Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cancer immunotherapy wikipedia , lookup
Immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Innate immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
DNA vaccination wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
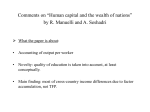
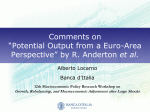
Genes and Immunity (2011) 12, 663–666 & 2011 Macmillan Publishers Limited All rights reserved 1466-4879/11 www.nature.com/gene SHORT COMMUNICATION A novel immunodeficiency disorder characterized by genetic amplification of interleukin 25 MR Green1,2, E Camilleri1, MK Gandhi2,3, J Peake4 and LR Griffiths1,2 Genomics Research Centre, Griffith Institute for Health and Medical Research, Griffith University, Gold Coast, Queensland, Australia; Griffith Medical Research College, A Joint Program of Griffith University and the Queensland Institute of Medical Research, QIMR, Herston, Queensland, Australia; 3Clinical Immunohaematology Laboratory, Queensland Institute of Medical Research, Herston, Queensland, Australia and 4Queensland Pediatric Immunology and Allergy Service, Royal Children’s Hospital, Herston, Queensland, Australia 1 2 Many primary immunodeficiency disorders of differing etiologies have been well characterized, and much understanding of immunological processes has been gained by investigating the mechanisms of disease. Here, we have used a wholegenome approach, employing single-nucleotide polymorphism and gene expression microarrays, to provide insight into the molecular etiology of a novel immunodeficiency disorder. Using DNA copy number profiling, we define a hyperploid region on 14q11.2 in the immunodeficiency case associated with the interleukin (IL)-25 locus. This alteration was associated with significantly heightened expression of IL25 following T-cell activation. An associated dominant type 2 helper T cell bias in the immunodeficiency case provides a mechanistic explanation for recurrence of infections by pathogens met by Th1-driven responses. Furthermore, this highlights the capacity of IL25 to alter normal human immune responses. Genes and Immunity (2011) 12, 663–666; doi:10.1038/gene.2011.50; published online 21 July 2011 Keywords: immunodeficiency; IL25; T-cell; Th1; Th2; copy number variation Introduction Primary immunodeficiency disorders affect approximately two people per 100 000, and predispose affected individuals to recurrent infections and the development of other disorders such as lymphomas.1,2 Primary immunodeficiency disorders range in both severity and etiology, but the majority result in a deficiency in antibody production. Many of these disorders have been well characterized and result from specific genetic defects that, in most cases, lead to the loss-of-function of central components of immune maturation or signaling.3 The profound effect on immune function by genetic defects is testament to the importance of specific components in maintaining immune homeostasis. The establishment of a type 1 (Th1) or type 2 (Th2) helper T-cell dominance is an important step in regulating the class of immune response mounted against pathogens (reviewed in Kidd4). Polarization of Th1 or Th2 subsets from non-committed naı̈ve T-cells is primarily driven by cytokine signals that are directed by the type of antigen encountered by immune cells. The most definitive base of information regarding cytokine-driven polarization of helper T-cells highlights interferon-g- and Correspondence: Professor LR Griffiths, Genomics Research Centre, Griffith Institute for Health and Medical Research, Griffith University, Gold Coast Campus, Queensland 4215, Australia. E-mail: [email protected] Received 16 March 2011; accepted 13 June 2011; published online 21 July 2011 interleukin (IL)-4mediated signaling as the drivers of Th1 and Th2 polarization, respectively. Signaling by these cytokines causes helper T-cell polarization by invoking broad transcriptional changes. In Th1 cells, these transcriptional changes are driven primarily by the transcription factor TBX21 (T-bet5), whereas in Th2 cells, they are primarily driven by the transcription factor GATA3.6,7 These transcription factors induce the expression of cytokines by Th1- or Th2-polarized cells that function as a positive feedback loop to promote further polarization of cells to the same subtype and inhibit polarization to the opposing subtype. The culmination of these events is a dominance of one helper T-cell state over the other and dichotomization of the class of immune response mounted against invading pathogens. In addition to the well-characterized interferon-g- and IL4-driven T-helper cell polarization mechanism, there is accumulating evidence for a role of other factors in regulating this axis. These include the Th1-associated cytokine IL12, the Th2-associated cytokine IL5, and more recently, a newly