Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
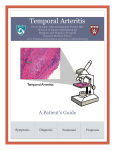
Episode9–Non‐traumaticEyeEmergencies PreparedbyDr.LucasChartier GeneralApproach: Characterizationofapatient’seyepainhelpsdeterminethelocationofthepathology: (a)up‐front,scratchy,‘sand‐in‐the‐eye’painrelatestoanteriorstructuressuchasthelids,conjunctivae, cornea,andforeignbodies; (b)deep,boring,‘behind‐the‐eye’toothachepressure‐typepainrelatestoposteriorstructures; (c)photophobiarelatestouvealtractpathologysuchasiris,ciliarybodyandchoroid Systematiceyeexamforeverypatientwithaneyecomplaint:6parts‐visualacuity(the'6thvitalsign'),visual fieldsbyconfrontation,sizeandreactivityofpupil,extraocularmovements(forcranialnervepalsies), anteriorsegment(slit‐lampexam)andposteriorsegment(fundoscopy) Thepainfulredeye Acuteangle‐closureglaucoma: Characterizedbyatleast2ofthefollowingsymptoms–acuteonsetocularpainwithnauseavomiting, intermittentblurringofvisionwithhalosseenaroundlights(duetocornealedema),photophobia,andvisual loss–alongWITHatleast3ofthefollowingsigns–intraocularpressure(IOP)>21mmHg(often40‐80 mmHg),conjunctivalinjection,cornealepithelialedemacausinghaziness,fixedandmid‐dilatedpupil,and shallowanteriorchamber(onobliqueflashlighttestwithshadowmedialtopupilcausedbythebulging anteriorchamberwhenthelightisflashedfromthepatient’stemporalside) Riskfactorsincludeelderlypatientswhoarefar‐sighted(hyperopic),andtriggersincludetransitionfrom lighttodarkenvironment(causingmydriasis)aswellasmanymedications–anticholinergic,antimuscarinic, antidepressant,antipsychotic,antihistaminic,andsympathomimetics(mostofthemthroughmydriasis) EDmanagement(re‐assessIOPq15minintheearlyphasesoftreatment): Topicalbeta‐blocker(e.g.1dropofTimolol0.25‐0.5%)todecreaseaqueoushumourproductionifno contraindicationspresent(COPD,asthma,bradycardia) Topicalcholinergic(1‐2dropsofPilocarpineq15minx2doses)tocausemyosis,decreaseangleofthe anteriorchamberatthetrabecularmeshworklevel,andincreasedrainage Parenteralagents:Acetazolaminde500mgIV(orPO)todecreaseaqueoushumourproduction,andadd Mannitol1.25‐2g/kgIVof20%solutiontoexertanosmoticdiuresisifaresponsewithotherdrugsdoesnot occur Whenisacuteangle‐closureglaucomamissed?(a)Elderly,disabilities,dementia,psychiatricptswherea thoroughhistoryandphysicalmaybechallenging(b)ptswhopresentprimarilywithheadacheorabdopain andvomiting Consideracuteangle‐closureglaucomainanyptwhohashadrecenteyesurgery Anterioruveitisoriritis: Symptoms–deep,achingpainradiatingtoperiorbitalortemporalarea,worsewitheyemovementsand accommodation,andwithPHOTOPHOBIA(veryimportant) Signs–ciliaryflush(erythemathatisworseclosertotheiris,andnotintheperipheryasinconjunctivitis), painreliefwithcyclolegicsbutnotwithtopicalanesthetics,andconsensualphotophobia(lightinthe unaffectedeye,becauseitcausesbilateralmyosis,causespain),andabnormalslitlampexamwithkeratitic precipitatesorhypopyon,andcellsandflareintheanteriorchamber,whichscintillateformillisecondsata timelike‘snowflakesinthecar’sheadlights’whendrivingatnightunderanobliqueslitlamplight Importantdiagnosistomakeinordertopreventlong‐termvisionlossconsequencesduetoscarring, malfunctionintheshapeoftheiris,andtheincreasedlikelihoodofretinaldetachment,andalsotoscreenfor the50%ofcasesthathaveunderlyinginfectiousorautoimmunediseasessuchasherpes,tuberculosis, syphilis,toxoplasmosis,aswellastheseronegativespondyloarthropathies–inflammatoryboweldisease, ankylosingspondylitis,reactivearthritis,psoriaticarthritis;alsoBehçet,rheumatoidarthritis,SLE, sarcoidosis,andscleroderma