Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
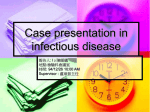
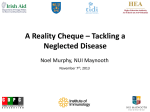
192 Skin Features Accompanying Imported Human African Trypanosomiasis: Hemolymphatic Trypanosoma gambiense Infection Among Two French Expatriates With Dermatologic Manifestations Khaled Ezzedine, MD,*† Hervé Darie, MD,† Michel Le Bras, MD, PhD,† and Denis Malvy, MD, PhD*† *Travel Clinics and Tropical Disease Unit, Department of Internal Medicine, Infectious Diseases and Tropical Medicine, University Hospital Center, Bordeaux, France; †Centre René Labusquière (Tropical Disease Branch), University Victor Segalen Bordeaux 2, Bordeaux, France DOI: 10.1111/j.1708-8305.2007.00114.x D ermatologic conditions are commonly encountered among returned travellers and longterm residents of the tropics.1 Indeed, many serious infections acquired during travel or stay in tropical countries are associated with skin manifestations that may provide important diagnostic and care clues. The location of lesions, their pattern, and the presence of associated symptoms such as pruritus or fever are important to consider in establishing a prompt and appropriate diagnosis. This critical circumstance is illustrated by the following case reports that describe two French expatriates with human African trypanosomiasis due to Trypanosoma brucei gambiense who had been diagnosed with delay, at the hemolymphatic stage of the disease and within a presentation comprising characteristic although sparsely reported cutaneous involvement. Case Reports Patient 1 A 37-year-old French expatriate worker was evacuated from Libreville, Gabon, to be admitted in our clinic because of a febrile illness with fatigue, anorexia, and arthralgias. The patient had been in vigorous health 8 months earlier when he experienced the onset of a febrile presentation with prosCorresponding Author: Khaled Ezzedine, MD, Centre René Labusquière, Université Victor Segalen Bordeaux 2, 146, Rue Léo Saignat, F-33076 Bordeaux CEDEX, France. E-mail: [email protected] tration, intermittent posterior-located headache, severe arthromyalgia, and intense residual fatigue. Despite the lack of anorexia, the patient acknowledged an involuntary progressive weight loss accounted to 1 kg/month. Five months later, he developed recurrent insomnia episodes accompanied with dermatologic manifestations owing for a diffuse, blanching, macular rash located on the two arms and on the trunk. Simultaneously, an intense pruritus of the trunk aggravating an acute paravertebral paresthesia sensation was noted. Three weeks before admission, he developed laterocervical lymphadenopathies accompanied by a raise of the body temperature as high as 41°C. The patient is a French man working in Central Africa for 15 years. He had successively lived in Congo, Cameroon, Guinea, and then in Gabon and worked in rural forest areas. He had been diagnosed 4 years before for infection with the filarial worm Loa loa and was efficiently cured. His medical history was otherwise unremarkable. At admission, the body temperature was at 39.5°C and the pulse was 90. The blood pressure was 120/70 mm Hg. On physical examination, a macular rash involved the right shoulder (Figure 1), the right pectoral part of the anterior trunk (Figure 2), the left axillae, and the left arm. They appeared as polycyclic plan plaques of 3 to 9 cm in diameter surrounded by an intense erythematous peripheral border and a blancher center. Mobile, tender cervical and occipital lymphadenopathies, 1 to 2 cm in diameter, were also palpable. © 2007 International Society of Travel Medicine, 1195-1982 Journal of Travel Medicine, Volume 14, Issue 3, 2007, 192–196 Skin Features Accompanying Imported Human African Trypanosomiasis Neurological examination was poorly remarkable, showing right and left palmomental reflexes. The patient was sound. The sensation and muscle strength were normal. Laboratory findings failed to reveal anemia; the erythrocyte sedimentation rate was 55 with a considerable elevated serum IgM antibody level of 25 g/L (normal range, 0.9–2.9 g/L). Evaluation of a peripheral blood smear as well as a lymph node fluid aspirate specimen confirmed the diagnosis and showed trypanosomes. The immunological evaluation by passive hemaglutination antibodies test showed an elevated serum-specific IgG at a titer level of 1/64 and a