Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
(CANCER RESEARCH 51. 1680-1683. March 15. I991|
Effect of Hyperthermia on Normal Tissue Toxicity and on Adriamycin
Pharmacokinetics in Dogs
A. V. Wilke, C. Jenkins, A. J. Milligan, A. Legendre, and D. L. Frazier1
College of I 'eterinary Medicine, Departments of Environmental Practice ¡A.y. W., D. L. F.J anil L'rban Practice /('. J., A. J. M., A. L.), university of Tennessee,
Knoxrille. Tennessee Ì790I-I07I
ABSTRACT
MATERIALS AND METHODS
This study examined the effects of Adriamycin (ADR) (30 mg/m2),
whole-body hyperthermia (\VBII) (42 ( for 1 h), and the combination of
the two (ADR plus \\ HII) on gastrointestinal and hematopoietic toxicity
and the effects of VVBI1on ADR pharmacokinetics in the normal dog
(n = > treatment group).
Duodenal biopsies were collected from animals in each group via
endoscopy and were incubated in the presence of | '1l|ili> miilim- as an
Adult pure-bred beagle dogs of both sexes (Marshall Farms, North
Rose, NY) were divided into three treatment groups (n = 5): ADR,2 i.v.
Adriamycin-HCl (Adria Labs, Columbus, OH) at 30 mg/m2; WBH,
whole-body hyperthermia at 42°Cfor 1 h; and ADR plus WBH, 42°C
index of cell turnover. Additional duodenal biopsies were assayed for the
enzymes 7-glutamyltranspeptidase, /V-acetyl-j8-i>-glucosaminidase, and
succinate dehydrogenase. Complete blood chemistry profiles and differ
ential blood cell counts were done prior to and following treatment. Cell
turnover was most depressed 3 days after ADR or ADR plus WBH;
\YBII alone had little effect on cell turnover. Neither 7-glutamyltrans
peptidase, /V-acetyl-iS-D-glucosaminidase, nor succinate dehydrogenase
activities were significantly altered by any of the treatment protocols.
High performance liquid Chromatograph) was used to quantify Adri
amycin and adriamycinol in samples collected up to 6 h after drug
administration. Duodenal biopsies were collected immediately and I h
after drug administration for measurement of tissue concentrations of
Adriamycin. A significant increase in the apparent volume of distribution
and whole-body clearance and decrease in area under the plasma Adria
mycin concentration versus time curve occurred when drug was adminis
tered concurrently with YVBII.This differs from results reported in some
other mammalian species.
INTRODUCTION
Hyperthermia has been shown to potentiate cytotoxicity of
several antitumor drugs, including the anthraeycline antibiotic
Adriamycin (1-3). At the cellular level, hyperthermic conditions
lead to an increased influx of Adriamycin into cells and in
creased cell kill (4). The in vivo situation is clearly more com
plex, because it includes additional factors; most notably, drug
delivery to a given tissue must be considered.
Milligan et al. (5) reported that whole-body hyperthermia
increased blood flow to the gastrointestinal tract, heart, and
pancreas. The phenomenon of increased drug delivery to the
gastrointestinal tract is supported by a report of bloody diarrhea
in dogs after concurrent whole-body hyperthermia and Adria
mycin (6). Other studies have reported nonuniform drug deliv
ery with concurrent whole-body hyperthermia (7).
The purpose of this study was to determine whether wholebody hyperthermia altered the pharmacokinetics of Adriamycin
and whether the concurrent administration of whole-body hy
perthermia and Adriamycin increased gastrointestinal toxicity.
Received 9/25/90; accepted 1/9/91.
The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement in
accordance with 18 L'.S.C. Section 1734 solely to indicate this fact.
1To whom requests for reprints should be addressed, at College of Veterinary
Medicine. Department of Environmental Practice. University of Tennessee. P.O.
Box 1071. Knoxville. TN 37901-1071.
