Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
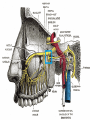
Slide 1 Sphenopalatine Ganglion Anesthetic Block for Treatment of Intractable Migraine and Cluster John E. Castaldo MD Professor and Chief of Neurology College of Medicine USF Timothy M. Breidegam Endowed Chair in Neurology Lehigh Valley Health Network Slide 2 Anatomy of SPG Slide 3 ssSs SPG spg Slide 4 Slide 5 Slide 6 Slide 7 Structure The Spenopalatine ganglion is the largest of the parasympathetic ganglia associated with the branches of the Maxillary Nerve It is triangular or heart-shaped, of a reddish-gray color, and is situated just below the Maxillary nerve as it crosses the fossa. Supplies the lacrimal gland, paranasal sinuses, glands of the mucosa of the nasal cavity and pharynx, the gingiva, and the mucous membrane and glands of thehard palate. It communicates anteriorly with the nasopalatine nerve. Slide 8 Roots Receives Sensory parasympathetic and sympathetic input Sensory root derived from two sphenopalatine branches of the maxilary nerve Parasympathetic root is derived from the nervus intermedius of the facial nerve through the greater petrosal branch Slide 9 Slide 10 Connections to CNS Slide 11 Possible Sites of Action of Triptans in the Trigeminovascular System Possible Sites of Action of Triptans in the Trigeminovascular System Goadsby PJ, et al. N Engl J Med. 2002;346:257-70. Reprinted with permission. Slide 12 Pathophysiology of Migraine Goadsby PJ, et al. N Engl J Med. 2002;346:257-70. Slide 13 BOLD MRI WMA Slide 14 MRI and stroke PET Slide 15 Slide 16 Slide 17 Patterns of Use of Peripheral Nerve Blocks and Trigger Point Injections Among Headache Practioners in the USA: Results of the American Headache Society Interventional Procedure Study Avi Ashkenazi et al Headache 2010;50:937-942 Slide 18 Slide 19 Slide 20 Anatomy of Cranial Occipital Nerves Slide 21 Slide 22 Ashkenazi et al 2010 . CCH = chronic cluster headache; CM = chronic migraine; CTTH = chronic tension-type ; ECH = episodic cluster; ETTH = episodic tension-type headache; HC = hemicrania continua; MA = migraine with aura; MO = migraine without aura; NDPH = new daily persistent headache; ON = occipital neuralgia; SM = status migrainosus. Slide 23 Indications for use of GON Block Slide 24 Peripheral Nerve Block Locations For greater and lesser ONBs For supraorbital nerve and infraorbital nerve blocks . Few participants performed auriculotemporal nerve blocks. s or responders used the occipital ridge, the occipital notch, or midway between the occipital protuberance and mastoid. delivered at the supra- and infraorbital notch or depression tended to localize the nerve relative to the tragus or zygomatic arch Localized by palpation The supratrochlear nerve was also rarely injected Slide 25 Peripheral Nerve Blocks Outcome Judged successful by 89% if headache resolved in the days following Judged successful by 68% if headache resolved following the injection Percent of injections judged successful by either criteria? Unknown Slide 26 Sphenopalatine Block Intranasal with marcaine soaked pledgets Infrazygomatic lateral approach through salivary glands Suprazygomatic lateral approach: Glassman procedure. Slide 27 Glassman Procedure: set up 5 CC syringe 22 g 2 inch needle Mixture of 0.5% Ropivacaine (4 cc) and 40 mg of Methylprednisolone (1cc) Patient lying in the lateral decubitus position An assistant to offer reassurance Alcohol and gauze pads and ice pack 5 minutes to prepare, 2 minutes to inject Slide 28 Glassman procedure Patient is asked to stay in the lateral decubitus position for ten minutes (injected side up) Then turn to lying on the back 5 minutes Then sitting up semi recumbent position for 5 minutes until pain is relieved Slide 29 SPG Block: Glassman Slide 30 Note position and maxillary art Slide 31 Patient Comfort No patient reported the procedure as “painful” enough as to have wished it wasn’t done. Most rated it associated with a mild discomfort no greater than 2-3 on a scale of 1-10. Some rated 0 discomfort with the procedure in comparison to their level of headache pain. All patients found immediate relief of nausea, vomiting and sensitivity to sound and light. Slide 32 Results of SPG block prior to DC from the office Complete pain relief 16% Pain reduction 3 pointsLeichert scale 46% Pain reduction of 3-6 points 31% Pain reduction of greater than 