Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
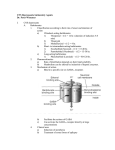
Sedative Hypnotics and Their Use and Misuse John C. Mutziger DO, FAOAAM January 24,2015 Prevalance of Abuse NIH 2011 - 2014 • 12th graders – 68.2% alcohol 38.1% cigarettes 17.2% smokeless tobacco 50.4% illicit drugs 4.5% cocaine 7.6% hallucinogens 7.7% tranqualizers 11.1% opioids Barbiturates • • • • Synthesized originally in 1864 by von Bayer 1903 Barbital was synthesized (Veronal) 1912 Phenobarbital was synthesized These were the drug of choice during days leading up to the development of Benzodiazepines • Benzodiazepines were developed in the 1950’s • 1954 Dr. Leo Sternback found chlordiazepoxide Barbiturates Types of Barbiturates • Ultrashort Short acting Generic Therapy methohexital General thiopental anesthesia pentobarbital Sedation secobarbital Seizures amobarbital Hypnotic Types of Barbiturates • Intermediate butabarbital butalbital Hypnotic, seizures, HA’s phenobarbital mephobarbital Sedation, and seizures Long Acting Barbiturates • Are highly lipid souluble • Are excreted through hepatic metabolism and then renal excretion • Favored through alkalinization of the urine • Half-lives are increased in pregnancy and in patients with chronic liver disease • Depresses respiratory drive • Hepatic metabolism is responsible for tolerance by induction Benzodiazepines • Next in 1963 diazepam was developed (Valium) • Thereby leading to the Age of Anxiety – 20th Century • These were used for many uses – sedative, hypnotic, anxiolytic, amnesic. How Do They work? • Both the benzodiazepines, barbiturates and the new non-benzodiazepines are modulated at the GABAa receptor. • GABAa is a ligand-gated Cl- channel • When stimulated it gives a fast inhibitory postsynaptic potential- therefore is allostericaly activated by benzodiazepines; it reduces the probability of generation of an active potential GABA beta • This is a G protein coupled receptor that acts as a dimer- Increases permeability to K+ and decreases Ca++ conductance • For barbiturates there is a positive modification of GABAa via allosteric mechanism that increases its effect; in other words, it is a direct GABAa agonist and prolongs the opening of the Cl- channel, esp. at B2 and B3 subunits GABA a Receptor GABAa Receptor GABAa Receptor How Benzos Work Non-benzodiazepines Zolpidem (Ambien) Zalepom (Sonata) Zopidone (Lunesta) These may act through overlapping binding sites at alpha and beta subunits • These drugs inhibit flumitrazepam • • • • Benzodiazepines • Rx. peaked in 1975 – 10% of all prescriptions • They are prescribed mainly for anxiety and insomnia now • They are relatively safe with rare OD’s • Are addicting • Are taken with other drugs Clinical Uses of Benzodiazepines • Anxiety disorders – Acute anxiety – Generalized anxiety disorder – Panic disorder – Phobias (social, simple) – PTSD – Obsessive-compulsive Disorder Clinical Uses of Benzodiazepines • Insomnia • Anxiety associated with medical illness – Cardiovascular – Gastrointestinal – Somatoform disorder Clinical Uses of Benzodiazepines • • • • • • • Convulsive Disorders Acute status epilepticus Neonatal seizure disorders Preeclampsia Tetanus Adjunct to other anticonvulsants Amnestic (before surgery or procedure) Clinical Uses of Benzodiazepines • Spastic disorders and other types of acute muscle spasm – cerebral palsy, multiple sclerosis, paraplegia secondary to spinal trauma • Involuntary movement disorders – restless leg syndrome, akathisia associated with neuroleptic use, choreiform disorders and myoclonus Clinical Uses of Benzodiazepines • Detoxification from alcohol and other substances • Agitation or anxiety associated with other psychiatric conditions – acute mania, psychosis, anxiety with depression, impulse control disorder, catatonia or mutism • Other adjunctive uses- surgery, dentistry, diagnostic procedures, cardioversion, chemotherapy