2The abbreviations used arc: ADR. Adriamycin; WBH, whole-body hyperilu-i HIM.HPLC, high performance liquid chromalography: AUC. area under the
plasma concentration versus time curve: ADR-OL, adriamycinol; G(JT. i-glutamyltranspeptidase;
NAG. ,V-acetyl-ci-D-glucosaminidase; SDH. succinyl
dehydrogenase.
hyperthermia for 1 h, with Adriamycin administered when rectal tem
perature reached 42°C.Thirty mg/m2 ADR is the standard clinical dose
for canine patients (8); higher doses (50-60 mg/m2) are often used in
humans (9-11) but are not tolerated by dogs. Dogs were fasted over
night before treatment but were given free access to water. In all groups,
dogs were premedicated with butorphanol (0.4 mg/lb), diazepam (0.2
mg/lb), and atropine (0.04 g/lb); anesthesia was mask-induced and
maintained with isoflurane. WBH (42°C)was induced in appropriate
groups with a thermal blanket that utilized recirculating heated water.
Temperature was monitored using a Bailey TM-10A with internal
calibration and i.p., i.m., and rectal thermocouples (one probe/site).
Rectal temperature was used as the primary indicator for monitoring
purposes; approximately 1 h was needed to raise rectal temperature to
42°C.
Adriamycin Pharmacokinetics. In the ADR and ADR plus WBH
groups, venous blood (3 ml) was collected immediately, at 15, 30, and
45 min and at 1, 2, 4, and 6 h after Adriamycin administration.
Duodenal biopsies were collected via endoscopy immediately after and
1 h after drug administration, for measurement of ADR tissue concen
trations. All samples were placed on ice immediately, blood was then
centrifuged, and the plasma and biopsies were stored at —20°C
until
analysis.
Plasma extraction of ADR and its metabolites was carried out using
a modification of the method of Robert (12). Briefly, daunomycin was
added as internal standard to I ml plasma, and the sample was purified
using C-18 Sep-Pak minicolumns (Waters Assoc., Milford, MA), with
phosphate buffer and methanol. Duodenal biopsies were homogenized
with a Dounce tissue grinder in 1 ml phosphate buffer and then treated
like plasma (13).
The HPLC system consisted of a ^-Bondapak phenyl (10-cm x 80mm) column protected by a CN-type Guardpak (Waters Associates)
column. The mobile phase consisted of a gradient of 0.1% ammonium
formate (pH 4.0) and acetonitrile. Fluorescence of the eluate was
monitored with excitation at 480 nm and emission at 550 nm (Waters
model 470 detector).
Pharmacokinetic parameters were determined using an automated
curve-stripping program followed by a SAS-based nonlinear regression
program. Calculation of parameters shown in Table 1 was as follows:
C'fO= extrapolated drug concentration in the central compartment
at time = 0
(•„
= dose/C^
Kfó= dose/fi- AUC, where fi is the slope of the elimination phasee
V¿m= dose/K- AUC, where K is the first-order elimination
rate constant
CL = dose/AUC
I'.;.,= In 2/«,where H is the slope of the distribution phase
/vin= In 2//ÃŽ,
where ß
is the slope of the elimination phase
AUC was calculated by the trapezoidal method (14). Vjt, Vdf, and
K/„.represent volumes of distribution of the central compartment.
1680
Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1991 American Association for Cancer Research.
ADRIAMYCIN PHARMACOKINETICS
Table 1 Pharmacokinetic parameters describing the disposition ofAdriamycin in
normal dogs, with and without concurrent whole-body hyperthermia (42" C)
10
ADR
-ADR
- - ADR-OL
WBH
BH-2.76
+ \V
ADR
ADR-OL
0.99011.3
+
A
(/jg/ml)a
(h-1)B
1.080.1+
(Mg/ml)P
±0.0520.730
12
Or1)('„,
150.281±0.2
(liter/kg)K,tf
±0.05915.9
(liter/kg)K/„„
±4.294.55+
1.250.065
(liter/kg)''/,„
(h)'»„
0.0061.34
±
(h)C7.
±0.4139.8
5.305.94+
+
(ml/kg/min)CP()
1.010.648
(/Jg/ml)AUC(Mg/m|.h)ADR"5.82
0.1
0.01
0.001
0.0001
100
200
300
TIME, m
elimination phase, and area, respectively. CL is the whole-body clear
ance; i./,oand t:/,sare the half-lives in the distribution and elimination
phases, respectively.
Statistical comparison of these parameters was performed using the
Wilcoxon test (SAS, Cary, NC).
