Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
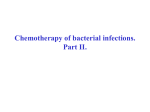
MAJOR ARTICLE Treatment Outcomes for Serious Infections Caused by Methicillin-Resistant Staphylococcus aureus with Reduced Vancomycin Susceptibility Benjamin P. Howden,1 Peter B. Ward,1 Patrick G. P. Charles,1 Tony M. Korman,2 Andrew Fuller,3 Philipp du Cros,3 Elizabeth A. Grabsch,1 Sally A. Roberts,9 Jenny Robson,8 Kerry Read,10 Narin Bak,4 James Hurley,7 Paul D. R. Johnson,1,5 Arthur J. Morris,9 Barrie C. Mayall,1 and M. Lindsay Grayson1,5,6 1 Departments of Infectious Diseases and Microbiology, Austin Health, 2Department of Infectious Diseases, Southern Health, 3Department of Infectious Diseases, The Alfred Hospital, 4Western Health, 5Department of Medicine, University of Melbourne, 6Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, and 7Ballarat Health Services, Ballarat, and 8Sullivan Nicolaides Pathology, Brisbane, Australia; and 9Auckland District Health Board and 10North Shore Hospital, Auckland, New Zealand Although infections caused by methicillin-resistant Staphylococcus aureus with reduced vancomycin susceptibility (SA-RVS) have been reported from a number of countries, including Australia, the optimal therapy is unknown. We reviewed the clinical features, therapy, and outcome of 25 patients with serious infections due to SA-RVS in Australia and New Zealand. Eight patients had endocarditis, 9 had bacteremia associated with deep-seated infection, 6 had osteomyelitis or septic arthritis, and 2 had empyema. All patients had received vancomycin before the isolation of SA-RVS, and glycopeptide treatment had failed for 19 patients (76%). Twenty-one patients subsequently received active treatment, which was effective for 16 patients (76%). Eighteen patients received linezolid, which was effective in 14 (78%), including 4 patients with endocarditis. Twelve patients received a combination of rifampicin and fusidic acid. Surgical intervention was required for 15 patients (60%). Antibiotic therapy, especially linezolid with or without rifampicin and fusidic acid, in conjunction with surgical debulking is effective therapy for the majority of patients with serious infections (including endocarditis) caused by SA-RVS. Nosocomial infections due to methicillin-resistant Staphylococcus aureus (MRSA) are an increasing problem in many parts of the world, including in Australia [1]. The therapeutic options available to treat serious infections due to MRSA are limited. The emergence of MRSA strains with reduced vancomycin susceptibility (SA-RVS) further reduces treatment options. Initially, the clinical significance of heterogeneous vancomycin– Received 7 August 2003; accepted 11 October 2003; electronically published 29 January 2004. Presented in part: 43rd Interscience Conference on Antimicrobial Agents and Chemotherapy, Chicago, Illinois, 14–17 September 2003 (abstract K-1750). Reprints and correspondence: Dr. Benjamin Howden, Department of Microbiology, Austin Hospital, Locked Bag 25, Heidelberg, Victoria, Australia, 3084 ([email protected]). Clinical Infectious Diseases 2004; 38:521–8 2004 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2004/3804-0009$15.00 intermediate S. aureus (hVISA) strains was debated, but they have now been clearly associated with glycopeptide treatment failure [2–7], as well as with higher in-hospital patient mortality rates than MRSA [8]. Serious clinical infections with SA-RVS—both vancomycinintermediate S. aureus (VISA) and hVISA—have now been reported in many countries, yet treatment efficacy has not been systematically assessed [9–11]. The laboratory confirmation of SA-RVS remains problematic and time-consuming, with the population analysis profile (PAP) being considered the current reference standard test [12]. After our initial report [11], we developed a protocol incorporating PAP testing for the investigation of possible SA-RVS isolates. Many isolates from across Australasia have since been referred to our department for testing. To assess the clinical features and treatment outcomes of patients with serious infections due to SA-RVS, we systematically reTreatment of SA-RVS • CID 2004:38 (15 February) • 521 viewed data for all patients whose referred sterile site isolates were confirmed to be SA-RVS in our laboratory. PATIENTS, MATERIALS, AND METHODS Ascertainment and review of patients. All