defined member of the IL17 family, IL25, has been shown to promote Th2 responses.8,9 Here, we describe the molecular characterization of a novel immunodeficiency disorder. This case shows profound combined immunodeficiency that manifested from an early age with recurrent Varicella infections, bronchitis, skin infections, upper respiratory tract infections and otitis media (For detailed case history, see Supplementary Information). No molecular alterations characteristic of currently defined immunodeficiency disorders were found, and the case tested negative for Primary immunodeficiency disorders MR Green et al 664 human immunodeficiency virus. We therefore utilized genome-wide DNA and transcriptional profiling, to define the etiology of the disorder. Results and discussion To define the molecular etiology of a novel immunodeficiency disorder, we utilized whole-genome high resolution DNA copy number analysis to elucidate potentially causative genetic alterations. Using this approach, we identified a tetraploid region at 14q11.2 that mapped over the IL25 gene, which has a role in promoting Th2 responses and thereby suppressing Th1 responses. By pairing genetic analysis with transcriptional profiling, we identified a large number of genes associated with Th1/Th2 profiles to be differentially expressed in peripheral blood lymphocytes of the case, including a significant enrichment of a GATA3 transcriptional signature, indicative of a Th2 bias that was also confirmed in the case by flow cytometric analysis. Single-nucleotide polymorphism (SNP) microarraybased platforms are an effective tool for gaining high resolution DNA copy number information, with extensive genome coverage.10 Because of the inability to define the etiology of this immunodeficiency syndrome based on molecular tests for known disorders (Conley et al.11 and Supplementary Information), we undertook a comprehensive screen for potentially etiologic DNA copy number alterations in the case genome with reference to 100 HapMap controls. This highlighted small, previously defined, naturally occurring copy number variations, as well as a larger tetraploid region at 14q11.2 (chr11:19,272,965-23,891,430; Figure 1a), which did not align to copy number variations previously identified in a large population of healthy control subjects.12 The presence of this alteration was confirmed by matrix assisted laser desorption/ionisation time of flight (MALDI-TOF) copy number analysis (Figure 1b) and encompassed the gene encoding IL25, a cytokine known to induce Th2 immune responses.8,9 In vitro analysis of IL25 gene expression in purified lymphocytes following T-cell activation found that this cytokine was expressed at levels 2.49-fold higher in case lymphocytes, compared with lymphocytes from control subjects (t-test P-value ¼ 0.001, Figure 1c). We therefore hypothesized that genetic amplification and overexpression of IL25 in this case may skew immunity towards Th2 responses and thereby result in insufficient Th1 immune responses. To provide further evidence towards this hypothesis, we utilized the genome-wide transcriptional profiling. Comparison of gene expression profiles from peripheral blood lymphocytes of the case and an age-, gender-, ethnicity-matched healthy control subject identified a Figure 1 Increased DNA copy number of IL25 results in overexpression following T-cell activation. (a) Genome-wide DNA copy number analysis was performed using Sty 250 K SNP arrays (Affymetrix, Santa Clara, CA, USA), on peripheral blood DNA from the case and three control subjects. Copy number was calculated as in Supplementary Materials, and identified a quadraploid region at 14q11.2 that mapped over the IL25 locus. (b) DNA copy number increase was confirmed by matrix assisted laser desorption/ionization time of flight (MALDITOF) mass spectrometry-based analysis of two markers within the hyperploid region (rs4562981 and rs6489721), compared with a control marker within the glyceraldehydes 3-phosphate dehydrogenase gene (rs6489721). The significantly larger area under the curve of the homozygous SNP rs4562981 and heterozygous SNP rs6489721 compared with the heterozygous control marker confirm hyperploidy of the candidate region. (c) Expression of IL25 was measured by quantitative PCR in purified peripheral blood lymphocyte cultures following T-cell activation, using anti-CD3 T-cell activation plates. Expression of IL25 in the case sample was found to be significantly (P ¼ 0.001) higher than that in an age-, gender-, ethnicity-matched healthy control subject. For detailed methods, refer to Supplementary Material. *Po0.05. Genes and Immunity Primary immunodeficiency disorders MR Green et al large number of differentially expressed genes. Among these were a large number of genes associated with Th1 or Th2 transcriptional profiles, which supported a decreased Th1 signature and increased