Cell Turnover. Duodenal biopsies were collected via endoscopy prior
to treatment and at the following times after treatment: 1 h, 3 days,
and 7 days. Six biopsies were collected at each time and placed in
polypropylene microcentrifuge tubes (two biopsies/tube) containing 1
ml ice-cold Krebs-Ringer bicarbonate/glucose buffer. Procaine penicil
lin G (2000 units/ml), dihydrostreptomycin (0.25 mg/ml), and gentamicin (0.05 mg/ml) were added to eliminate bacterial growth. [3H]Thymidine (0.5 ¿iCi;ICN Biomedicals, Costa Mesa, CA) was added,
and the open vials were placed in a 37°Cwater bath for 1 h. The
atmosphere of the bath was maintained at 5% COV95% Ch.
At the end of the incubation, DNA was extracted with perchloric
acid and quantified with diphenylamine, as described by Leyva and
Kelley (15). ['H]Thymidine uptake was quantified by mixing aliquots
of the acid extract with Pico-Flor 40 (Packard, Downers Grove, IL)
and counting (Packard liquid scintillation analyzer model 1500).
Histopathology. Duodenal biopsies were collected for histopathological examination prior to treatment and on day 3 following treatment.
Biopsies were fixed in neutral buffered formalin prior to sectioning,
hemotoxylin-eosin staining, and light microscopic examination.
Enzyme Assays. Duodenal biopsies were collected prior to treatment
and on day 3 following treatment, for assay of GGT, NAG, and SDH.
These assays were performed according to the micromethods developed
by Andersen et al. (16). When necessary, multiple biopsies for a given
time were combined to give a sample size of at least 5 mg. Briefly,
ADR
— ADR + WBH
0.001
234
hr.
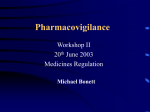
Fig. 2. Plasma Adriamycin concentration versus time curves generated from
pharmacokinetic data, using the formula
A and B are intercepts, a and >iare the slopes of the distribution and elimination
phases, respectively, and t is time since drug administration.
1.3515.0
±
±2.690.024
0.0020.339
+
0.0301.32
±
0.56953.7
+
5.39*23.1
±
±5.85*0.052
0.0072.09
±
53137.0
±0.1
42.3*2.78
+
1.350.236
±
+ 0.061*
±0.084ADR
' Treatment groups (n = 5 each); all values are mean ±SE.
' P < 0.05, Mann-Whitney.
400
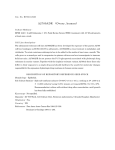
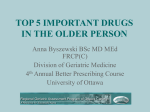
Fig. 1. Representative plots of actual ADR and ADR-OL plasma concentra
tions in dogs receiving drug alone (ADR) and drug with concurrent whole-body
hyperthermia (ADR plus WBH).
TIME,
WITH HYPF.RTHERMIA
samples were homogenized in 1 ml of ice-cold 0.15 M NaCl, pH 7.O.
with a Dounce tissue grinder (Wheaton, Millville, NJ). Protein concen
tration of this homogenate was determined using the Bio-Rad protein
assay (Bio-Rad, Richmond. CA). GGT and NAG assays consisted of
incubation of homogenate aliquots with the fluorescently labeled sub
strate analogs A/-7-glutamyl-<v-naphthylamide and 4-methylumbelliferyl-2-acetamido-2-deoxy-£i-r>-glucopyranoside, respectively. At 40
and 60 min for GGT and NAG. respectively, the reactions were stopped,
and liberated fluorescent label was quantified using a Perkin-Elmer
LS5B fluorometer. The SDH assay was based on reduction of piodonitrotetrazolium to its UV-absorbing form. p-Iodonitrotetrazolium-formazan was then extracted with ethyl acetate and quantified
using a Shimadzu UV-visible spectrophotometer (490 nm).
RESULTS
Pharmacokinetics. The HPLC system used in this study was
capable of separating daunomycin (internal standard), ADR,
and the metabolites of ADR, ADR-OL, ADR aglycone, and
ADR-OL aglycone. ADR-OL was the only metabolite detected
in significant quantities in the plasma; however, its appearance
varied between dogs. Whole-body hyperthermia decreased peak
plasma concentrations of ADR-OL [0.0126 ±0.0016 Mg/ml
(mean ±SE) versus 0.573 ±0.020 Mg/ml; P = 0.09]. Repre
sentative plasma concentration versus time profiles are shown
in Fig. 1. ADR aglycone and ADR-OL aglycone (both at <5
ng/ml) were seen in four animals (two ADR, two ADR plus
WBH). ADR aglycone was detected no later than 45 min after
drug administration in the ADR group and no later than 5 min
after drug administration in the ADR plus WBH group. ADROL aglycone was detected up to 30 min after drug administra
tion in the ADR group and up to 15 min after drug administra
tion in the ADR plus WBH group.
