Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
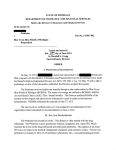
Rheumatology 2006;45:1566–1569 Advance Access publication 16 May 2006 doi:10.1093/rheumatology/kel156 Concise Report Low-dose infliximab treatment for ankylosing spondylitis—clinically- and cost-effective R. N. Jois, J. Leeder, A. Gibb, K. Gaffney, A. Macgregor, M. Somerville and D. G. I. Scott Ojectives. Infliximab has been shown to be effective in the treatment of ankylosing spondylitis (AS) when treated in a dose of 5 mg/kg at 6 weekly intervals. This dose of infliximab has not been determined by any structured randomized trials and has significant cost implications. We describe our experience of treating AS with low-dose infliximab (3mg/kg at 8 weekly intervals). The efficacy and cost implications are discussed. Methods. Patients who had active AS [Bath AS Disease Activity Index (BASDAI) 4] were treated with infliximab 3 mg/kg at 0, 2, 6 weeks and thereafter at 8 weekly intervals. Response to treatment was defined as 50% improvement in BASDAI. Other response criteria such as ASAS 20, 40 and five of the six criteria were also assessed. Direct drug costs for infliximab were determined. Results. Twenty-two consecutive AS patients received infliximab. All 22 completed treatment for 3 months, 15 patients for 6 months and 14 for 12 months. Mean age was 45 years (range 21–62) and mean disease duration 14.5 years (range 2–43). Of the patients, 54% achieved a 50% BASDAI response at 3 months and the benefit was sustained at 12 months in 63%. Similar response rate was seen with the other assessment criteria. Direct drug costs were significantly lower when low-dose infliximab regimen was used. Conclusions. Low-dose infliximab (3 mg/kg at 8 weekly infusions) is effective in the treatment of AS. Higher doses are required in a small proportion of patients when treatment is only partially effective. Titrating the dose and frequency of infusions may be required in individual patients to achieve optimal response. Using low-dose infliximab has significant economic implications. KEY WORDS: Ankylosing spondylitis, Infliximab, Anti-TNF therapy. Ankylosing spondylitis (AS) is a chronic inflammatory disease characterized by sacroiliitis, spinal inflammation and progressive spinal fusion. It may lead to significant disability and reduced quality of life [1] comparable with that of rheumatoid arthritis [2]. Non-steroidal anti-inflammatory drugs (NSAIDs) and physiotherapy were the main stay of treatment for axial disease until recently. NSAIDs were thought to have little or no effect in modifying spinal disease [3], and conventional disease-modifying drugs like methotrexate, which are effective in inflammatory arthritis, have been proved to be ineffective in spinal disease [4]. Although, more recently, continuous use of NSAIDs has been shown to reduce radiographic progression in AS [5], the only treatments to show a significant effect on spinal inflammation and quality of life have been the biological drugs—anti-TNF inhibitors. Randomized trials have shown that both infliximab [6, 7] and etanercept [8–10] are effective in suppressing inflammation in active AS, resulting in improvement in the symptoms and signs of axial as well as peripheral joint disease, accompanied by a reduction in magnetic resonance imaging evidence of inflammation in the spine [11, 12]. Infliximab has recently been shown to maintain persistent clinical response in patients with AS over 3 yrs [13]. The licensed and recommended dose of infliximab to treat AS is 5 mg/kg at 6–8 weekly intervals. This dose of infliximab has not been determined by any structured randomized trials. Infliximab at 5 mg/kg every 6 weeks was shown to be better than 3 mg/kg every 6 weeks in a small study of patients with undifferentiated spondyloarthropathy. Three patients in each group received treatment for a period of 12 weeks [14]. This observation and the fact that the higher dose was found to be effective in inflammatory bowel disease resulted in subsequent trials being undertaken at this dose. However, this high dose of infliximab has considerable cost implications. In this study, we describe our clinical experience of treating 22 consecutive AS patients attending our rheumatology clinic, using low-dose infliximab at 3 mg/kg every 8 weeks. The clinical efficacy and direct drug costs are