Toxicity and Side Effects • With the introduction of chlordiazepoxide (Librium) in 1960, these agents replaced barbiturates as sedative-hypnotics. • They cause significantly less respiratory depression and are rarely lethal by themselves in an overdose. Toxicity and Side Effects • • • • Drowsiness, lethargy Ataxia, muscle incoordination Seizures, if abruptly discontinued Hypotonia, dysarthria, dizziness, and even hyperactivity Characteristics of Benzodiazepines • High Potency – Alprazolam (Xanax) – Lorazepam (Ativan) – Trizolam (Halcion) Characteristics of Benzodiazepines • Drugs with a long half life – Clonazepam (Klonopin) – Chloradiazepoxide (Librium) – Clorazepate (Tranxene) – Diazepam (Valium) – Flurazepam (Dalmane Characteristics of benzodiazepines • Drugs with a short half-life – Oxazepam (Serax) – Temazepam (Restoril) Mechanisms of Abuse Hedonic uses Tolerance Withdrawal syndrome Benzodiazepines with rapid onset have the greatest risk for this type of abuse • Tolerance causes patients to escalate the dose • Withdrawal syndrome appears on decreasing dosage or discontinuation • • • • Mechanisms of Abuse • Tolerance develops as decreased responsiveness to GABAa receptors to Benzos • Some evidence too that mRNA involved with the synthesis of alpha1 part of the GABAa site are reduced during long exposure to Benzos • Glutamatergic system may also play a role in the withdrawal syndrom Abuse Liability • Benzodiazepines occupy a intermediate position of abuse liablity • Barbiturates and methaqualone had a greater risk of liabilty Toxicity • When used alone – low risk • However when used with other types of medications, they act synergistically with other CNSdepressants, sedating antidepressants, neuroleptics, anticonvulsants, antihistamines and alcohol, with and without opiates Toxicity and Drug Interactions • Psychomotor retardation – drowsiness, poor concentration, ataxia, dysarthria, motor incoordination, muscle weakn ess, vertigo and mental confusion. • Memory impairment – Benzos induce anterograde amnesia. This appears separate from sedation as an effect. Toxicity and Drug Interactions • Paradoxical Disinhibition – Increased excitement, irritability, aggression, hostility, and impulsivity may occur. • This paradoxical disinhibition may in rare cases result in attacks of rage or violence or other antisocial behaviors. They are more common in children and the elderly Toxicity and Drug Interactions • Depression and emotional blunting – there is an association between Benzos use and depressive symptoms, and in some cases the emergence of suidical ideation. • Dependence – may appear as early withdrawal or protracted withdrawal in patients. Abuse of benzodiazepines • • • • Approximately 80% is polydrug abuse Rarely alone Usually with opioids 3-41% abuse with ethanol Abuse of Benzodiazepines • Increased risk of abuse – High potency – Short duration of action – High purity – Water solubility – High volatiltiy Benzodiazepine Overdose • • • • • • • Dizziness Confusion Drowsiness Blurred vision Unresponsiveness Anxiety Agitation Trends in Drug Use Physical Exam Findings • • • • • • • • • • • Nystagmus Hallucinations Slurred speech Ataxia Coma Hypotonia Weakness Amnesia Paradoxical excitation Respiratory depression Hypotension Diagnosis • • • • • • • • Immunoassay screening Get ABG’s, CXR, Pregnancy test Serum electrolytes Glucose Bun Cr Ethanol level Acetaminophen level Pearls • Benzodiazepine risk increases with age • Women are as twice as likely to receive a benzodiazepine Rx. • ¼of all Rx. for benzodiazepines are for long acting • Men are more likely to abuse with opioids Withdrawal Symptoms • • • • • • Insomnia Gastric problems Tremors Agitation Fearfulness Muscle Spasms Withdrawal Symptoms • Less likely – – – – – – – – – Irritable Depersonalization Derealization Hypersensitive to stimuli Suicidal behavior Depression Psychosis DT’s Seizures