Plasma elimination of ADR was best described by a twocompartment model (Fig. 2) characterized by a rapid distribu
tion phase (t<A„
= 0.07 h) and a slower elimination phase (f,/1(j=
1.34 h). WBH induced significant changes in clearance (CL),
apparent volumes of distribution (Vdc, Vde, Vdmi), and AUC
(Table 1).
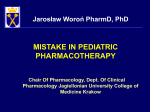
ADR concentrations in duodenal samples did not differ sig
nificantly between the two drug treatment groups. WBH caused
higher ADR concentrations initially, followed by more rapid
elimination of ADR from the duodenal epithelium (Fig. 3);
however, these differences were not statistically significant.
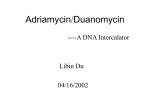
Cell Turnover. Cell turnover data showed considerable vari
ability. Although comparisons of mean cell turnover values, at
specific time points, to pretreatment control values were not
statistically significant, some trends were seen (Fig. 4). [1H]-
1681
Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1991 American Association for Cancer Research.
ADRIAMVCIN PHARMACOKINKTICS
Table 2 Enzvme activities of duodenal biopsies from normal dogs receiving ADR,
42°CWBH for 1 h, or both concurrently (ADR plus WBH)
108642
MEDIATE1IpnrnoNE
M
HOUR31I
Pinch biopsies were collected via endoscopy. Assays were performed using
either fluorescent-labeled substrate analogs (GGT. NAG) or spectrophotometric
methods (SDH).
GGT"(units/g)ADR*WBHADR
units/g)i.S\44232.13.17.64.38.93Â
±0.984
3PretreatmentDay
0.338±
0.269±
iPretreatmentDay
0.220±
0.880±0.130±
±I.27
.03
±1.23±1
+1
+WBHPretreatmcnt'Day
.32 ±0.0.0.0.0.0.160\05183113173187SDH(10~'
33.543.492.923.733.814.40±
0.338NAG(units/g)1.13
" Enzyme activities by treatment group were not significantly different (MannWhitney).
* Treatment groups («= 5 each); all values are mean ±SE.
' Biopsy collection time relative to treatment.
n¡255JI
Fig. 3. Adriamycin content of duodenal biopsies (mean ±SE: n = 5). Biopsies
were collected immediately after and l h after drug administration from dogs
receiving drug alone (ADR) or drug concurrent with 42°Chyperthermia (ADR
plus WBH).
Thymidine uptake in drug-containing groups (ADR, ADR plus
WBH) reached a maximum depression on day 3 following
treatment, whereas the WBH group values were most depressed
on the day of treatment. The two drug-containing groups had
similar responses; their absolute differences were probably due
to the higher pretreatment values of the ADR plus WBH group.
Histopathology and Clinical Parameters. Duodenal biopsies
from each treatment group were histopathologically normal.
Complete blood counts and chemistry panels were normal;
mean values within groups were never outside the clinically
normal range. Creatinine clearance was significantly reduced
on day 3, compared to pretreatment clearance (4.04 versus 2.67
ml/min-kg), in the ADR plus WBH group. Posttreatment
creatinine clearance was within normal limits for the ADR and
WBH treatment groups.
Enzyme Assays. Activities for the enzymes GGT, NAG, and
SDH were not statistically changed by the treatment protocols,
when day 3 samples were compared to pretreatment (Table 2).
Posttreatment GGT activity was increased slightly in the WBH
and ADR plus WBH treatment groups, whereas the ADR group
was relatively unchanged.
DISCUSSION
Altered plasma or tissue concentrations of Adriamycin or its
metabolites resulting from concurrent administration of wholebody hyperthermia may affect toxicity towards cancer cells as
well as normal tissues. Only Adriamycin and adriamycinol have
been previously described in the dog (17). In the present study,
the HPLC system used was capable of separating Adriamycin,
adriamycinol, and the respective aglycones. All four compounds
were detected in plasma; no metabolites were detected in duo
denal biopsies. The alcohol derivative of Adriamycin, ADROL, probably does not have significant antitumor activity but
has been implicated in Adriamycin-induced cardiotoxicity (18).