discussed. Patients and methods Patients with AS (defined by the modified New York criteria [15]), who were symptomatic despite maximum dose of two different NSAIDs, were considered for biologicals. Eligibility criteria were defined as the presence of active disease with a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) [16] 4. Patients were referred to a specialized biologicals clinic for further assessment to discuss the introduction of infliximab. Patients with contraindications for biologicals were excluded. Department of Rheumatology, Norfolk and Norwich University Hospital, Norwich, Norfolk, UK. Received 18 December 2005; revised version accepted 7 April 2006. Correspondence to: Ramesh N. Jois, Department of Rheumatology, Norfolk and Norwich University Hospital, Colney Lane, Norwich NR4 7UY, UK. E-mail: [email protected] 1566 ß The Author 2006. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: [email protected] Low-dose infliximab for AS BASDAI, Bath AS Functional Index (BASFI) [17], Bath AS Metrology Index (BASMI) [18], patient global assessment [0–100 on visual analogue scale (VAS)], erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were recorded at baseline and at 3, 6 and 12 months follow-up. Data concerning infliximab efficacy, concomitant treatment and toxicity were recorded. Infliximab was started at 3 mg/kg and given at 0, 2 and 6 weeks of initiation and at 8-weekly intervals thereafter. Response to treatment was defined as a >50% reduction in BASDAI compared with baseline. Treatment response was assessed at 3 months. If there was at least 20% reduction in BASDAI score at 3 months, the same infliximab regimen was continued until 6 months. If the 50% reduction in BASDAI was not achieved by 6 months or 20% at 3 months, then the dose of infliximab was increased to 5 mg/kg. If the therapeutic response was short-lived, such that there appeared to be a flare before the time of the next infusion (i.e. before 8 weeks) but the initial response was reasonable, then the frequency of the infusions was increased to 6- or 7-weekly intervals. Pre-biologicals medications such as NSAIDs, sulphasalazine and methotrexate were left unchanged for the first 6 months. Other assessments of response included ASAS 20 criteria [19] and the more recently defined short-term improvement criteria: ASAS 40 and ASAS 5 of 6 [20]. Cost-effectiveness was calculated as direct drug costs among responders to the low-dose infliximab regimen (3 mg/kg 8-weekly) and compared with the potential costs involved if these patients were to be treated with infliximab in the licensed dose (5 mg/kg 6–8 weekly). The cost of each 100 mg of infliximab was taken as £451 (equivalent to E667.5) (cost as per British National Formulary, March 2005). The direct drug cost savings after using the low-dose infliximab regimen was determined. Statistics All the values were expressed as median (range). Differences of the various response criteria at 3, 6 and 12 months when compared with baseline were tested using the Wilcoxon matched-pairs signed-ranks test for statistical significance. A P < 0.05 was considered statistically significant. The percentage of patients who met the treatment response criteria was determined by actuarial analysis. Results We treated 22 consecutive AS patients with infliximab 3 mg/kg at 8-weekly intervals. The baseline characteristics of the patients are shown in Table 1. One patient had previous history of psoriasis and another had ulcerative colitis, both of which were quiescent. Twenty-two patients have been treated for 3 months, 15 for 6 months and 14 for 12 months. The median change in BASDAI along with other assessment parameters over time are shown in Table 2. The BASDAI for individual patients at different time points are illustrated in Fig. 1. The percentage of patients who attained BASDAI 50 response at various time points and the other assessment parameters— ASAS 20, ASAS 40 and ASAS 5 of 6—are shown in Table 3. Three of the 15 patients (20%) who continued infliximab to 6 months did not show 50% reduction in the BASDAI scores at 3 months but achieved this response criterion at 6 months. They had, however, shown a 20% reduction in BASDAI at 3 months. One patient increased the frequency to 7-weekly cycles at 3 months and one patient to 6-weekly cycles at 3 months for optimal response. Two patients have reduced the