patients with a sterile site isolate confirmed as SA-RVS (see laboratory methods and susceptibility definitions below) whose isolate was referred to our laboratory during the period of 1 May 2001 through 31 January 2003 were eligible for inclusion in this study. A questionnaire was sent to the referring clinician to obtain the patient’s demographic characteristics and data on comorbidities, risk factors for infection, infection, treatment, and outcome. Clinical definitions. “Glycopeptide failure” was defined as a blood culture positive for S. aureus after ⭓7 days of glycopeptide therapy or as a sterile site isolate positive for S. aureus after ⭓21 days of glycopeptide therapy. The type of infection was accepted as that reported by the treating clinician. However, a diagnosis of osteomyelitis required consistent nuclear or radiographic image (e.g., technetium bone scan or MRI) findings and/or histological confirmation, and a diagnosis of endocarditis was required to meet recognized criteria [13]. “Cure” was defined as no clinical or laboratory evidence of infection after the completion of antimicrobial therapy; furthermore, the patient had to be alive at follow-up. “Effective suppression” was defined as no clinical or laboratory evidence of active infection while receiving suppressive oral antimicrobial therapy. “Effective therapy” was defined as cure or effective suppression; patients who were apparently cured but who died of another cause during the follow-up period were also considered to have received effective therapy. “Relapse” was defined as additional sterile site isolate(s) that tested positive for SARVS or MRSA either after cessation of the antimicrobial therapy that had initially lead to clearance of infection or during receipt of appropriate therapy. Because patient outcomes were assessed in May 2003, the duration of follow-up varied on the basis of the date of initial diagnosis of SA-RVS infection. Laboratory methods and susceptibility definitions. The identification of all isolates as S. aureus was confirmed using standard methods [14]. The MIC of vancomycin was determined using the broth microdilution method for all isolates, in accordance with NCCLS recommendations [15], using cation-adjusted Mueller-Hinton broth. Susceptibility tests for linezolid, quinupristin-dalfopristin, and oxacillin were performed using the Etest (AB Biodisk), in accordance with the manufacturer’s instructions. Testing of all other antimicrobial susceptibility was performed using agar dilution, in accordance with NCCLS criteria [15]. Population analysis profile testing and calculation of the area under the curve (AUC) of test strains and an Mu3 control (ATCC 700698) were performed as described elsewhere [12]. 522 • CID 2004:38 (15 February) • Howden et al. The ratio of the AUC of the test isolate to that of the Mu3 control (PAP/AUC ratio) was calculated. SA-RVS was defined as an isolate of S. aureus with a PAP/AUC ratio of ⭓0.9 [12]. PFGE and riboprinting. Riboprint patterns were obtained using the RiboPrinter Microbial Characterisation System (Qualicon) with EcoR1 digestion. The riboprint pattern was determined using a combination of visual and computerassisted analysis. PFGE was performed on all isolates using methods described elsewhere, with some modifications [16]. For PFGE, strains were considered to be indistinguishable if there was no difference in bands, and they were considered to be related (i.e., subtypes of the same PFGE subtype) if they varied by 1–3 bands. A PFGE dendogram was constructed using GelCompar II (Applied Maths) to calculate similarity coefficients and to perform unweighted pair group analysis using arithmetic mean clustering. Dice coefficient with 0.5% optimization and 1.0% position tolerance was used. Three isolates from each of the 2 major PFGE groups found were referred to another laboratory for comparison, by PFGE analysis, with reference epidemic MRSA strains currently circulating in Australia and New Zealand. RESULTS Clinical treatment questionnaires were completed for 25 (89%) of the 28 patients who had a referred sterile site isolate confirmed to be SA-RVS at our laboratory during the study period. Patient demographics and risk factors for infection are presented in table 1. Twenty-three patients had a previously documented MRSA infection, but all 25 patients had received glycopeptide therapy