Th2 signature (Figure 2a). This included 4.17-fold decreased expression of the Th1-associated gene TBX21, a central transcription factor driving Th1 polarization. Although the transcription factor responsible for driving Th2 polarization (GATA3) was not found to be significantly differentially expressed between case and control subjects by gene expression microarray analysis, the activity of this transcription factor may be modified by post-translational modifications that would not be detected at the transcript level.13 We therefore investigated GATA3 activity by gene set enrichment analysis (for detailed methods, refer to Supplementary Information) of the previously defined GATA3PATHWAY signature14,15 and found evidence that GATA3 activity is significantly enriched in case lymphocytes (enrichment score ¼ 0.512, P-value o0.001; Figure 2b). Additionally, the previously defined IL4PATHWAY and IL5PATHWAY signatures (http://www.broadinstitute.org/gsea/msigdb/index.jsp), which may also be considered suggestive of a Th2 bias, also showed enrichment in the immunodeficiency case (enrichment scores ¼ 0.549 and 0.620, respectively), but did not obtain statistical significance with robust multiple hypothesis testing correction. Finally, evidence for a Th2 bias within the immunodeficiency case was gained by flow cytometric analysis of lymphocyte populations, using the CD4 helper T-cell marker and intracellular staining for the Th1- or Th2-associated cytokines, interferon-g and IL4. Importantly, T-cell activation of healthy control subjects by anti-CD3 stimulation resulted in quantifiable populations of Th1 cells (data not shown). However, in the case subject, there was a profound absence of lymphocytes with a Th1 phenotype, but a clearly defined Th2 population (Figure 2c). This provided additional evidence towards a skewed Th2 dominance in the immunodeficiency case, which we posit is a direct result of genetic amplification of the IL25 locus. Several factors of the case history further substantiate a Th2 bias. Patients with profound immunodeficiency commonly suffer from recurrent infections by pathogens that are cleared by Th2-mediated responses, such as Pneumocystis carinii pneumonia or acid-fast bacteria,16,17 whereas there is no evidence of these infections within the case history of this novel disorder. In contrast, this patient suffered from recurrent infections by Varicella, Staphylococcus aureus and Pseudomonas aeruginosa, which are more effectively cleared by Th1 responses.18–20 An overactive Th2 response is also further supported by other features of the case history, including (i) occurrence idiopathic thrombocytopenia purpura at age 3 without relapse, which is consistent with a Th2 imbalance,21 (ii) the normal levels of IgE despite lymphopenia and deficiencies of other immunoglobulins, as an IgE isotype switch is supported by a Th2 response,22 and (iii) the normal proliferative response of lymphocytes to pokeweed, which elicits a Th2 response,23 but poor proliferative responses to all other mitogens. Together, these support our hypothesis that genetic amplification and resulting overexpression of IL25 drives a Th2 bias in this case and renders the subject susceptible to infections cleared by Th1 responses, in addition to other pathologies associated with overactive Th2 responses. In conclusion, this study not only shows the utility of whole-genome screens in defining the molecular basis for novel disorders, but also provides insight into a novel 665 Figure 2 IL25 amplification and overexpression is associated with a Th2 bias in the case. (a) Total RNA from peripheral blood of the case and matched control were profiled using HG U133 Plus2.0 microarrays (Affymetrix). A large number of genes associated with Th1/Th2 profiles were found to be differentially expressed in the case. Genes associated with a Th1 profile, including the Th1-associated transcription factor TBX21, were found to be downregulated, and genes associated with a Th2 profile were found to be upregulated. (b) Although GATA3 was not found to be differentially expressed between case and control subjects, gene set enrichment analysis of the GATA3PATHWAY signature found it to be significantly enriched in the case (enrichment score ¼ 0.512, Po0.001). (c) A Th2 skew was confirmed by cytoflow analysis, using the CD4 helper T-cell marker and intracellular staining for the Th1-associated cytokine, interferon-gg, or the Th2-associated cytokine, IL4. This showed that, following in vitro T-cell activation with anti-CD3, there were no detectable cells of a Th1 phenotype in the case, and the majority of CD4 þ cells showed intracellular expression of IL4, indicating they were of a Th2 phenotype and confirming a Th2 bias in the case. For detailed methods, see Supplementary Information. Genes and Immunity Primary immunodeficiency disorders MR Green et al 666 disorder that