Increased cardiotoxicity in humans receiving concurrent wholebody hyperthermia and Adriamycin has been reported ( 19). The
present study did not examine the ADR-OL content of cardiac
tissues; however, our results indicate that peak ADR-OL
plasma concentrations were increased by hyperthermia.
This study demonstrated that whole-body hyperthermia al
tered the pharmacokinetics of Adriamycin in the normal dog.
Specifically, increases in the rate of drug distribution to tissue
and the volume of distribution of drug occurred. An increase in
whole-body clearance, a decrease in AUC, and a trend toward
decreased peak plasma concentration (CA))were noted. These
increases in tissue distribution did not seem to result in overt
toxicity to the duodenum. Although changes in other parame
ters were seen (e.g., B, ß,and K/r), these changes were not
statistically significant, probably due to small sample size and
variability within groups.
Various investigators have reported different results for Adri
amycin pharmacokinetics in response to whole-body hyperther
mia. Daly et al. (6) reported no change in mean Adriamycin
plasma concentrations during 43°Chyperthermia induced by
extracorporeal heating of blood in heparinized dogs. Animals
were given a dose (2 mg/kg) comparable to the dose used in the
present study, but spectrofluorometric methods were used and
pharmacokinetic parameters were not calculated for the four
animals used. Daly's study reported bloody diarrhea lasting for
7 days after treatment, which was attributed to increased drug
levels in the gastrointestinal tissues. Mimnaugh et al. (20)
reported that WBH affected only the initial rate of Adriamycin
distribution to tissues (fi..,J in rabbits and not the volume of
distribution. This conflicts with our finding of increased vol
umes of distribution of Adriamycin with concurrent hyperther
mia. Mimnaugh et al. also reported that whole-body hyperther
mia did not increase Adriamycin concentrations in tissue sam
ples (including duodenum) collected 60 min after treatment,
with the exception of cardiac muscle. Our finding of a tendency
toward decreased peak ADR plasma concentration (CAl) with
WBH also does not agree with Mimnaugh's significantly in
15
a.
WITH HYPERTHERM1A
10
o
>I
DAY
Fig. 4. [JH]Thymidine uptake by duodenal biopsies incubated for l h in the
presence of 0.5 M¿"¡
|'H]thymidine (mean ±SE: n = 5).
creased CPain heated rabbits. Cn, may be an important param
eter, in light of reports that peak Adriamycin concentrations
are directly related to incidence of toxicity (9, 21, 22). The
1682
Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1991 American Association for Cancer Research.
ADRIAMYCIN
PHARMACOKINETICS
results of the present study are similar to the changes in the
pharmacokinetic disposition of cisplatin when it is administered
concurrently with whole-body hyperthermia to dogs (7). The
differences in pharmacokinetics may be attributable to different
physiological responses to hyperthermia in the two species.
Ex vivo ['H]thymidine incorporation has been used to study
the effects of drugs on intestinal mucosa proliferarne activity
(23). In the present study, a single dose of Adriamycin decreased
proliferative activity in the duodenal mucosa for at least 2 days;
however, activity returned to normal by 1 week. A pilot study
evaluating cell turnover on days 1-7 showed maximum depres
sion of activity on day 3; therefore, dogs in this study were
biopsied only on days 1, 3, and 7, to minimize anesthesia and
trauma to the gastrointestinal tract. Whole-body hyperthermia
alone produced little change in the proliferative activity of
duodenal mucosa. The depression of proliferative activity seen
in the groups receiving Adriamycin can be attributed to the well
documented effects of Adriamycin on DNA replication systems
(24-27). The effects include inhibition of DNA topoisomerase
II and intercalation into DNA, both of which may interfere
with DNA replication. The variability in these data may be a
result of the inherent nonuniformity in biopsy size and depth.
Differences in the number of villus tips versus crypt cells could
be reflected in cell turnover rates. Additionally, ['Hjthymidine
incorporation in larger biopsies may have been limited by
diffusion of labeled thymidine into the entire biopsy.
The results of the enzyme assays indicated that the treatment
protocols significantly affected neither GGT, NAG, nor SDH
activities. These enzymes are brush border, lysosomal, and
mitochondrial enzymes, respectively (28). The activities of these
three enzymes have been shown to be altered by intestinal
disease (28). There seemed to be a slight induction of GGT in
the hyperthermic groups, which was not seen in the ADR group.
The reason for this enzyme induction is not clear.