positive enzyme-linked immunosorbent assay test for specific IgM. Examination of the cerebrospinal fluid (CSF) demonstrated a normal cell count, a CSF smear after centrifugation without trypanosome, and a slight elevated level of nonspecific IgM antibodies (2.8 µg/100 mL). The patient was diagnosed with human African trypanosomiasis probably due to T brucei gambiense, and he received a diagnosis of the hemolymphatic stage of the disease, characterized by the absence of involvement of the central nervous system (CNS). He was efficiently and conveniently treated with a regimen of 10 doses of intravenous pentamidine isethionate at a dose of 4 mg/kg over 21 days. The clinical symptoms improved within a few days, the biological abnormalities resolved, and the serological testing was negative within 6 weeks. The patient remained asymptomatic 3 years later. Figure 1 Circumscribed, polycyclic plan plaque of 7 cm diameter surrounded by an intense erythematous peripheral border and a blancher center of the right shoulder (patient 1). 193 Figure 2 Circumscribed, macular erythematous rash of the upper right pectoral area (patient 1). Patient 2 A 72-year-old man living in Libreville, Gabon, was referred with a diffuse and intense pruritus. His medical history was remarkable for chronic prostatitis treated by sequential antibiotic regimen courses and uncomplicated malaria attacks. The patient had been in apparent healthy status 5 months earlier when he developed an irregular febrile presentation, accompanied by asthenia, an involuntary weight loss of 10 kg, and an intense and generalized pruritus predominant to the trunk and the two upper limbs. The cutaneous condition became rapidly unbearable and was not soothed by the application of local emollient and corticosteroids, and the administration of oral antihistaminic drugs. The body temperature was 38°C, and the pulse was regular at 85. Blood pressure was 110/70 mm Hg. Tender, mobile, bilateral cervical, axillary lymph nodes, 1 to 2 cm in diameter, were found. There was neither hepatomegaly nor spleen enlargement. The remaining integument and the other physical findings, including those of the neurological examination, were unremarkable. Laboratory findings reported an erythrocyte sedimentation rate at 81 and an elevated aspecific serum IgG and IgM antibody levels of 29 and 22 g/L, respectively. Examination of a thin smear of peripheral blood allowed the observation of sparse trypanosome brucei trypomastigotes. The examination of the aspirate fluid obtained from lymph node puncture was negative. Examination of CSF demonstrated a normal cell count, no biochemical abnormalities with normal protein level. Assessment of a sample of CSF after centrifugation disclosed no evidence of trypanosomal involvement. The serological evaluation of serum sample J Travel Med 2007; 14: 192–196 194 by agglutination and indirect immunofluorescence tests were positive, with antibody titer level accounting at 1/64 and 1/160, respectively. The serological testing of CSF was negative. Encephalic computerized tomography scan was normal. Electrocardiogram and chest X-ray were normal. The patient was diagnosed with human African trypanosomiasis probably due to T brucei gambiense with hemolymphatic stage involvement. The patient received a regimen of 10 doses of intravenous pentamidine isethionate at a dose of 4 mg/kg over 21 days. The symptoms and blood parasitic involvement improved within 5 days. The specific serological findings became negative over 2 months. Three years later, the patient remained asymptomatic. Discussion Human African trypanosomiasis, also known as sleeping sickness, is acquired through the bites of infected bloodsucking tsetse flies of the genus Glossina. Concerning the risk of transmission to the expatriates, occupation may affect exposure to tsetse flies. Indeed, among such overseas residents, an assessment of environmental hazards to which they were potentially exposed is an important issue to assess prompt diagnosis.2,3 Some exotic dermatoses are acquired by individuals who visit rural areas or wander off the usual tourist routes. Concurrently, the occupation activity of a variety of overseas field-workers may be associated with a high-risk exposure to a diversity of vectors and infectious agents because of their job requirements and location. Human African trypanosomiasis is endemic in