results from overexpression of IL25. This expands the current base of knowledge regarding pathologies associated with overactive Th2 responses and provides another example of how deregulation of a single immune component can have a profound effect on proper immune function. Conflict of interest The authors declare no conflict of interest. Acknowledgements We acknowledge the contribution of clinical immunologists that have provided their findings, including Prof Rebecca Buckley (Duke University Medical Centre, NC, USA), Dr Alison Jones (Great Ormond Street Hospital for Children, London, England) and Dr Alain Fischer (Necker University Hospital, Paris, France). Also, Michael R Green was supported by the Herbert Family Philanthropic Scholarship. References 1 Baumgart K, Britton W, Kemp A, French M, Robertson D. The spectrum of primary immunodeficiency disorders in Australia. J Allergy Clin Immunol 1997; 100: 415–423. 2 Tran H, Nourse J, Hall S, Green M, Griffiths L, Gandhi M. Immunodeficiency-associated lymphomas. Blood Rev 2008; 22: 261–281. 3 Rosen F, Cooper M, Wedgwood R. The primary immunodeficiencies. New Engl J Med 1995; 333: 431–440. 4 Kidd P. Th1/Th2 balance: the hypothesis, its limitations, and implications for health and disease. Alt Med Rev 2003; 8: 223–246. 5 Szabo S, Kim S, Costa G, Zhang X, Fathman C, Glimcher L. A novel transcription factor, T-bet, directs Th1 lineage commitment. Cell 2000; 100: 655–669. 6 Zheng W, Flavell R. The transcription factor GATA-3 is necessary and sufficient for Th2 cytokine gene expression in CD4 T cells. Cell 1997; 89: 587–596. 7 Yamashita M, Ukai-Tadenuma M, Miyamoto T, Sugaya K, Hosokawa H, Hasegawa A et al. Essential role of GATA3 for the maintenance of type 2 helper T (Th2) cytokine production and chromatin remodeling at the Th2 cytokine gene loci. J Biol Chem 2002; 279: 26983–26990. 8 Angkasekwinai P, Park H, Wang Y, Wang Y, Chang S, Corry D et al. Interleukin 25 promotes the initiation of a proallergic type 2 response. J Exp Med 2007; 204: 1509–1517. 9 Fort M, Cheung J, Yen D, Li J, Zurawski S, Lo S et al. IL-25 induces IL-4, IL-5, and IL-13 and Th2-associated pathologies in vivo. Immunity 2001; 15: 985–995. 10 Lee C, Iafrate A, Brothman A. Copy number variations and clinical cytogenetic diagnosis of constitutional disorders. Nat Genet 2007; 39: S48–S54. 11 Conley M, Notarangelo L, Etzioni A. Diagnostic criteria for primary immunodeficiencies. Clin Immunol 1999; 93: 190–197. 12 Iafrate A, Feuk L, Rivera M, Listewnik M, Donahoe P, Qi Y et al. Detection of large-scale variation in the human genome. Nat Genet 2004; 36: 949–951. 13 Yamagata T, Mitani K, Oda H, Suzuki T, Honda H, Asia T et al. Acetylation of GATA-3 affects T-cell survival and homing to secondary lymphoid organs. EMBO J 2000; 19: 4676–4687. 14 Asnagli H, Murphy K. The functional genomics experience (are you experienced?). Nat Immunol 2001; 2: 826–828. 15 Chen C, Zhang D, LaPorte J, Ray A. Cyclic AMP activates p38 mitogen-activated protein kinase in Th2 cells: phosphorylation of GATA-2 and stimulation of Th2 cytokine gene expression. J Immunol 2001; 165: 5597–5605. 16 Garvy B, Wiley J, Gigliotti F, Harmsen A. Protection against Pneumocystis carinii pneumonia by antibodies generated from either T helper 1 or T helper 2 responses. Infect Immun 1997; 65: 5052–5056. 17 Power C, Wei G, Bretscher P. Mycobacterial dose defines the Th1/Th2 nature of the immune response independently of whether immunization is administered by the intravenous, subcutaneous, or intradermal route. Infect Immun 1998; 66: 5743–5750. 18 Moser C, Jensen P, Kobayashi O, Hougen H, Song Z, Rygaard J et al. Improved outcome of chronic Pseudomonas aeruginosa lung infection is associated with induction of a Th1dominated cytokine response. Clin Exp Immunol 2002; 127: 206–213. 19 Sinha P, Ghosh A, Das T, Sa G, Ray P. Protein A of Staphylococcus aureus evokes Th1 type response in mice. Immunol Lett 1999; 67: 157–165. 20 Torigoe S, Ihara T, Kamiya H. IL-12, IFN-g and TNF-a released from mononuclear cells inhibit the spread of Varicella-zoster virus at an early stage of Varicella. Microbiol Immunol 2000; 44: 1027–1041. 21 Mouzaki A, Theodoropoulo M, Gianakopoulos I, Vlaha V, Kyrtsonis M, Maniatis A. Expression patterns of Th1 and Th2 cytokine genes in childhood idiopathic thrombocytopenia purpura (ITP) at presentation and their modulation by intravenous immunoglobulin G (IVIg) treatment: their role in prognosis. Blood 2002; 100: 1774–1779. 22 Weaver C, Harrington L, Mangan P, Gavrieli M, Murphey K. Th17: an effector CD4 T-cell lineage with regulatory T-cell ties. Immunity 2006; 24: 677–688. 23 Guo J, Rapoport B, MacLachlan S. Balance of the Th1/Th2 cytokines in thyroid autoantibody synthesis in vitro. Autoimmunity 1999; 30: 1–9. Supplementary Information accompanies the paper on Genes and Immunity website (http://www.nature.com/gene) Genes and Immunity