frequency of 1567 TABLE 1. Baseline characteristics Total number of patients Male/female Age, yrs: median (range) Disease duration, yrs: median (range) HLA B27 positive: n (%) Peripheral arthritis: n (%) Methotrexate users: n (%) Methotrexate and sulphasalazine combination users: n (%) NSAID users: n (%) 22 19/3 45 (21–62) 10.5 (2–27) 20 (90.9) 8 (36) 6 (27) 2 (9) 22 (100) infliximab infusions to 9-weekly cycles on 3 mg/kg after 6 months of treatment. Two of the non-responders increased the dose to 5 mg/kg (one after 6 months and the other after 12 months). One patient switched over to etanercept after 12 months. Overall, 19 of the 22 patients are still receiving infliximab at 3 mg/kg. No significant side effects from infliximab were observed. About 40% of the patients were able to stop NSAID use altogether. Of the eight methotrexate users, three stopped medication and five reduced the dose by a mean of 11.3 mg/week. Both the patients, who were on sulphasalazine, discontinued the drug. Cost evaluation Direct drug cost calculations were done on the assumption that the 19 patients who are at present receiving infliximab 3 mg/kg dose would continue the same treatment for a period of 12 months. The dose of infliximab was calculated after taking into consideration the actual body weight of these 19 patients. Three doses of infliximab were required for induction (0, 2 and 6 weeks) and thereafter an additional 6 doses for maintenance (8-weekly infusions) in the first year of treatment. The resulting direct drug cost would be £183 507.26 (E272 324.77) for the first year of treatment. Assuming that these 19 patients would need to be treated according to their actual body weight with the recommended (licensed) dose of infliximab i.e. 5 mg/kg 6-weekly infusions, they would need three doses for induction (0, 2 and 6 weeks) and nine doses (6-weekly infusions) or six doses (8-weekly infusions) for maintenance when treated for the first year. The resulting cost would then be £407 794.2 (E605 166.59) for the first year of treatment when treated 6-weekly and £305 845.65 (E453 874.94) when treated 8-weekly infusions. By using the low-dose infliximab regimen, the potential savings to our unit for the first year would therefore be £224 286.94 (E331 944.67) when compared with the 6-weekly regimen and £122 338.39 (E181 060.81) with the 8-weekly regimens. Discussion The efficacy of infliximab in relieving various symptoms in AS has been clearly demonstrated in randomized trials [6, 7]. The recommended and licensed dose of infliximab for treating AS is 5 mg/kg 6- to 8-weekly infusions. Infliximab has been found to very effective in controlling inflammation in rheumatoid arthritis at a lower dose (3 mg/kg 8-weekly infusions) [21]. There have not been any dose-finding randomized trials in AS. Maksymowych et al. [22] were the only group (from published data) to report efficacy of infliximab at 3 mg/kg every 8 weeks and noted that the lower dose appeared to be effective for both axial and peripheral involvement in AS. BASDAI 50 response was seen in 58% of their patients (n ¼ 17) at 3 months and in 75% at 12 months (n ¼ 8). The BASDAI 50 response seen in our cohort (54% at 3 months and 63% at 6 and 12 months) is comparable. R. N. Jois et al. 1568 TABLE 2. Median (range) of various parametres with infliximab (3 mg/kg) treatment Assessment parameter 0 months (n ¼ 22) BASDAI (0–10) BASFI (0–10) BASMI (0–10) Spinal pain VAS (0–10) Morning stiffnessa (0–10) ESR (mm/h) CRP (mg/dl) (normal<7) 6.6 6.4 4.6 6.7 6.2 22 21 (4.2–8.7) (4.7–8.2) (0.9–7.7) (1.0–9.5) (1.2–9.7) (9–119) (3–108) 3 months (n ¼ 22) 3.2* 3.7y 3.6y 4.4y 3.2y 9* 7* (0.2–8.5) (1.0–8.9) (0.8–7.7) (0.1–9.9) (0.3–9.2) (3–31) (3–20) 6 months (n ¼ 15) z 2.1 1.7z 3.8z 2.5** 1.5z 8y 7y (0.2–6.9) (0.1–8.6) (0–7.4) (0.1–8.6) (0–9.2) (3–21) (3–17) 12 months (n ¼ 14) 1.8z 1.7y 3.2y 2.5z 1.1z 12z 6z (0.1–9.9) (0.1–9.2) (0–6) (0.1–10) (0–9.35) (3–40) (3–34) 6 4 0 2 BASDAI 8 10 *P < 0.0001 yP < 0.001 zP < 0.01 **P < 0.05. a Average of items 5 and 6 on BASDAI. 