at some time before the diagnosis of SA-RVS. The source of the SA-RVS infection was determined in 18 cases (surgical wound infection, 12 [67%] of 18; central intravenous line infection, 2 [11%]; diabetic foot infection, 2 [11%]; biliary stent infection, 1 [6%]; catheter related urinary tract infection, 1 [6%]). Data on 5 patients (patients 1, 2, 6, 9, 14; table 2) had been briefly reported in a previous publication by our group [17], but because this report did not include the patients’ treatment and outcome data, they were further described in this study. All patients had serious infections caused by SA-RVS (table 2), including 17 patients with bacteremia (endocarditis, 8 patients; osteomyelitis and/or septic arthritis, 4; intra-abdominal or biliary sepsis, 2; pacemaker abscess, 1; other, 2). Six patients had osteomyelitis and/or septic arthritis (including 3 patients with prosthetic joint infection) without bacteremia, and 2 patients had postsurgical empyema. Prolonged bacteremia while receiving vancomycin therapy was common among patients with endocarditis (median duration of bacteremia, 13 days; range, 7–32 days) and among those with osteomyelitis and/or septic arthritis (median duration of bacteremia, 9.5 days; range, Table 1. Demographic characteristics of and risk factors for 25 patients infected with Staphylococcus aureus with reduced vancomycin susceptibility (SA-RVS). Characteristic Value Ratio of men to women 16:9 Age, median years (range) 65 (45–83) MRSA infection before SA-RVS 23 Median time from initial diagnosis of MRSA infection to SA-RVS detection (range) 22 days (3 days– 31 months) Duration of glycopeptide therapy during the 6 months before SA-RVS detection, median days (range) 15 (0–91) Predose vancomycin serum level of !10 mg/mL in the first week of therapy 16 a Risk factor Diabetes 8 Immunosuppression 7 Malignancy 6 End-stage renal failure 3 Surgery !8 weeks before SA-RVS detection 18 Hospital location at time of diagnosis of SA-RVS infection ICU 9 Medical ward 7 Surgical ward 8 Outpatient 1 NOTE. Data are no. of patients, unless otherwise indicated. ICU, intensive care unit. a Data are for only 20 patients with SA-RVS infection who had vancomycin levels assessed during the first week of glycopeptide therapy. 5–33 days). Glycopeptide therapy failed for 19 (76%) of 25 patients, 15 of whom had detectable S. aureus bacteremia after 7 days of glycopeptide therapy, and 4 of whom had S. aureus isolated from a sterile site after 21 days of glycopeptide therapy. The PAP/AUC ratio range was 0.9–1.87, and the MIC of vancomycin (determined using the broth microdilution method) was 2–4 mg/L for all isolates (table 2). Although all isolates were susceptible to linezolid and quinupristin-dalfopristin, resistance and intermediate susceptibility were common for multiple other antibiotics, as follows: 100% of the isolates were resistant to oxacillin and to trimethoprim-sulfamethoxazole, 96% were resistant and 4% had intermediate susceptibility to tetracycline, 88% were resistant and 8% had intermediate susceptibility to erythromycin, 88% were resistant to gentamicin, 88% were resistant to ciprofloxacin, 36% were resistant to rifampicin, 8% were resistant to fusidic acid, and 4% were resistant to chloramphenicol. Notably, resistance to rifampicin developed during initial therapy for bacteremia in 3 cases (2 cases were being treated with vancomycin and rifampin, and 1 case was being treated with vancomycin, rifampicin, and fusidic acid). PFGE demonstrated 7 groups, with the majority of isolates being in 2 main groups (figure 1). There were 3 riboprint patterns, with most isolates in 2 groups. There was only limited correlation between the riboprint pattern and PFGE group. Although a number of isolates were found to be identical by PFGE, they had generally been isolated from different hospitals or at different times, indicating that cross-transmission was unlikely to be responsible for the similarities. Isolates from PFGE groups E and G were found, by comparison with reference strains, to be AUS2 and AUS3 epidemic MRSA, the most common multidrug-resistant strain of MRSA found in Australian hospitals, especially those in eastern Australia [18]. Twenty-one of the 25 patients received active antibiotic therapy to treat their SA-RVS infection, and 4 patients (patients 15, 16, 17, and 22; table 2) received either no therapy