50% 37% No Relief whatsoever 1% NB: Pain relief by Leichert Scale 1-10 and measured at 20 minutes after injection Slide 33 Patient Selection Status Migrainosis refractory to steroids, DHE , triptans and narcotics Chronic Migraine refractory to multiple medications including Botox Cluster refractory to Prednisone. Lithium and Valproic acid Hemicrania continua New Daily Persistent Headache Pain level of 7-10 at time of procedure Slide 34 PAIN LEVEL REDUCTION WITH SPG BLOCK n=146; 2008-12 Slide 35 # of Name update ND Kathryn W David H Sharon H Sarah M Beverly A Kama N Machelle Karen D Denise S George B Danine S Multiple SPG Blocks MRN# 149980 1185525 1375873 00450464 1196876 1394774 00597342 00217610 00218321 1567412 00681442 injections 6 4 3 5 4 4 8 11 3 4 4 4 Bilat Bilat Bilat bilat bilat uni uni uni bilat uni bilat bilat Bilat/uni chronic mig chronic mig migraine hemicrania continua chronic mig chronic mig chronic mig chronic mig chronic mig cluster/ mig chronic mig Botox chronic mig Slide 36 Case Study: 44 year old woman Hx: Migraine with aura all her life starting at menarche Increasing severity and frequency over 10 years. Concern over deviated septum and “chronic sinus headache” ENT evaluation negative Frequency Daily Severity 8-10 Treating with 100 Exedrine per week. Slide 37 HA profile CHARACTER: The pain feels like " Burning in cheeks, like I have a pulse in my eyeballs) “ ice picks to biparietal regions AURA:with migraine spots Location: right anterior quadrant of head predominant ASSOCIATED SYMPTOMS:face and scalp sensitivity. skin in the nose and over face hurts at times. AUTONOMIC FEATURES:nausea and vomiting and light sensitivity and sound sensitivity TRIGGERS:light, bacon, stress, menses odors can trigger. Slide 38 HA profile cont. EXERTIONAl: makes both types of headaches worse. SLEEP HYGEINE:can't sleep well. Can fall asleep STRESS: High stress "normal everyday" SOCIAL LIFE:withdrawn from friends because of daily pain ANXIETY: high anxieyt all the time. DEPRESSION:She feels sad and easily becomes tearful ESTROGEN CYCLES: worse Slide 39 HA Profile FAILED MEDS:Cymbalta, physical therapy, yoga, pilates. Flexeril, tramadol toradol injections.skelaxin , valium, xanax, topamax and Amitriptyline, Nortriptyline,Cymbalta, Effexor, Zoloft, steroids, IV narcotic Imitrex minimally helpful Other symptoms: Positional vertigo worsening over the last 10 months Slide 40 Therapy Lamictal advance to 150 bid Get off OTC analagesic meds Migraine hygeine Brief course of steroids and ergot therapy Trazodone therapy for sleep and HA Epley maneuver Slide 41 Abnormal MRI Slide 42 Outcome Chronic Daily Headache persists Could not tolerate Trazodone self DC Vertigo cleared Ice pick pain better Depression remains high Anxiety high Appears in office in excruciating pain with nausea and vomiting. Slide 43 Therapy Right SPG anesthetic nerve block using 1 cc of 40 mg depomedrol and 4 CC 0.5 % Ropivacaine. Fluoxetine 20 mg daily initiated Lamictal continued at 150 mg po bid Maxalt for break through pain Slide 44 Outcome “I have my life back” No significant headaches for 3 months since SPG injection No vertigo since Epley maneuver No ice pick pain Bipolar symptoms clear Depression markedly improved Sleep architecture improved. Slide 45 Conclusions: SPG injections are safe, well tolerated and effective abortive therapy for migraine and cluster headaches Glassman approach is better tolerated that trans nasal by most patients Most patients achieve and immediate 50100% reduction in pain in 20 minutes with better results evolving over hours to days Durability of relief is variable lasting days to months in most Slide 46 Conclusion Continued Best results appear to be in patients with unilateral anterior quadrant head pain centered over temple, forehead and eye. Results are superior to auriculotemporal nerve blocks in combination with occipital nerve blocks, the gold standard of cranial block therapy Best results obtained with comprehensive preventive headache therapy including diet, exercise, preventive/abortive meds, psych and attention to sleep architecture Slide 47 Next steps Randomize clinical trial comparing GON block to SPG block in refractory pain patients Quantitative long term evaluations of post procedure pain relief. Identification of headache subtypes most responsive to procedure Assess for long term complications, if any Slide 48 Questions?