a belt running across Africa. The two patients have surely been infected by T brucei gambiense, which is the cause of the infection in West Africa and accounts for humans to represent the main natural reservoir. In this epidemiological form of the disease, transmission of the infection occurs endemically in rural, forested areas, particularly near rivers or watering spots, where humans most frequently come into contact with tsetse flies. So, tourists rarely acquire T brucei gambiense infection because they seldom visit the focal rural areas of Central and West Africa where the disease is transmitted, although worker residents may be sparsely concerned.4–6 Contrarily, Trypanosoma brucei rhodesiense is the agent of disease in East Africa to the east and south J Travel Med 2007; 14: 192–196 Ezzedine et al. of the Lake Victoria. It is a zoonosis primarily affecting wild animals. It causes sporadic human cases of infection as human individuals may intrude into the cycle that normally involves only the vectors and game animals. It affects especially hunters, honey and beeswax gatherers, and tourists mostly participating in organized photographic or hunting safaris.7 African trypanosomiasis is characterized by the development of a lesion at the inoculation site, followed by parasitemia, hemolymphatic involvement associated with blood smear invasion and lymph nodes development at the draining sites, and eventually invasion of the CNS, which leads to meningoencephalitis, cerebral atrophy, and death. Trypanosoma brucei gambiense infection is a quite indolent lymphoma-like disease, progressing over months to years, reflecting the partial adaptation of T brucei gambiense to its reservoir host. A key feature of the host response is generalized immunosuppression, which is accompanied by polyclonal activation of B cells and leads to the production of large amounts of nonspecific IgM, as was observed in our two reported cases. The first sign of infection is a painful chancre, which develops at the site of the tsetse fly bite within 1 to 2 weeks after the bite. It is typically a large (2–5 cm in diameter), erythematous, indurated, fixed cutaneous swelling, and it may ulcerate. Unfortunately and contrarily to the noisy aspect of numerous rubbery inflammatory lesions occurring during the T. brucei rhodesiense infection, it is seldom evident in patients infected with T brucei gambiense4,8 as the infection is often a unique, circumscribed, indurated nodule and as the latter may not be reported because the patient assumes it to be an insect bite or mistakes it for a focal cellulitis. The frequent localizations are legs, knees, groin, and axillae. Resolution occurs within a few weeks. During the hemolymphatic stage of the disease, parasites enter the blood stream and intermittent episodes of high fever develop. The acute septicopyohemic-like course of T. brucei rhodesiense infection tends to blur the distinction between the stages of the disease, and patients have a narrower range of organ failure and hemologic symptoms before the onset of coma than those infected with T brucei gambiense. A characteristic, although exceptionally reported among less than 10% of cases, evanescent macular rash may be present, with typical polycyclic erythema plaques called trypanides and urticarial rashes occurring on the trunk or the proximal side of the limbs.9 This rash may be hemorrhagic. 195 Skin Features Accompanying Imported Human African Trypanosomiasis It is more easily observed among patients with light phototype skin. The presentation of patient 1 is remarkable as these above rarely recognized eruptive manifestations were on the forefront of the physical examination. These features are probably underlined by neighbored immunopathogenic mechanisms encountered through other sepsis-related eruptive conditions such as the erythematous macules known as “rose spots” of typhoid fever due to Salmonella typhi.10 The even isolated intense pruritic condition is a common manifestation of tropical imported diseases. It usually accompanies a helmintic infection11 or may reveal an advanced stage in the course of an unrecognized or treated human immunodeficiency virus infection/acquired immunodeficiency syndrome or the onset of a lymphoma involvement. The other dermatologic signs may account for localized cutaneous edema of the hand, feet, or face. They are more frequent