or minimal therapy directed at their SA-RVS infection. Three patients (patients 15–17) died before or soon after the SA-RVS infection was recognized. A fourth patient (patient 22) with a past history of multiple antibiotic-related adverse reactions and complications who had infected bilateral total hip prostheses was considered to have no treatment options except complete surgical removal of the infected prostheses, but this was refused by the patient. A number of antibiotic combinations were used by the 21 actively treated patients, but treatment with linezolid was most common (n p 18), either alone (n p 9) or sequentially with other agents, especially rifampicin and fusidic acid (n p 8). For Treatment of SA-RVS • CID 2004:38 (15 February) • 523 Table 2. Details of disease and treatment in patients infected with Staphylococcus aureus with reduced vancomycin susceptibility (SA-RVS). Patient Age in years/sex Type (site) of infection Underlying disease or risk factor Duration of positive blood culture results during glycopeptide therapy, days MIC of a vancomycin, mg/L 1 80/M Endocarditis (TV) Diabetes mellitus, Wegner granulomatosis, ESRF, immunosuppression, IVC filter 29 4 2 66/F Endocarditis (TV), PPM, IVC filter Diabetes mellitus, IHD, PPM, recent IVC filter 19 2 3 73/M Endocarditis (MV) Retroperitoneal fibrosis, steroid therapy, recent laparotomy 8 2 4 73/F Endocarditis (TV), vertebral OM, epidural, psoas, splenic abscesses Bowel carcinoma, steroid therapy 8 4 5 66/F Endocarditis (MV) Diabetes mellitus, cervical carcinoma, steroid therapy, aortic stenosis 13 4 6 72/M Endocarditis (prosthetic AV) Inflammatory arthritis, steroid therapy, AVR, MVR, PPM, recent open cholecystectomy 7 2 7 77/F Endocarditis (AV), splenic, renal abscess Diabetes mellitus, AS, MR, recent small bowel resection for polyps 20 2 8 67/M Endocarditis (prosthetic AV), mediastinitis Diabetes mellitus, recent AVR 32 2 9 45/M Bacteremia, spinal OM, spinal wound infection Automobile accident, paraplegic, recent thoracic fusion 12 4 10 46/F Bacteremia, extensive OM (foot), stump infection Diabetes mellitus, ESRF, PVD 5 2 11 63/M Bacteremia, SA (knee), vertebral OM, epidural abscess Diabetes mellitus, recent knee reconstruction and posttrauma ORIF 33 4 12 80/M Bacteremia, SA (shoulder, THR, TKR) RA, steroid therapy, THR, TKR 7 2 13 50/F Bacteremia, intraabdominal collections PVD, recent AAA graft and small bowel resection 1 2 14 55/F Bacteremia, biliary stent, liver abscess Cholangiocarcinoma, chemotherapy, recent biliary stent 15 2 15 83/M Bacteremia, PPM abscess PPM, AVR, colonic cancer, recent hemicolectomy 8 4 16 56/F Bacteremia Diverticular disease, recent hemicolectomy 1 4 17 64/F Bacteremia, pneumonia, meningitis Removal of pituitary adenoma, CSF leak 1 2 18 60/M OM (1st metatarsal), abscess (foot) Diabetes mellitus, PVD … 2 19 69/M SA (prosthetic knee joint) TKR … 2 20 70/M SA, OM (shoulder) Fall, recent arthroscopy of shoulder … 2 21 52/F OM, SA (tibia/knee) ORIF of tibial fracture … 4 22 66/M Bilateral SA, OM (THR) Bilateral THR … 2 23 63/M OM, SA (first MTPJ) ESRF, renal transplantation … 2 24 62/M Empyema Dermoid tumor in chest wall, recent thoracotomy … 4 25 59/M Empyema, pneumonia Lung cancer, recent lobectomy … 4 NOTE. AAA, abdominal aortic aneurysm; AUC, area under the curve; AV, aortic valve; AVR, aortic valve replacement; CCF, congestive cardiac failure; ESRF, end-stage renal failure; IVC, inferior vena cava; MTPJ, metatarsophalyngeal joint; MV, mitral valve; OM, osteomyelitis; ORIF, open reduction internal fixation; PAP, population analysis profile; PPM, permanent pacemaker; PVD, peripheral vascular disease; SA, septic arthritis; THR, total hip replacement; TKR, total knee replacement; TV, tricuspid valve. a Determined using the broth microdilution method. cases in which linezolid was used in combination with other antibiotics, linezolid monotherapy was usually given until the infection was clinically controlled (range, 17–78 days), followed by an alternative regimen (usually rifampicin with fusidic acid) either to complete a defined treatment course or for long-term 524 • CID 2004:38 (15 February) • Howden et al. suppression. One patient (patient 12; table 2) was treated with fusidic acid and chloramphenicol after initial control of the infection with linezolid, because the infection was resistant to rifampicin and all other available