drugs, and therefore an
increased hypotensive effect. The potentiating effect of chlorothiazide on pentolinium
particularly affected the postural drop of blood pressure. Some postural hypotension
was observed as a response to chlorothiazide itself in 4 of 13 patients. Three of these
had a considerable fall in plasma volume while the fourth had an extensive sympathectomy previously. The postural response was abolished in each case by the infusion of
sufficient Dextran to replace lost plasma volume.
SHEPS
Circulation, Volume XXI, March 1960
Preparation of Electrocardiographic Data for Analysis by Digital Electronic
Computer
HUBERT V. PIPBERGER, EDWARD D. FREIS, LEONARD TABACK and HENRY
L. MASON
Downloaded from http://circ.ahajournals.org/ by guest on June 18, 2017
Circulation. 1960;21:413-418
doi: 10.1161/01.CIR.21.3.413
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1960 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://circ.ahajournals.org/content/21/3/413
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles
originally published in Circulation can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of
the Web page under Services. Further information about this process is available in the Permissions
and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/