Significant changes in complete blood counts and serum
chemistry parameters were not seen in the present study. These
parameters would more likely be changed with repeated drug
administration.
In conclusion, this study demonstrated that whole-body hy
perthermia increases the distribution of Adriamycin in the
normal dog. There is not, however, a uniform increase to all
tissues. It seems likely that blood flow to tumors in various
tissues would differ, just as it differs in various normal tissues.
Whether the pharmacokinetic changes seen would increase or
decrease Adriamycin concentrations in a spontaneous tumor
and the effect on tumor cell killing would likely depend on the
location of the tumor. Whole-body hyperthermia also increased
clearance of Adriamycin from plasma, which may be a result of
increased excretion as well as distribution. Since fractionated
hyperthermia protocols are often used clinically, the effects of
repeated heating on plasma and tissue pharmacokinetics and
toxicity should be examined. Additionally, because blood flow
patterns probably change during hyperthermia, the question of
pharmacokinetics after continuous infusion with concurrent
hyperthermia needs to be addressed.
REFERENCES
I. Hahn. G. M. Potential for therapy of drugs and hyperthermia.
39: 2264-2268. 1979.
Cancer Res..
WITH HVI'ERTHERMIA
2. Herman. S. H.. Sweets. C. C.. White, D. M.. and Gemer. E. \V. Effect of
heating on lethality due to hyperthermia and selected chemothcrapeutic
drugs. J. Nati. Cancer Inst.. 68: 487-491. 1982.
3. Herman, T. S. Temperature dependence of Adriamycin. c/.v-diamminechloroplatinum. bleomycin. and 1.3-bis(2-chloroethyl)-l-nitrosourea
cytotoxicity
in vitro. Cancer Res.. 43: 517-520, 1983.
4. Rice. G. C.. and Hahn. G. M. Modulation of Adriamycin transport by
hyperthermia as measured by fluorescence-activated cell sorting. Cancer
Chcmother. Pharmacol.. 20: 183-187, 1987.
5. Millii:.in A. J.. Petersen. I. A., and Ferrei. K. D. Changes in complete blood
count, blood chemistry and perfusion values during fractionated whole body
hyperthermia. Int. J. Radial. Oncol. Biol. Phys.. in press, 1991.
6. Daly. J. M., Wang, V. M.. Kapelanski. D.. and Frazier, O. H. Systemic
therrnochemotherapy: toxicity and plasma pharmacokinetics of methotrexate
and doxorubicin. J. Surg. Res.. 37: 343-347. 1984.
7. Riviere. J. E.. Page, R. L.. Rogers. R. A.. Change. S. K.. Dewhirst. M. W.,
and Thrall. D. E. Nonuniform alteration of ci'.v-diamniinedichloroplatinum
(II) tissue distribution in dogs with whole body hyperthermia. Cancer Res.,
50:2075-2080.
1990.
8. Ogilvie, Ci. K.. Richardson. R. C.. Curtis. C. R.. Withrow, S. J., Reynolds.
H. A., Norris, A. M., Henderson. R. A.. Klausner. J. S.. Fowler. J. D., and
McCaw, D. Acute and short-term toxicoses associated with the administra
tion of doxorubicin to dogs with malignant tumors. J. Am. Vet. Med. Assoc..
195: 1584-1587. 1989.
9. Speth. P. A. J.. Linssen. P. C. M.. Holdrinet. R. S. G., and Haanen. C.
Plasma and cellular Adriamycin concentrations in patients with myeloma
treated with ninety-six-hour continuous infusion. Clin. Pharmacol. Ther..
41: 661-665. 1987.
10. Gil. P., Favre. R.. Durand. A., Iliadis. A.. Cano. J. P.. and Carcassonne, Y.
Time
Adriamycin
and Adriamycinol kinetics. Cancer Chemother. dependency
Pharmaco'l.. of10:
120-T24. 1983.
11. Robert. J.. Bui, N. B.. and Vrignaud. P. Pharmacokinetics of doxorubicin in
sarcoma patients. Eur. J. Clin. Pharmacol.. 31: 695-699. 1987.
12. Robert, J. Extraction of anthracyclincs from biological fluids for HPLC
evaluation. J. Liquid Chromatogr...?: 1561-1572. 1980.
13. Cox. S. K.. Wilke, A. V., and Frazier. D. Determination of Adriamycin in
plasma and tissue biopsies. J. Chromatogr., in press. 1991.
