Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
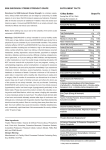
NUTRILYTE® NUTRILYTE® (Multi-Electrolyte Concentrate) (Multi-Electrolyte Concentrate) Rx Only Rx Only Not for direct infusion. For prescription compounding of intravenous admixtures only. Concentrated solution. Dilute to appropriate strength with suitable intravenous fluid prior to administration. DESCRIPTION: Nutrilyte (Multi-EIectrolyte Concentrate) is a sterile, nonpyrogenic, concentrated solution of intra- and extracellular electrolytes, excluding phosphate. No antimicrobial agent has been added. It is available in a 20 mL single dose preparation and a 100 mL Pharmacy Bulk Package. The 100 mL Pharmacy Bulk Package contains many doses for use in a pharmacy admixture program in the preparation of parenteral fluids. See directions for dispensing from the 100 mL Pharmacy Bulk Package. Electrolytes (mEq): per mL per 20 mL Acetate 2.03 40.6 Potassium 2.03 40.6 Chloride 1.68 33.6 Sodium 1.25 25 Magnesium 0.40 8 Calcium 0.25 5 Gluconate 0.25 5 Nutrilyte Contains per mL per 20 mL Sodium Acetate •3H2O, USP 135 mg 2.7 grams Potassium Chloride, USP 125 mg 2.5 grams Sodium Gluconate 55 mg 1.1 grams Magnesium Acetate •4H2O 43 mg 0.86 gram Potassium Acetate, USP 34.5 mg 0.69 gram 22 mg 0.44 gram Calcium Acetate •H2O Water for Injection, USP q.s. q.s. pH (6.3 to 7.0) adjusted with Glacial Acetic Acid when necessary. Calculated Osmolarity: Approximately 7562 mOsmol/Liter; 7.562 mOsmol/ mL. CLINICAL PHARMACOLOGY Nutrilyte Concentrate provides a source of intra- and extracellular electrolytes in suitable amounts, to help maintain normal cellular metabolism during total parenteral nutrition (TPN) and other parenteral therapy in adults. Use of properly diluted Nutrilyte meets most adult daily electrolyte requirements and provides adjunctive therapy for replenishment of depleted electrolyte stores. Intracellular: Potassium, the principal intracellular cation, maintains the integrity of the cellular membrane, helps transport dextrose across the cell membrane and contributes to normal renal function: Magnesium, the second most concentrated intracellular cation, acts as an important cofactor in enzymatic reactions and helps to maintain normal central nervous system activity and amino acid utilization. Calcium participates in the maintenance of normal neuromuscular functions and blood coagulation. Extracellular: Chloride, the primary extracellular anion, contributes to the maintenance of acid-base balance. Sodium, the principal extracellular cation, acts in conjunction with potassium to maintain integrity of the cell membrane. Sodium also helps to maintain motor nerve depolarization, normal renal metabolism and fluid balance. Acetate is a bicarbonate alternate and an important intermediate in the tricarboxylic acid cycle. INDICATIONS AND USAGE Nutrilyte Concentrate is indicated for use as a supplement to parenteral nutritional solutions containing amino acids, dextrose and/or other calorie sources delivered by central venous or peripheral infusion to facilitate amino acid utilization and maintain electrolyte balance in adults. Nutrilyte Concentrate is also indicated as a source of replacement electrolytes for the depleted adult patient during parenteral therapy. CONTRAINDICATIONS Nutrilyte Concentrate is contraindicated in clinical conditions where additives of potassium, sodium, calcium, magnesium or chloride could be clinically detrimental. Such conditions include anuria, hyperkalemia, heart block or myocardial damage and edema due to cardiovascular, renal or hepatic failure. Nutrilyte Concentrate is not intended for pediatric use. Use only if solution is clear and seal intact. WARNINGS 1. Strongly hypertonic solutions. Must be properly diluted and thoroughly mixed before injection. 2. Contains no phosphate. Patients receiving TPN solutions containing concentrated dextrose may also require phosphate in addition to Nutrilyte. It is necessary to take into consideration the calcium and magnesium ions in this solution in order to avoid precipitation where phosphate is present in the diluted solution. Phosphate (10-15 mEq/L), calcium (5 mEq/L) and magnesium (5-10 mEq/L) rarely are incompatible when properly mixed. Higher levels must be added cautiously with adequate mixing (avoid layering) and inspection. Additional calcium and phosphate may be added to alternate bottles. If additional phosphate is required, it is essential to consider the salt form because of pre-existing levels of potassium and the final concentration of phosphate in the infusate. 3. Each 20 mL of Nutrilyte contains 40.5 mEq of potassium. Patient requirements should be carefully evaluated prior to the addition of any potassium salt to a solution containing Nutrilyte. 4. This product contains aluminum that may be toxic. Aluminum may reach toxic levels with prolonged parenteral administration if kidney function is impaired. Premature neonates are particularly at risk because their kidneys are immature, and they require large amounts of calcium and phosphate solutions, which contain aluminum. Research indicates that patients with impaired kidney function, including premature neonates, who receive parenteral levels of aluminum at greater than 4 to 5 mcg/kg/day accumulate aluminum at levels associated with central nervous system and bone toxicity. Tissue loading may occur at even lower rates of administration. NUTRILYTE® NUTRILYTE® (Multi-Electrolyte Concentrate) (Multi-Electrolyte Concentrate) Rx Only Rx Only PRECAUTIONS 1. To minimize the risk of possible incompatibilities arising from mixing this solution with other additives that may be prescribed, the final infusate should be inspected for cloudiness or precipitation immediately after mixing, prior to administration and periodically during administration. 