agents. Of note, 1 patient with osteomyelitis and septic arthritis of the first metatarso- PAP/AUC ratio Antibiotic therapy (duration) Treatment outcome Other interventions Overall outcome Comments 1.43 Linezolid (40 days) None Effective therapy Cured Follow-up duration of 10 months 1.14 Rifampin plus fusidic acid (11 days), then linezolid (38 days) TV vegetectomy, removal of PPM and IVC filter Effective therapy Cured Follow-up duration of 10 weeks 1.01 Linezolid (49 days) None Effective therapy Cured Follow-up duration of 3 months 1.77 Linezolid (42 days), then rifampin plus fusidic acid (8 days) None Effective therapy Died Died of comorbidities; culture results were negative after linezolid therapy 1.40 Linezolid plus rifampin and fusidic acid (12 days) MV repair Not effective Died Died of cardiac failure; culture results were negative after linezolid therapy 0.91 Rifampin plus fusidic acid (12 days) None Not effective Died Active therapy ceased after cerebral embolus 1.14 Rifampin (9 days), then linezolid (7 days) None Not effective Died Died of severe sepsis, CCF; culture results were positive after linezolid therapy 0.90 Linezolid (42 days) Redo AVR with homograft 10 days after linezolid therapy was stopped Not effective Died Died of postoperative bleeding; further positive blood culture results after linezolid therapy was ceased 1.36 Linezolid (32 days), then rifampin plus fusidic acid to suppression Laminectomy, wound debridement Effective suppression Clinically healthy Follow-up duration of 10 months 0.95 Linezolid (60 days) Above-knee amputation Effective therapy Cured Follow-up duration of 1 month 1.34 Rifampin plus fusidic acid (10 months) to suppression Multiple washouts, cervical and tho-racic laminectomies Effective suppression Clinically healthy Follow-up duration of 7 months 0.93 Linezolid (31 days), then fusidic acid and chloramphenicol long term None Relapse Clinically healthy Relapse of SA-RVS bacteremia while receiving fusidic acid and chloramphenicol; resolved 1.12 Linezolid (17 days), then rifampin plus fusidic acid (14 days) None Effective therapy Died Died of bacteremia due to gram-negative organisms; no further SA-RVS detected 1.17 Linezolid (34 days), then rifampin plus fusidic acid (14 days) Multiple drainages Effective therapy Died Died of cancer; no further SA-RVS detected 1.38 Rifampin plus fusidic acid (1 day) PPM explanted N/A Died Died of overwhelming sepsis 1.87 None None N/A Died Died of overwhelming sepsis 0.93 None None N/A Died Died of overwhelming sepsis 0.95 Linezolid (42 days) Abscess drainage Effective therapy Cured Follow-up duration of 4 months 1.22 Linezolid (78 days), then rifampin plus fusidic acid Removal of prosthetic knee Effective suppression Clinically healthy Received suppressive therapy; followup duration of 10 months 1.15 Linezolid (63 days) Shoulder washout Effective therapy Cured Follow-up duration of 5 months 1.10 Linezolid (28 days) Removal of plates and screws Effective therapy Cured Follow-up duration of 69 days 1.14 None Removal of THR N/A Chronic infected Chronic low-grade infection of left THR 0.91 Vancomycin (77 days) None Effective therapy Cured Follow-up duration of 6 months 1.28 Linezolid (56 days) Drainage of empyema Effective therapy Cured Follow-up duration of 2 weeks 1.07 Linezolid (42 days) Decortication Effective therapy Cured Follow-up duration of 4 months phalangeal joint (patient 23; table 2) was treated (and cured) with 11 weeks of vancomycin therapy because the managing clinicians were unaware that the infection was due to SA-RVS. Although this isolate fulfilled the definition of SA-RVS (PAP/ AUC ratio, 0.91), the clinical course was such that no additional isolates were recovered for testing. In the actively treated group (n p 21 ), 16 patients (76%) had an effective response to therapy. Ten patients (48%; patients 1–3, 10, 18, 20, 21, and 23–25) were cured at follow-up (table 2), 3 (14%; patients 9, 11, and 19) received effective suppressive therapy (table 2), and an additional 3 (14%; patients 4, 13, and 14), although they were apparently cured of infection, had died Treatment of SA-RVS • CID 2004:38 (15 February) • 525 Figure 1. PFGE analysis of 25 Staphylococcus aureus isolates with reduced vancomycin susceptibility. A, Alfred Hospital (Australia); B, Ballarat Health Services (Australia); M, Monash Medical Centre (Australia); N, Auckland