Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
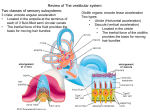
Results: OPKs -- 20deg/sec: Normal gain -- 40deg/sec: Symmetrical but reduced gain in both directions CALORIC TESTING Wait a second…..we’re not done yet! ICE CALORIC Results • Brief, low-velocity (4 deg/sec), right-beating nystagmus • Extinguished quickly & did not reverse upon patient’s movement to sitting • Suggests possible presence of residual high-frequency vestibular function in the left ear – Not considered definitive: Short response duration Failure to reverse with a change in position Moo. That’s Right! Image retrieved from: http://pureluxury.com VNG Results Summary -- Left caloric weakness -- Right-beating component of post-headshake nystagmus Left peripheral vestibular lesion. -- Oblique (down beating) component of post-headshake nystagmus -- Prolonged saccadic latencies -- Reduced gain in smooth pursuit testing -- Reduced gain in OPK testing at 40deg/sec Central vestibular dysfunction? --Effect of centrally acting medications & neurological conditions (Parkinson’s/TIA) is unknown Left Peripheral Vestibular Lesion What Pathology is Responsible? Unilateral Weakness + Unilateral Hearing Loss Vestibular Labyrinthitis • Labyrinthitis is an inflammation of the inner ear and vestibular and auditory portion of the 8th nerve. Viral- caused by a viral infection Bacterial-caused by a bacterial infection Image taken from: vestibulopathy.com • Infection of the inner ear or 8th nerve as a whole that causes a vestibular imbalance, vertigo and hearing loss. (Maire & Melle, 2004) Viral Labyrinthitis Symptoms • Usually unilateral • Very sudden onset – During the day. – Upon awakening in the morning • Vestibular symptoms: – Can be mild or severe • Auditory symptoms: – Sudden SSNHL (usually unilateral) • Tinnitus (Vestibular Disorders Association (VEDA), 2011) Common Diagnostic Findings • Audiometric Testing: – Asymmetric hearing loss involving the affected ear – Differential Diagnosis! • Caloric Testing: – Decreased response in the affected ear Possible: • Gaze Nystagmus • Spontaneous Nystagmus – Horizontal and beating away from affected ear (Maire & Melle, 2004) & (Hain, 2010) Treatment: 3 Parts • Part I Treat the Infection – Steroids (Prednisone) Anti-inflammatory – Antiviral Drugs (Acyclovir) Herpes infections – Antibiotics (Amoxicillin) Bacterial infections • Part II Treat the Symptoms – Antivert (Meclizine) Symptoms of vertigo – Benadryl (Antihistamine) Motion sickness – Ativan (lorazepam) Valium (diazepam) Anxiety • Part III: Vestibular and Aural Rehabilitation Why No Spontaneous Nystagmus? • The patient’s initial episode of vertigo was in January 2012 • Seen for VNG in March 2012 • After a severe peripheral lesion, nystagmus intensity declines rapidly as days pass due to… CNS COMPENSATION! (Jacobson & Shepard, 2008) Types of Compensation • Compensation Goal: Reset the VOR so that it can respond accurately to head movements • Static: The cerebellum uses the intact labyrinth as a reference point to reset the level of activity of vestibular nuclei on the impaired side – Eliminates spontaneous nystagmus – Asymmetry no longer perceived without head movement • Dynamic: Helps to restore the normal gain asymmetry that occurs with head movement – Eliminates oscillopsia – Reduces complaints of dizziness with head movement (Jacobson & Shepard, 2008) Types of Compensation • VNG testing revealed no spontaneous nystagmus – Static compensation complete • Patient complaint of imbalance exacerbated with head movement consistent with postheadshake nystagmus – Dynamic compensation incomplete! Patient Prognosis What do we anticipate for the patient’s balance moving forward? Patient Prognosis • Residual high frequency vestibular function better prognosis in rehabilitation • Moderate to strong evidence that vestibular rehabilitation (VR) is a safe, effective management for unilateral peripheral vestibular dysfunction (UPVD) – Provides a resolution to symptoms in the medium term • Exercise based interventions