2. Blood levels of sodium, potassium, calcium, magnesium, phosphorus and chloride should be monitored frequently during parenteral nutrition or intravenous therapy, and the daily dosage of electrolytes may require tailoring to meet individual needs. In tissue electrolyte depletion, addition of certain electrolytes may be required to meet individual patient needs. 3. Care must be exercised administering solutions containing up to 30 mEq of sodium and 40 mEq of potassium per liter to patients with renal or cardiovascular insufficiency, particularly if they are postoperative or elderly. Sodium-containing solutions should be administered with caution to patients receiving corticosteroids or corticotropin or to other salt-retaining patients. Potassium replacement therapy may be guided by serial electrocardiograms since plasma levels are not necessarily indicative of tissue potassium levels. 4. Administration of barbiturates, narcotics or hypnotics should be adjusted with caution in patients also receiving magnesium-containing solutions because of an additive central depressive effect. 5. Parenteral magnesium and/or calcium and/or potassium should be administered with extreme caution to patients receiving digitalis preparations. 6. Extraordinary electrolyte and fluid losses are not necessarily corrected by infusion of solutions containing Nutrilyte. In order to avoid deficits, special consideration must be given to replacement of excessive fluid and electrolyte losses in such conditions as protracted vomiting or diarrhea, nasogastric suction or fistula drainage. 7. If both phosphate and a Nutrilyte Concentrate are to be added to the solution for TPN administration, add the Nutrilyte Concentrate to one container (either to the amino acids or the concentrated dextrose) and add the phosphate to the other to avoid physical incompatibilities between calcium and phosphorus. ADVERSE REACTIONS Symptoms may result from an excess or deficit of one or more of the ions present in Nutrilyte Multi-Electrolyte Concentrate. Therefore, frequent monitoring of blood electrolyte levels is essential. Sodium excess can cause edema and subsequent congestive heart failure in patients with cardiovascular insufficiency. Potassium excess can cause an abnormal electrocardiogram, cardiac arrhythmias leading to cardiac arrest, paresthesias and flaccid paralysis, mental confusion and weakness. Potassium deficit can impair neuromuscular function and cause intestinal dilatation and ileus. Magnesium excess can cause muscular weakness, flushing, sweating, hypotension, circulatory collapse and depression of cardiac and central nervous system function. Magnesium deficiency can cause hyperirritability, psychotic behavior, tachycardia, hypertension and neuromuscular dysfunction. Calcium excess can cause depression, headaches, drowsiness, disorientation, syncope, dysphagia, hypotonia of skeletal and smooth muscles, arrhythmias and coma. Calcium deficits can produce neuromuscular hyperexcitabilty (paresthesias, cramps, tetany and grand mal seizures). Phosphorus deficiency may lead to impaired tissue oxygenation and acute hemolytic anemia. Relative to calcium, excessive phosphorus intake can precipitate hypocalcemia with ensuing neuromuscular hyperexcitabilty. DOSAGE AND ADMINISTRATION For adults, one 20 mL dose of Nutrilyte should be added to each liter of amino acid/dextrose solution (TPN) or other suitable intravenous solution. Route: Nutrilyte Concentrate is for prescription compounding of intravenous admixtures only. The solution is strongly hypertonic. Not for direct patient injection. Dilute to appropriate strength with suitable intravenous fluid prior to administration. DIRECTIONS FOR DISPENSING FROM 100 mL PHARMACY BULK PACKAGE—NOT FOR DIRECT INFUSION The 100 mL Pharmacy Bulk Package is for use in a Pharmacy Admixture Service only. The 100 mL Pharmacy Bulk Package should be suspended (inverted) by its IV hang label in a laminar flow hood or biological safety cabinet. Prior to entering a Pharmacy Bulk Package, remove the flip-off seal and cleanse the rubber closure with a suitable antiseptic agent. Entry into the Pharmacy Bulk Package must be made with a sterile transfer set or other sterile dispensing device and the contents dispensed in aliquots using aseptic technique. Use of a syringe needle is not recommended as it may cause leakage. ANY UNUSED PORTION MUST BE DISCARDED WITHIN 4 HOURS AFTER INITIAL ENTRY. The date and the time initially opened should be recorded in the space provided on the Pharmacy Bulk Package label. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. HOW SUPPLIED: Nutrilyte® (Multi-Electrolyte Concentrate) NDC 0517-3120-25 20 mL Single Dose Vial For preparing 1 Liter TPN Solution. Boxes of 25 NDC 0517-3100-25 100 mL Pharmacy Bulk Package Boxes of 25 Store at 20° to 25°C (68° to 77°F); excursions permitted to 15° to 30°C (59° to 86°F) (See USP Controlled Room Temperature). IN3100 Rev. 1/09 MG #15000 AMERICAN REGENT, INC. SHIRLEY, NY 11967