District Health Board (New Zealand); O, North Shore Hospital (New Zealand); Q, Sullivan Nicolaides Pathology (Australia); R, Royal Melbourne Hospital (Australia); U, Austin Health (Australia); W, Western Hospital (Australia). of their underlying diseases at the time of follow-up (table 2). The length of follow-up for these effectively treated patients is described in table 2. SA-RVS infection clearly contributed to the death of an additional 4 patients. Thus, 7 patients (33%) had died at follow-up. The sole patient who experienced relapse (patient 12; table 2) had a good response to linezolid for multifocal prosthetic joint septic arthritis, but his clinical condition deteriorated, with a single additional blood culture positive for MRSA 4 months after treatment was changed to long-term suppressive therapy with fusidic acid and chloramphenicol. Despite the fact that the patient remained on fusidic acid and chloramphenicol, the results of 4 additional sets of blood cultures were negative, and the patient eventually stabilized. He was clinically healthy 2 months later while receiving suppressive therapy. Among the 18 patients who received linezolid therapy, the duration of linezolid treatment varied (range, 7–78 days) but was generally prolonged (median, 41 days). Side effects while receiving linezolid occurred in 8 patients and included thrombocytopenia (n p 5), abnormal liver function test values (n p 1), nausea (n p 1), and taste disturbance (n p 1 ). In 3 patients, the platelet count decreased to !50 ⫻ 10 9 platelets/L, with 1 patient requiring a platelet transfusion. All 3 patients had endocarditis and developed thrombocytopenia after ⭓35 days of therapy. Two patients (patients 2 and 4; table 2) com- 526 • CID 2004:38 (15 February) • Howden et al. pleted their course of linezolid therapy despite having platelet counts of 40 ⫻ 10 9 and 46 ⫻ 10 9 platelets/L, respectively, with no further decrease in the platelet count. One patient (patient 1; table 2), whose platelet count decreased to 7 ⫻ 10 9 platelets/ L, stopped taking linezolid therapy 2 days early, and no alternate therapy was used. The other 2 patients who developed mild thrombocytopenia continued to receive linezolid therapy. Surgery was an important component of therapy for 13 patients in the actively treated group, including 69% of patients for whom therapy was effective. Of the 13 actively treated patients who underwent surgery, 11 (85%) received effective therapy, whereas, of those who did not undergo surgery, 5 (63%) of 8 received effective therapy. The surgery usually involved significant debulking of infection (e.g., vegetectomy, debridement and removal of infected prosthetic devices, and drainage of multiple liver abscesses), and, in some cases, repeated surgery was required. DISCUSSION We found that serious infections due to SA-RVS in Australasia were generally identified in patients in whom glycopeptide treatment had failed. This correlates with previous reports of treatment failure in patients infected with these SA-RVS strains [4, 7, 8]. Nevertheless, the vast majority of these patients were effectively treated with antibiotics, either alone (31%) or in combination with surgical debulking of the infected site (69%). Linezolid was the most commonly used antibiotic, particularly for initial therapy, followed, in some patients (n p 5), by a switch to combination therapy with rifampicin and fusidic acid. Overall, adverse reactions were uncommon, except for thrombocytopenia in patients receiving prolonged courses of linezolid. These results are encouraging, given the serious nature of the infections we observed and the high rate of complex comorbidities in these patients. In particular, our relative success in treating endocarditis due to SA-RVS (therapy was effective for 4 of 8 patients) is notable, given that there is only a single previous reported case of successful treatment of SARVS endocarditis [19]. However, the fact that the remaining 4 patients with endocarditis died of complications (2 had ongoing bacteremia, despite receiving linezolid therapy) highlights the difficulties associated with this disease. Overall, in our study, linezolid appeared to be a relatively safe and effective agent, as long as therapy was not prolonged. All patients in this study had a clinical course that was consistent with infection with a staphylococcal strain that