EDmanagement: Cycloplegicdropstopreventmyosis,whichactsasbothpaincontrolandbreakingupofthesynechiaecaused aroundtheiris–Homatropine(1dropTIDof2‐5%solution)lastsafewdaysandisprobablybest,or Cyclopentolate(1dropTIDof0.5‐2%solution),whichlasts1day;Mydriacyl,whichlastsonly2‐3hrs,isgood fordiagnosisbutnotfortreatment Steroidsshouldonlybeusedinconjunctionwithophthalmologistconsultationduetotheconcernfor worseningofunderlyinginfectionordevelopmentofcornealulcer,bothofwhichmayleadtolossofvision Ophthalmologicalfollow‐upwithin24hrs Thepainlessredeye Kawasakidisease: Acutesystemicvasculitisofmucosalvesselsofunknownetiologyinchildren<5yoleadingtocoronaryartery aneurysmifnottreatedacutely–thecriteriaisrememberedwiththemnemonicWarmC‐R‐E‐A‐M Warm‐Fever>39°Cfor5days,PLUS4ofthe5followingsigns(orlessin‘atypical’formofthedisease): C‐Conjunctivitis,bilateralnon‐exudative R–Rash,polymorphic(e.g.urticarial,maculopapular)andonthebody(notvesicularnorbullous) E–Edemaorerythemaofthehands,eventuallyleadingtodesquamation A‐Adenopathywithatleastoneanteriorcervicallymphnode>1.5cm(notgeneralizedoverthewholebody) M–Mucosalinvolvement:fissuredredlips,strawberrytongue IncompleteKawasaki:AmericanGuidelines‐“IfthetypicalclinicalfindingsofKawasakidiseasearepresentin achildwithfeverforlessthanfivedays,orifthreeclassicfeaturespluscoronoaryarteryfindingson echocardiographyarefound,thediagnosisstillcanbemadeandtreatmentinitiated” FeaturesthatgoagainstthediagnosisofKawasaki:exudativeconjunctivitisorpharyngitis,discreteintra‐oral lesions,bullousorvesicularrashandgeneralizedlymphadenopathy Pearls:almostalwayslookunwell/veryirritable,feverisminimallyresponsivetoanitpyretics,oftenhave peri‐analerythema,andthereisoftenasharpdemarcationatthewristandanklesfromtherednessinthe extremities Abnormaltests–Highplatelets,WBC,ESRandCRP,LFTs(especiallyAST/ALT),sterilepyuriainurine(WBC presentbutnobacteria),aswellasnormochromic,normocyticanemiaandhyponatremia Treatment–HighdoseASAandIVIG,bestiftreatwithin10dofonsetofsymptoms(lowercomplicationrate) Painlesslossofvision Ddxofpainlessacutevisuallossnotrelatedtotraumaincludesvascularocclusion,retinal detachment,vitreoushemorrhage,maculardisorders,neuro‐ophthalmologicdisease,hysteria,and secondarytomethanolorviagra Pearls–lossofvisionoversecondsisusuallyduetoavascularetiology,suchasischemiaoftheretina; posteriorvitreousdetachmentwilloftencausedebristoobstructthelightbutthepatientcanseethroughit, vs.retinaldetachmentwherebythereisafrankfielddeficit Temporalarteritis: Vasculitisofautoimmuneetiologyaffectingthearterialbranchesoftheinternalcarotidartery(ophthalmic andtemporalarteries)thatisoftenprecededbyfeaturesofpolymyalgiarheumatica(PMR) DefinitionfromtheAmericanCollegeofRheumatologists:ageover50,newheadache,abnormalityofthe temporalartery(tendernessorpulselessness),ESR>50,andpositivetemporalarterybiopsy;3outof5 positivecriteriaresultinasensitivityof93%forthediagnosis,andaspecificityof91% Symptoms–jawclaudicationanddiplopiaaremostpredictive,butalsotemporalareapainandsubacute peripheralvisionloss,lowgradefever,constitutionalsymptomslastingweekstomonths(anorexia,fatigue, myalgias,nightsweats,weightloss),ataxia,decreasedhearing Signs–beading,prominenceortendernessofthetemporalarteryisthemostpredictive,butalsotemporal scalpareatenderness,hyperesthesiaandhypersensitivity,andvestibularorhearingimpairmentattimeof presentation Thinkoftemporalarteritisinelderlypatientswhopresent'Weak&Dizzy'becauseoftensymptomsarevague