0 3 6 12 Follow-up (months) FIG. 1. BASDAI for individual patients at different time points. TABLE 3. Responders to various assessment criteria as determined by actuarial analysis Variable BASDAI 50 ASAS 20 ASAS 40 ASAS 5 of 6 Time (months) Probability of meeting response criteria (%) 95% CI 3 6 12 3 6 12 3 6 12 3 6 12 54.6 63.6 63.6 63.6 78.2 78.2 50.0 66.7 66.7 59.1 79.6 79.6 35.7–75.6 41.8–84.9 41.8–84.9 44.3–82.6 56.9–93.7 56.9–93.7 31.6–71.8 44–87.6 44–87.6 39.9–79.2 58.3–94.4 58.3–94.4 and BASMI at 3 months compared with baseline in our cohort was statistically significant (P < 0.0001 for BASDAI and P < 0.001 for the others). The absolute change in the mean value in various indices in our cohort (data not shown) compared with other studies like Braun et al. [23] were similar; for example, BASDAI was 3.0 in our cohort and 3.3 in Braun et al., BASFI 2.5 and 2.2, and BASMI 0.8 and 0.9 in the two respective groups. The absolute change in all these parameters at 6 months and after 1 yr was also similar in both studies. The efficacy of infliximab at lower doses has also been shown in the present study by other response criteria such as ASAS 20, 40 and 5 of 6. ASAS 20 response in our cohort was 63% at 3 months and 78% at 6 and 12 months. The ASAS 20 response seen when higher dose of infliximab (5 mg/kg 6 weekly) was used in various other trials were: 75% at 3 months [6], 80% [23] at 6 months and 60 [23] and 71% [24] at 12 months. The percentage of patients meeting the ASAS 40 (50% at 3 months and 66% at 6 and 12 months in our cohort compared with 47% at 6 months [7] and 66% at 12 months in other trials [24]) and ASAS 5 of 6 (59% at 3 months and 79% at 6 and 12 months in our cohort compared with 49% at 6 months [7] and 51% at 12 months in other trials [24]) when treated with inflixiamb 3 mg/kg 8 weekly is very encouraging and the efficacy is sustained over a period of 12 months. However, it is important to note that the percentage of responders in our study was determined by actuarial analysis, which was not the case with other studies. About 40% of the patients were able to completely stop NSAID use, and reduction in dose or discontinuation of DMARDs such as methotrexate and sulphasalazine were observed. The recommended dose of infliximab for AS has significant cost implications and using the low-dose regimen, as we have shown, has a lot of potential for cost savings. The cost savings is not only with the direct drug costs but will also include various other indirect costs such as hospital attendance, nursing time, etc. It is important to note that the numbers of patients treated in our study are small and the results, therefore, need confirmation in a large cohort, such as a well-structured randomized controlled trial, where AS patients are treated with either infliximab at the licensed dose or on low dose. Conclusions The BASDAI 50 response seen in our patients is also comparable with other studies in which patients were treated with infliximab 5 mg/kg (53% at 3 months [6], 51% at 6 months [7] and 51% [23], 57% [24] and 60% [25] at 12 months). Even though direct comparison between studies is not always possible due to differences in patient demographics, assessment criteria and strict exclusions in formal clinical trials, the response rate seen in our patients is very encouraging especially when using lower doses of infliximab. The median change in BASDAI, BASFI We have shown that infliximab is effective in suppressing the signs and symptoms of AS at 3 mg/kg and that higher doses are required in a small proportion of patients when treatment is only partially effective. This may be adjusted also by titrating the dose to individual patients and titrating the frequency of infusions. Starting at the low dose of infliximab (3 mg/kg 8-weekly infusions) and then increasing the dose when indicated seems a sensible way in clinical practice, especially in a cashstrapped health service. Using low-dose infliximab has significant economic implications. Low-dose infliximab for AS Rheumatology Key messages Low-dose infliximab (3 mg/kg 8 weekly) is effective in treatment of AS. Results of efficacy are comparable with the recommended high-dose regimen (5 mg/kg 6 weekly). Low-dose infliximab has significant cost implications. 11. 12. 13. Acknowledgements We would like to thank all our patients without whom this work would not have been possible. We would also like to thank Dr P. Merry, consultant rheumatologist, Norfolk and Norwich University Hospital, for allowing us to include his patients in the study. Research grant support to the department received from ScheringPlough, Wyeth and Abbott Pharmaceuticals. 14. 15. 