had reduced susceptibility to vancomycin. Nevertheless, these isolates highlighted the difficulty in readily detecting such vancomycin resistance in vitro, given that all strains initially demonstrated an MIC of vancomycin in the susceptible range (⭐4 mg/L), with a number of strains (n p 15) having an MIC of vancomycin of only 2 mg/L. Thus, studies that use the criteria of an MIC of vancomycin of ⭓4 mg/L or growth on media containing vancomycin, 4 mg/L, as diagnostic for SA-RVS [8, 20] may overlook such strains as ours and not proceed to PAP testing. However, as 1 patient (patient 23) in our study demonstrated, even PAP findings do not always correlate with clinical outcome. The SA-RVS strain isolated from patient 23 had a PAP/AUC ratio of 0.91 (i.e., just above the cutoff for SARVS) and an MIC of vancomycin of 2 mg/L (as determined using the broth microdilution method), yet the infection was apparently eradicated and the patient cured after receiving an 11-week treatment course of vancomycin. There are a number of potential explanations for the outcome in this case. First, given that the patient had end-stage renal failure and reduced vancomycin clearance, serum and bone vancomycin concentrations may have been substantially higher than in patients with more normal renal function. Second, the proportion of this patient’s S. aureus population with reduced susceptibility to vancomycin may have been sufficiently low that the combination of high vancomycin levels and the patient’s routine immune function may have been sufficient to eradicate resistant subpopulations. The mechanisms of vancomycin resistance in S. aureus are not known, although a thickened cell wall is a common feature, and this appears to be inducible by vancomycin [10, 21]. Consistent with this observation, most of our patients not only had previous MRSA infection and glycopeptide exposure, but 80% of those with recorded vancomycin levels had a low (!10 mg/ L) trough concentration during the first week of vancomycin therapy. Low vancomycin levels, particularly in the early stages of therapy, could result in induction of preexisting low-level vancomycin resistance or could select for new vancomycinresistant strains [10]. This clearly has implications in terms of the emphasis placed on surgical drainage and debulking of high–bacterial load infections in such patients (e.g., MRSAassociated abscesses and infected prostheses) and possibly has implications on vancomycin dosing. Whenever possible, MRSA-associated abscesses should be drained and a high priority given to removal of infected prosthetic devices. Molecular assessment of our SA-RVS isolates indicated a number of PFGE groups, with no substantive evidence of clonal dissemination. Isolates that appeared to be clonal were generally not epidemiologically linked—either by institution or time. Nevertheless, the fact that PFGE analysis suggested that some strains were closely related to the AUS2 and AUS3 MRSA strains that are the most common multidrug-resistant MRSA strains found in Australia [18] is concerning and highlights the potential for MRSA strains with reduced susceptibility to vancomycin to become widespread in Australia. Our study has some limitations. First, it is not possible, given the methodology of our case detection, to identify the correct clinical sequence in our patients—namely, whether our patients’ infections were ineffectively treated with glycopeptides with reduced susceptibility to vancomycin, thereby being induced and resulting in greater glycopeptide failure; or whether SA-RVS strains were primarily responsible for the infection all along, and glycopeptide failure was an inevitable consequence. Second, given the size and descriptive nature of our study, we cannot be certain about the efficacy of agents such as linezolid and rifampicin plus fusidic acid. However, our results are encouraging, especially if a combined medical and surgical approach is taken. Our study suggests that SA-RVS is not just a laboratory phenomenon, but that such strains are associated with serious infections that respond to carefully targeted nonglycopeptide therapy. With the increasing recognition of SA-RVS, future controlled studies comparing the efficacy of therapeutic agents should be performed. Acknowledgment We thank Geoff Coombs (Royal Perth Hospital; Perth, Australia), for performing PFGE typing of selected isolates, and the Treatment of SA-RVS • CID 2004:38 (15 February) • 527 microbiology and clinical staff from each of the hospitals that contributed cases. References 1. Turnidge JD, Nimmo GR, Francis G. Evolution of resistance in Staphylococcus aureus in Australian teaching hospitals. Med J Aust 1996; 164:68–71. 