14. Gibaldi. M., and Perrier. D. Estimation of areas. In: J. Swarbrick (ed.). Drugs
and the Pharmaceutical Sciences, Vol. 15. Pharmacokinetics. pp. 445-449.
New York: Marcel Dekker. Inc.. 1982.
15. Leyva. A., and Kelley. W. N. Measurement of DNA in cultured human cells.
Anal. Biochem.. 62: 173-179. 1974.
16. Andersen. K. J.. Schionsby. H.. and Skagcn. D. W. Enzyme activities in
human and ral jcjunal mucosa. Scand. J. Gastroenterol.. 18: 241-249. 1983.
17. Oosterbaan. M. J. M., Dirks. R. J. M., Vree. T. B.. and van der Kleijn. E.
Pharmacokinetics of anthracyclines in dogs: evidence for structure-related
bod\ distribution and reduction to their hydroxy metabolites. Pharm. Res..
35-39. 1984.
18. Olson. R. D.. Mushlin. P. S.. Brenner. D. E.. Fleischer. S.. Cusack. B. J.,
Chang. B. K.. and Boucek. R. J.. Jr. Doxorubicin cardiotoxicity
may be
caused by its metabolite, doxorubicinol.
Proc. Nati. Acad. Sci. USA. 85:
3585-3589.1988.
19. Kim. Y. D.. Lees. D. E., Lake. C. R., Whang-Peng. J.. Schuette, VV.. Smith,
R.. and Bull. J. Hyperthermia potentiates doxorubicin-related
cardiotoxic
effects. J. Am. Med. Assoc.. 241: 1816-1817. 1979.
20. Mimnaugh. E. G., Waring, R. W.. Sikic, B. I.. Magin. R. L.. Drew. R.,
Litters. C. L., Gram, T. E., and Guarino, A. M. Effect of whole body
hyperthermia on the disposition and metabolism of Adriamycin in rabbits.
Cancer Res.. 38: 1420-1425. 1978.
21. Legha. S. S., Benjamin. R. S.. Mackay. B.. el al. Reduction of doxorubicin
cardioloxicity by prolonged continuous intravenous infusion. Ann. Intern.
Med.. 96: 133-139. 1982.
22. Vogelzang. N. J. Continuous infusion chemotherapy: a critical review. J.
Clin. Oncol.. 2: 1289-1304. 1984.
23. Craven, P. A.. Thornburg. K.. and DeRubertis. F. R. Sustained increase in
the proliferation of rat colonie mucosa during chronic treatment with aspirin.
Gastroenterology. «4:567-575. 1988.
24. Bodley. A. L.. and Liu. L. F. Topoisomerases as novel targets for cancer
chemotherapy. Bio/technology, \ovemher: 1315-1319. 1988.
25. Tewey. K. M.. Rowe, T. C.. Yang, L., Halligan. B. D.. and Liu, L. F.
Adriamycin-induced DNA damage mediated by mammalian DNA topoisom
erase II. Science (Washington DC'). 226: 466-468. 1984.
26. Zwelling. L. A.. Michaels. S.. Erickson, L. C., Ungerleider. R. S.. Nichols.
M.. and Kohn. K. \V. Protein-associated deoxyribonucleic acid strand breaks
in LI210 cells treated with the deoxyribonucleic acid intercalating agents
4'(9-acridinylamino)methanesulfon-m-anisidide
and Adriamycin. Biochem
istry. 20: 6553-6563. 1981.
27. Chen. G. L.. and Liu. L. F. DNA topoisomerases as therapeutic targets in
cancer chemotherapy. Annu. Rep. Med. Chem.. 21: 257-262. 1986.
28. Andersen. K. J.. Schionsby. H.. and Skagen. D. W. Jejunal mucosal enzymes
in untreated and treated coeliac disease. Scand. J. Gastroenterol., 18: 251256. 1983.
1683
Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1991 American Association for Cancer Research.
Effect of Hyperthermia on Normal Tissue Toxicity and on
Adriamycin Pharmacokinetics in Dogs
A. V. Wilke, C. Jenkins, A. J. Milligan, et al.
Cancer Res 1991;51:1680-1683.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://cancerres.aacrjournals.org/content/51/6/1680
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from cancerres.aacrjournals.org on June 18, 2017. © 1991 American Association for Cancer Research.