Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Case Presentation
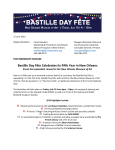
This 75-year-old lady, presented to us with ulcerated lesions on her face.
She had no history of trauma to the face or any contact with a chemical
substance. She had difficulty feeding due to severe pain in her oral cavity
and lips.
On physical exam, she was found to have diffuse crusting lesions over her
upper lip, nasal tip, lower lip, as well as on her upper and lower gingivae and
her hard palate (Figure1). Scraping the lesions gently shows them to be
friable, with a bloody base beneath the crust.
A biopsy was taken from these lesions by the bedside and was sent to
pathology.
Figure 1. Lesions of lips, nasal tip and ingivae.
DIAGNOSIS: Noma (Cancrum Oris)
Discussion
Noma has been referred to as “maladie dévoreuse de beauté et de vie” ("An
illness devouring beauty and life”) by Edmond Kaiser, founder of the
humanitarian organization Sentinelles. The word originates from the Greek
verb numein meaning “to devour”. This gangrenous disease affects soft and
hard tissues of the mouth and face, and occurs predominantly in children of
less developed countries having poor hygienic conditions and debilitating
diseases. The disease is severely disfiguring, and thus it has also been
named “the face of poverty”. The cause of cancrum oris is unknown, but it is
presumed to be infectious in origin. Some of the risk factors include Malaria,
malnutrition, measles, and poor oral hygiene.
Cancrum oris occurs in several forms. The classic form of the disease
mostly affects children between 3 and 6 years of age in less developed
countries. Another form, Noma of the debilitated adult, is less locally
invasive, and occurs in immuno-compromised adults with major debilitating
diseases in both developed and developing countries. A third form, Noma
neonatorum, has been called Noma due to similarity of the facial lesions but
it is a different disease affecting premature babies mostly. This form may
also include necrosis of the perineal region, which is fatal in almost all cases
because of irreversible septicaemia. It is important to remember that Noma
neonatorum is a discrete pathological entity that should not be confused with
the classic form of Noma.
The disease starts as an acute necrotizing gingivitis, followed by an acute
stage, of unknown duration. The first sign of acute noma is edema of the
cheek, gingiva, or both, followed by necrotising stomatitis, until bone is
exposed with exfoliation of teeth. The course of disease is very rapid and
death can occur only a few days after the onset of edema.
Clinically, most cases are unilateral. If the disease progresses, it may present
with anorexia, prostration, fetid odour, excessive salivation, and
occasionally local adenopathy. Pain and fever are common. Secondary
infections occur very rapidly, and most children die at this stage because of
starvation, aspiration pneumonia, or sepsis.
Consequences of Noma include healing by fibrous scars which may lead to
definitive strictures of the mouth. Other consequences include severe dental
malposition and salivary incontinence. Defective speech and nasal
regurgitation occur when the maxilla is lost.
The introduction of nutritional rehabilitation, local disinfection, & broad
spectrum antibiotics at the earliest stage can halt the disease. Other
treatments for the acute phase include rehydration and improved oral
hygiene. Physiotherapy may be helpful for the prevention of mouth
contractures. However, if the disease is more advanced, the only possible
treatment is reconstructive surgery. This is one of the most challenging
problems for surgeons, with each case requiring an individualized approach.
Several factors can aid in the prevention of noma and its sequelae, including
early recognition, appropriate diagnosis, correct understanding of the disease
process, and attempts at directed preventive and therapeutic strategies. A
multidisciplinary team approach is needed for optimum research and
management strategies. Noma is preventable if the disease is detected and
recognized at an early stage.
REFERENCES
1. Auluck A. Pai KM. Noma: life cycle of a devastating sore - case report and
2.
3.
4.
5.
6.
7.
literature review, Journal (Canadian Dental Association). 71(10):757, 2005 Nov
Berthold P. Noma: a forgotten disease, Dental Clinics of North America.
47(3):559-74, 2003 Jul.
Baratti-Mayer D. Pittet B. Montandon D. Bolivar I. Bornand JE. Hugonnet S.
Jaquinet A. Schrenzel J. Pittet D. Geneva Study Group on Noma. Noma: an
"infectious" disease of unknown aetiology, The Lancet Infectious Diseases.
3(7):419-31, 2003 Jul.
Enwonwu CO. Falkler WA. Idigbe EO. Oro-facial gangrene (noma/cancrum oris):
pathogenetic mechanisms, Critical Reviews in Oral Biology & Medicine.
11(2):159-71, 2000
Falkler WA Jr. Enwonwu CO. Idigbe EO. Microbiological understandings and
mysteries of noma (cancrum oris), Oral Diseases. 5(2):150-5, 1999 Apr
Valadas G. Leal MJ. Cancrum oris (noma) in children, European Journal of
Pediatric Surgery. 8(1):47-51, 1998 Feb.
Adolph HP. Yugueros P. Woods JE. Noma: a review, Annals of Plastic Surgery.
37(6):657-68, 1996 Dec.