Contraindications to Use • • • • • • Respiratory depression Myasthenia gravis Sleep apnea Bronchitis COPD Caution: Personality disorders, depression, pregnancy, elderly Pharmacokinetics • • • • • • • • Benzo ½ Life Alprazolam 12-15 hrs Chlordiazepoxide 10-30 Clonazepam 18-50 Diazepam 20-80 Lorazepam 10-20 Oxazepam 5-10 Prazepam 50-200 Speed of onset Intermediate Intermediate Slow Fast Intermediate Slow Slow Drug Interactions • With drugs metabolized by cytochrome P450 enzymes • With drugs metabolized through glucuronidation • Oral contraceptives, some antibiotics, antidepressants, antifungal agents inhibit the cytochrome enzymes in the liver • Carbamzepine and phenytoin accelerate may benzodiazepines. Drug Interactions • Common – Ketoconazole – Itremazole – Macrolide antibioitics – Fluoxetine – Nefozodone – Cimetidine Benzodiazepine Use and Risk of Alzheimer’s Disease • On Sept 9, 2014 published in the BMJ by Sophie Billioti de Gage et al • Conclucion – Benzodizepine use is associated with an increased risk of Alzheimer’s Disease. ͞ The stronger the association observed for long term exposures reinforces the suspicion of a possible direct association, even if benzodiazepine use might also be an early marker of a condition associated with an increased risk of dementia. Unwarranted long term use of these drugs should be considered as a public health concern.͟ Benzodiazepine Use and Risk of Alzheimer’s Disease • Use of benzos significantly associated with an increased risk of Alzheimer’s Disease. • 1.52 odds ratio for any use • 1.85 odds ratio for long term use (6 months or more) • 1.72 for use of benzos with a long half life. • This was a case-control study; not a randomized, controlled trial. Guidelines for the use of benzodiazepines in Office Practice • Contra-indications: – Pregnancy and risk for pregnancy – Active substance abuse, including alcohol – Medical and mental health problems that may be aggravated by Benzos…..including fibromyalgia, chronic fatigue syndrome, bipolar disorder, ADHD, kleptomania and other impulse control disorders. Sleep apnea, COPD, CHF. – Pt.s being treated with opioids for chronic pain or replacement therapy for narcotic addiction. – Grief reactions. Indications for short-tem treatment with Benzos • Short term treatment of anxiety disorders – 2-6 weeks. • Insomnia- short term 1-2 weeks. • Muscle relaxant- short term 1-2 weeks. • Urgent treatment of acute psychosis and agitation. • Treating alcohol detoxication • Seizures • Sedation Indications for long term use of Benzodiazepines • May be used longer in the terminally ill • Certain neurological disorders • Severely handicapped Tapering Benzodiazepines • A long term project • Start slow, starting with ½ of a tablet every 2 weeks (or 10% of the daily dose of the BZD) • May switch to an equivalent dose of a long acting BZD or phenobarbital and then taper off • Counseling should be available • Carbamazepine, valpoate, and gabapentin can be used to facilitate more rapid withdrawal. Special Considerations • Care to not taper alprazolam too quickly…more prone to withdrawal seizures • Patients with other addiction problems or on high doses or taking other opiates will be more difficult to withdraw. Consider consult. • As patients age, they become more sensitive to the same dose of BZD. • There is risk to operating machinery even with stable doses of BZD’s. Equivalence Table Alprazolam (Xanax) .5 mg. Chlordiazepoxide (Librium) 25 mg. Clonazepam (Klonopin) 0.5 mg. Diazepam (Valium) 10 mg. Lorazepam (Ativan) 1 mg. Temazepam (Restoril) 20 mg. Zolpidem (Ambien) 20 mg. Zaleplon (Sonata) 20 mg. Eszopiclone (Lunesta) 3 mg. Bibliography • Substance Abuse – Fourth Edition • Principles of Addiction – Fifth Edition • The Pharmacological Basis of TherapeuticsGoodman and Gilman • Drug Information Service – University of Texas Health Center at San Antonio and the College of Pharmacy at Austin