containing balance and strength training exercises effectively reduced falls (Telian et al, 1991), (Hiller & McDonnell, 2011) & (Gillespie et al, 2010) Impairments • Visual System – Cataracts – Glaucoma – Legally blind in left eye • Peripheral Vestibular System – Unilateral peripheral vestibular weakness • Somatosensory System – Arthritis – Peripheral Neuropathy (left foot) – Right lower leg amputation – Parkinson’s Disease Realistic Expectations Patient was counseled on realistic expectations given that the three inputs to balance are impaired • Our patient also experiences: – Anxiety – Depression Realistic Expectations • Patients with UPVD who demonstrate the greatestmagnitude self-report of disability/handicap also demonstrate concominant impairments of supporting senses • The magnitude of psychological comorbid conditions is predictive of self-reported dizziness handicap • Decreased balance confidence is associated with actual balance performance, duration of vestibular symptoms, general health related quality of life, and treatment for anxiety, depression or both, and visual impairments (Jacobson, 2002), (Piker et al, 2008) & (Marchetti et al, 2011) Realistic Expectations • The Dizziness Handicap Inventory (DHI) was developed to evaluate the self-perceived handicapping effects imposed by vestibular system disease • Three content domains representing aspects of dizziness – Functional – Emotional – Physical • Our patient has a DHI of 52 indicating a moderate/ borderline severe self-perceived handicap – 16-34 (mild) – 36-52 (moderate) – 54+ (severe) (Jacobsen & Newman, 1990) Moving Forward… • Single Sided-Deafness: – Not interested in audiologic intervention No CROS No BAHA • Permanent Unilateral Weakness: – Continue with PT with emphasis on vestibular rehabilitation & fall prevention. • Follow up with ENT/Neurotology consult. • If additional information needed: consider rotary chair testing • Patient JK has not followed up at this time References: Gillespie, L. D., Robertson, M. C., Gillespie, W. J., Lamb, S. E., Gates, S., Cumming, R. G., et al. (2010). Interventions for preventing falls in older people living in the community. The Cochrane Library (10). Hain, T.C. (2010). Labyrinthitis case. Retrieved from http://www.dizziness-andbalance.com/disorders/unilat/case%20labyrinthitis.html Hain, T.C. (2010). Vestibular neuritis and labyrinthitis. Retrieved from http:// www.dizziness-and-balance.com/disorders/unilat/vneurit.html Hiller, S.L., McDonnel, M.(2011).Vestibular Rehabilitation for Unilateral Peripheral Vestibular Dysfunction. Cochrane Database of Systemic Reviews, Issue 2. Art. No.: CD005397. DOI: 10.1002/14651858.CD005397.pub3. Jacobsen G.P. (2002). Development of a clinic for the assessment of risk of falls in the elderly. Seminars in Hearing, 23; 161-178. Jacobsen, G.P. & Newman , C.W..(1990). The development of the dizziness handicap inventory. Arch Otolaryngological Head Neck Surgery. 116(4); 424-427. References: Maire,R.& Melle, G.V. (2004). Horizontal Vestibulo-Ocular Reflex Dynamics in Acute Vestibular Neuritis and Viral Labyrinthitis:evidence of Otoloth-Canal Interation. Acta Otolaryngol, 124, 36-40. Marchetti, G.F., Whitney, S.L., Redfern, M.S., Furman, J.M. (2011). Factors Associated With Balance Confidence in Older Adults With Health Conditions Affecting the Balance and Vestibular System. Arch Physical and Mental Rehabilitation, 92; 1884-91. Piker, E. G., Jacobson, G.P., McCaslin, D.L., Grantham, S.L. (2008). Psychological comorbidities and their relationship to self-reported handicap in samples of dizzy patients. Journal of the American Academy of Audiology. 19; 337-347. Telian, S.A., Shepard, N.T., Smith-Wheelock, M., Hoberg, M. (1991). Bilateral vestibular paresis: diagnosis and treatment. Official Journal of Otolaryngology -Head & Neck Surgery, 104(1); 67-71. Vestibular Disorders Association (VEDA). (2011). Labyrinthitis and vestibular neuritis Retrieved from http://www.vestibular.org/vestibular-disorders/specificdisorders/labyrinthitisvest-neuritis.php