2. Turner J, Howe RA, Wootton M, et al. The activity of vancomycin against heterogeneous vancomycin-intermediate methicillin-resistant Staphylococcus aureus explored using an in vitro pharmacokinetic model. J Antimicrob Chemother 2001; 48:727–30. 3. Tenover FC, Biddle JW, Lancaster MV. Increasing resistance to vancomycin and other glycopeptides in Staphylococcus aureus. Emerg Infect Dis 2001; 7:327–32. 4. Hiramatsu K, Aritaka N, Hanaki H, et al. Dissemination in Japanese hospitals of strains of Staphylococcus aureus heterogeneously resistant to vancomycin. Lancet 1997; 350:1670–3. 5. Geisel R, Schmitz FJ, Thomas L, et al. Emergence of heterogeneous intermediate vancomycin resistance in Staphylococcus aureus isolates in the Dusseldorf area. J Antimicrob Chemother 1999; 43:846–8. 6. Fridkin SK. Vancomycin-intermediate and -resistant Staphylococcus aureus: what the infectious disease specialist needs to know. Clin Infect Dis 2001; 32:108–15. 7. Ariza J, Pujol M, Cabo J, et al. Vancomycin in surgical infections due to methicillin-resistant Staphylococcus aureus with heterogeneous resistance to vancomycin. Lancet 1999; 353:1587–8. 8. Fridkin SK, Hageman J, McDougal LK, et al. Epidemiological and microbiological characterization of infections caused by Staphylococcus aureus with reduced susceptibility to vancomycin, United States, 1997–2001. Clin Infect Dis 2003; 36:429–39. 9. Hiramatsu, K, Hanaki H, Ino T, Yabuta K, Oguri T, Tenover FC. Methicillin-resistant Staphylococcus aureus clinical strain with reduced vancomycin susceptibility. J Antimicrob Chemother 1997; 40:135–6. 10. Hiramatsu K. Vancomycin-resistant Staphylococcus aureus: a new model of antibiotic resistance. Lancet Infect Dis 2001; 1:147–55. 11. Ward PB, Johnson PD, Grabsch EA, Mayall BC, Grayson ML. Treat- 528 • CID 2004:38 (15 February) • Howden et al. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. ment failure due to methicillin-resistant Staphylococcus aureus (MRSA) with reduced susceptibility to vancomycin. Med J Aust 2001; 175:480–3. Wootton M, Howe RA, Hillman R, Walsh TR, Bennett PM, MacGowan AP. A modified population analysis profile (PAP) method to detect heteroresistance to vancomycin in Staphylococcus aureus in a UK hospital. J Antimicrob Chemother 2001; 47:399–403. Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis 2000; 30:633–8. Kloos WE, Banerman TL. Staphylococcus and Micrococcus. In: Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of clinical microbiology. 7th ed. Washington, DC: American Society for Microbiology Press, 1999:264–82. NCCLS. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. NCCLS document M7-A5. Wayne, PA: NCCLS, 2000. Murchan S, Kaufmann ME, Deplano A, et al. Harmonization of pulsedfield gel electrophoresis protocols for epidemiological typing of strains of methicillin-resistant Staphylococcus aureus: a single approach developed by consensus in 10 European laboratories and its application for tracing the spread of related strains. J Clin Microbiol 2003; 41: 1574–85. Charles PGP, Ward PB, Johnson PDR, Howden BP, Grayson ML. Clinical features associated with bacteremia due to heterogeneous vancomycin-intermediate Staphylococcus aureus. Clin Infect Dis 2004; 38: 448–51. Coombs GW, Malkowski MJ, Pearson JC, Bell JM, Nimmo GR. Epidemic MRSA in Australia [abstract 203-02]. Australian Group for Antimicrobial Resistance. In: Program and abstracts of the 10th International Symposium on Staphylococci and Staphylococcal Infections, Japan. Tokyo: Japanese Association for Infectious Diseases, 2002:97. Andrade-Baiocchi S, Tognim MC, Baiocchi OC, Sader HS. Endocarditis due to glycopeptide-intermediate Staphylococcus aureus: case report and strain characterization. Diagn Microbiol Infect Dis 2003; 45:149–52. Schwaber MJ, Wright SB, Carmeli Y, et al. Clinical implications of varying degrees of vancomycin susceptibility in methicillin-resistant Staphylococcus aureus bacteremia. Emerg Infect Dis 2003; 9:657–64. Srinivasan A, Dick JD, Perl TM. Vancomycin resistance in staphylococci. Clin Microbiol Rev 2002; 15:430–8.