at the advanced stage of the infection. The diagnosis of African trypanosomiasis rests on identification of the parasite that can often be found in blood smear or in wet blood preparations, with examination of buffy coat. Lumbar puncture is mandatory in all patients with confirmed or suspected African trypanosomiasis. Beside the presence of trypanosomes in the CSF, abnormal findings may suggest invasion of the CNS. Indeed, a white cell count greater than 5/µL is often used to define the stage of invasion of the CNS.12,13 Herein, the choice of therapy is determined by the subspecies of trypanosomes and the presence or absence of involvement of the CNS. Hemolymphatic T brucei gambiense infection is generally treated with intravenous pentamidine, which can have some adverse effects including hypoglycemia and hypotension. Therefore, in the jeopardized issue concerning the indication, the availability, the efficacy, and the unacceptable toxicity of the other agents, this drug remains a satisfactory, tolerated, and efficient treatment.14 In case of involvement of the CNS during T brucei gambiense infection, either melarsoprol or eflornithine can be used with an evident safer drug profile for eflornithine. Indeed, treatment with melarsoprol is often accompanied with several adverse effects with the most serious one consisting in a potentially lethal encephalopathic reaction.14 Finally, avoiding tsetse fly bites is quite illusory for overseas workers living in the well-known endemic focal areas. The flies are attracted to bright or contrasting colors and to the dust and motion of vehicles. They can bite through thin fabric. Longterm travelers or expatriates should use insect repellent, and wear wrist- and ankle-length clothing in neutral colors. Conclusions Human African trypanosomiasis should be suspected among patients presenting with cutaneous manifestations, lymphadenopathies, and fever and who live in a recognized endemic focal area. Prompt diagnosis of infection, mainly before the onset of CNS involvement, should be established as this form of the disease may be related to easy cure within a convenient therapeutic approach. Declaration of Interests The authors state they have no conflicts of interest. References 1. Ryan TE, Wilson ME, Kain KC. Illness after international travel. N Engl J Med 2002; 347: 505–516. 2. Donofrio LM, Millikan LE. Dermatologic diseases of eastern Africa. Dermatol Clin 1994; 12: 621–628. 3. Lucchina LC, Wilson ME, Drake LA. Dermatology and the recently returned traveller: infectious diseases with dermatologic manifestations. Int J Dermatol 1997; 36:167–181. 4. Iborra C, Danis M, Bricaire F, Caumes E. A traveller returning from Central Africa with fever and skin lesion. Clin Infect Dis 1999; 679–680. 5. Duggan AJ, Hutchinson MP. Sleeping sickness in Europeans: a review of 109 cases. J Trop Med Hyg 1966; 69:124–131. 6. Spencer HC Jr, Gibson JJ, Brodsky RE, Schultz MG. Imported African trypanosomiasis in the United States. Ann Intern Med 1978; 82:633–638. 7. Jelinek T, Bisoffi Z, Bonazzi L, et al. Cluster of African trypanosomiasis in travellers to Tanzanian national parks. Emerg Infect Dis 2002; 8: 634–635. 8. Malvy D, Djossou F, Weill FX, et al. Human WestAfrican trypanosomiasis with chancre presentation. Eur J Dermatol 2000; 10:761–762. 9. McGovern TW, Williams W, Fitzpatrick JE, et al. Cutaneous manifestations of African trypanosomiasis. Arch Dermatol 1995; 131:1178–1182. 10. Hoffner RJ, Slaven E, Perez J, et al. Emergency department presentations of thyphoid fever. J Emerg Med 2000; 19:317–321. 11. Caumes E, Carriere J, Guermonprez G, et al. Dermatoses associated with travel to tropical countries: a prospective study of the diagnosis and management J Travel Med 2007; 14: 192–196 196 of 269 patients presenting to a tropical disease unit. Clin Infect Dis 1995; 20:542–548. 12. Miezan TW, Meda HA, Doua F, et al. Assessment of central nervous system involvement in gambiense trypanosomiasis: value of the cerebrospinal white cell count. Trop Med Int Health 1998; 3:571–575. J Travel Med 2007; 14: 192–196 Ezzedine et al. 13. Lejon V, Büshner P. Cerebrospinal fluid in human African trypanosomiasis: a key to diagnosis, therapeutic decision and post-treatment follow-up. Trop Med Int Health 2005; 10:395–403. 14. Pepin J, Milord F. The treatment of human African trypanosomiasis. Adv Parasitol 1994; 33:1–47.