ESRandCRP–NormalESRvaluesincreasewithage(age÷2formen,and[age+10]÷2inwomen),and biopsy‐positivetemporalarterycaseswithnormalESRvaulesarenotuncommon,butthecombinationof normalESRandCRPhasasensitivityof99%inrulingoutthediagnosis DonotrelyononanormalESRalonetoruleouttemporalarteritis Treatment–Steroids,withPOformulationifnoocularsymptomsarepresentandIViftheyare;donotdelay treatmentevenifbiopsycannotbeperformedforafewdaysasearliertreatmenthasbeenshowntoleadto betterimprovement(60%iftreatedwithin24hrsofsymptoms,vs.only5%iftreatedafter24hrs) CentralRetinalArteryOcclusion(CRAO)–firstimage: Suddenabruptpainlessvisionloss(i.e.strokeoftheretina,withthe samecar‐diovascularriskfactors),eithercomplete(withlight‐dark perceptiononlyoverthewholevisualfield),orwithcentralvision retained(duetothedifferentvas‐culardistributionofthefovea) Signs–PositiveRAPD(rapidafferentpupillarydefect)withablanched, non‐perfusedretinawiththepathognomoniccherry‐redspot,i.e.the redfoveaunderlyingthealmosttransparentretina,lateraltoopticdisk Management–Time‐sensitivegoaltorestorebloodflowandremove obstructionthroughvigorousmassageofeyeballtobreaktheclotdown andsenditdownstreamtoconvertittoabranchocclusion,antiplatelet therapy(ASA),anddecreaseIOP(timolol,acetazolamide,and mannitol),possiblythrombolyticsonacase‐by‐casebasis,andbreathingintoapaperbag10mineachhourto increasetheCO2withresultantarterialvasodilation CentralRetinalVenousOcclusion(CRVO)–secondimage: “DVToftheeye”,vascularengorgement(gradualchanges);tell‐tale– bigangrystormyeyeonfundcoscopicexam;hyperaemic,‘bloodand thunder’exam Painfullossofvision Opticneuritis: Inflammationoftheopticnerve(duetodemyelination),usuallyinwomen15‐45,causingtheclassictriadof unilaterallossofvision,eyepain(especiallywitheyemovement)anddyschromatopsia(washedoutcolors, especiallyred,asiflookingthroughfrostedglass) Signs–Markedlydecreasedvisualacuity(oftentolightperceptiononly),withanormaleyeandfunduscopic exam–“thepatientseesnothing,andyouseenothingonexam”(maysometimesseeblurreddiskmargins andswollenveins),withpositiveRAPD(thepupilsparadoxicallydilatewhentheflashlightisswungfromthe unaffectedtotheaffectedeyeduetothedecreasedlightperception;alsoseeninvitreoushemorrhage,retinal detachmentorischemia,andretrobulbarhemorrhage);IfplaquesareseenonMRI,morelikelytodevelop multiplesclerosis Treatment–TheOpticNeuritisTreatmentTrialshowedthatIVmethylprednisolone250mgqidx3dfollowed byanoralprednisonetaperover1wkrestoresvisionmorequickly,anddelaysthedevelopmentofmultiple sclerosisby2yrs Pearlsfromtheexperts Infectiousconjunctivitis:Themostimportantpartofmanagementisirrigationandwashingoutoftheeye Contactlenswearersshouldbeprescribedanti‐pseudomonalssuchasTobramycin(aminoglycoside),or Ciprofloxacin Suspectgonococcalinfectionwithrecentunprotectedsexualintercourse,especiallyifthereissubstantial purulentdischargethatre‐accumulatesrapidlyafterwiping,orininfants3‐6daysoflifewithredeyesafter vaginalbirth,whichrequireadmissionandIVantibiotics 4non‐traumaticeyeemergenciesthatrequirepromptophthalmologicalconsultation: Acuteangle‐closureglaucoma,severeuveitis,acutelossofvision(fromCRAO,temporalarteritis,retinal detachmentoropticneuritis),andsignificantcornealulcerationof>1mminlength Tersonsyndrome–thirdimage:Insubarachnoidhemorrhage (SAH),thesuddenriseinintracranialpressuremayleadto retinalveinsrupture,resultinginasubhyloidhemorrhage withboatshapefromcentraldiskonfundoscopy (pathognomonicforSAH)