16. References 1. Ward MM. Quality of life in patients with ankylosing spondylitis. Rheum Dis Clin North Am 1988;24:815–27. 2. Zink A, Braun J, Listing J, Wollenhaupt J. Disability and handicap in rheumatoid arthritis and ankylosing spondylitis: results from the German rheumatological database. J Rheumatol 2000;27:613–22. 3. Miceli-Richard C, Dougados M. NSAIDs in ankylosing spondylitis. Clin Exp Rheumatol 2002;20(Suppl 28):S65–6. 4. der Horst-Bruinsma IE, Clegg DO, Dijkmans BA. Treatment of ankylosing spondylitis with disease modifying antirheumatic drugs. Clin Exp Rheumatol 2002;20(Suppl 28):S67–70. 5. Wanders A, Heijde D, Landewe R et al. Non-steroidal antiinflammatory drugs reduce radiographic progression in patients with ankylosing spondylitis: a randomized clinical trial. Arthritis Rheum 2005;52:1756–65. 6. Braun J, Brandt J, Listing J et al. Treatment of active ankylosing spondylitis with infliximab—a double-blind placebo controlled multicenter trial. Lancet 2002;359:1187–93. 7. der Heijde D, Dijkmans B, Geusens P et al. Efficacy and safety of infliximab in patients with ankylosing spondylitis. Results of a randomized, placebo-controlled trial (ASSERT). Arthritis Rheum 2005;52:582–91. 8. Davis JC Jr, van der Heijde D, Braun J et al. Recombinant human tumor necrosis factor receptor (etanercept) for treating ankylosing spondylitis: a randomized controlled trial. Arthritis Rheum 2003;48:3230–6. 9. Gorman JD, Sack KE, Davis JC. Treatment of ankylosing spondylitis by inhibhition of tumor necrosis factor alpha. N Engl J Med 2002;346:1349–56. 10. Brandt J, Khariouzov A, Listing J et al. Six-month results of a double-blind, placebo controlled trial of etanercept treatment in 17. 18. 19. 20. 21. 22. 23. 24. 25. 1569 patients with active ankylosing spondylitis. Arthritis Rheum 2003;48:1667–75. Sieper J, Baraliakos X, Listing J et al. Persistent reduction of spinal inflammation as assessed by magnetic resonance imaging in patients with ankylosing spondylitis after 2 years of treatment with the anti-tumor necrosis factor agent infliximab. Rheumatology 2005;44:1525–30. Lim AYN, Gaffney K, Marshall T. Juvenile onset spondylodiscitis: magnetic resonance imaging changes with infliximab. Rheumatology 2004;43:1456–7. Braun J, Baraliakos X, Brandt J et al. Persistent clinical response to the anti-TNF- antibody infliximab in patients with ankylosing spondylitis over 3 years. Rheumatology 2005;44:670–6. Brandt J, Haibel H, Reddig J et al. Suceessful short term treatment of severe undifferentiated spondyloarthropathy with anti-tumor necrosis factor alpha monoclonal antibody infliximab. J Rheumatol 2002;29:118–22. der Linden S, van Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 1984;27:361–8. Garrett S, Jenkinson T, Kennedy LG et al. A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 1994;21:2286–91. Calin A, Garrett S, Whitelock H et al. A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol 1994;21:2281–5. Jenkinson TR, Mallorie PA, Whitelock HC et al. Defining spinal mobility in ankylosing spondylitis (AS): the Bath AS Metrology Index. J Rheumatol 1994;21:1694–8. Anderson JJ, Baron G, van der Heijde D et al. Ankylosing spondylitis assessment group preliminary definition of short-term improvement in ankylosing spondylitis. Arthritis Rheum 2001;44:1876–86. Brandt J, Listing J, Sieper J et al. Development and preselection of criteria for short-term improvement after anti-TNF therapy in ankylosing spondylitis. Ann Rheum Dis 2004;63:1438–44. Maini RN, St.Clair EW, Breedveld FC et al. Infliximab (chimeric anti-tumor necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomized phase III trial. ATTRACT study group. Lancet 1999;354:1932–9. Maksymowych WP, Jhangri GS, Lambert RG et al. Infliximab in ankylosing spondylitis: a prospective observational inception cohort analysis of efficacy and safety. J Rheumatol 2002;29:959–65. Braun J, Brandt J, Listing J et al. Long term efficacy and safety of infliximab in the treatment of ankylosing spondylitis: an open, observational, extension study of a three-month, randomized, placebo-controlled trial. Arthritis Rheum 2003;48:2224–33. Nikas SN, Alamanos Y, Voulgari PV et al. Infliximab treatment in ankylosing spondylitis: an observational study. Ann Rheum Dis 2005;64:940–2. Temekonidis TI, Alamanos Y, Nikas SN et al. Infliximab therapy in patients with ankylosing spondylitis: an open label 12 month study. Ann Rheum Dis 2003;62:1218–20.