Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Clinical Science and Molecular Medicine (1975) 48, 97s-100s.
Some haemodynamic effects of compound AH 5158 compared with
propranolol, propranolol plus hydrallazine, and diazoxide:
the use of AH 5158 in the treatment of hypertension
B. N. C. P R I C H A R D , F. 0. T H O M P S O N , A . J . B O A K E S
AND
A. M. JOEKES
Departnrent of Clinical Pharmacology, Medical Unit, University College Hospital Medical School and Hypertension Clinic,
Unicersity College Hospital, London, and St Peters Group of Hospitals, Institute of Urology, London
Key words: compound AH 5158, hypertension.
properties (Boakes, Knight & Prichard, 1971).
Compound AH 5158 produced a parallel shift in
the dose-response curve to isoprenaline-induced
tachycardiaand phenylephrine-induced hypertension.
In the present study, with non-invasive techniques,
we have compared some haemodynamic effects of
compound AH 5158 with those of beta-adrenergic
blockade alone (propranolol), with the effects of a
beta-blocking agent in combination with a vasodilator (propranolol plus hydrallazine), and finally
with those of vasodilatation from diazoxide.
We also report our experience in the treatment of
hypertension with compound AH 51 58 in a series of
thirty-one patients.
Introduction
Methods
Summary
1. Intravenous administration of compound AH
51 58, which possesses alpha- and beta-adrenergic
receptor-blocking properties, produces haemodynamic effects similar to those seen from the combined effects of propranolol and hydrallazine.
2. Chronic oral administration has demonstrated
that compound AH 5158 is an effective hypotensive
agent capable of controlling the blood pressure in
patients previously requiring large doses of drugs
such as methyldopa. Some postural and exercise
hypotension may be seen with larger doses.
Beta-adrenoceptor-blocking drugs have been used
in the treatment of hypertension for over 10 years
(Simpson, 1974). The experience of some investigators has indicated that they are of similar potency
to bethanidine, guanethidine or methyldopa
(Prichard & Gillam, 1969; Prichard, Gillam &
Graham, 1970; Zacharias, Cowen, Vickers & Wall,
1972). There have also been reports of the use of
beta-receptor-blocking drugs in combination with
an alpha-receptor-blocking drug (Beilin & JuelJensen, 1972).
Compound AH 5 158, 5-{I-hydroxy-2-[(1-methyl
3-phenylproypl)amino]ethyl) salicylamide, was
found to possess beta- and alpha-adrenergic receptor-blocking properties in animals, and preliminary human pharmacological studies confirmed these
Haemodynamic studies
Twelve patients were studied supine at rest.
Changes in thoracic impedance were used to calculate
the stroke volume, two tape electrodes being placed
around the neck and two around the lower thorax
(Kubicek, Patterson & Witsoe, 1970). The impedance method for cardiac output measurement
correlates well with that of the standard isotopic
technique, giving a correlation coefficient of 0.82
(Hill & Thompson, 1975). Blood pressure was
measured by a standard arm sphygmomanometer.
Patients rested for 10 min and base-line readings of
the stroke volume, pulse rate and blood pressure
were taken. Twelve patients were given 0.5 mg
(0.001 mmol)/kg of compound AH 5158 intravenously over 10-20 min. The total dose ranged from
22 mg (0.06 mmol) to 70 mg (0.19 mmol). The blood
pressure was taken at 5 min intervals and when the
maximum hypotensive effect was obtained the
Correspondence: D r B. N. C. Prichard, Department of
Clinical Pharmacology, Medical Unit, University College
Hospital Medical School, University Street, London,
W.C.I.
97s
B. N. C. Prichard et al.
98s
cardiac output and pulse rate measurements were
repeated. Twelve other patients were given propranolol intravenously, 8 mg (0.028 mmol)-16 mg
(0.056 mmol) injected over 10-20 min, sufficient to
produce a fall of heart rate to 60 beatsimin. When
the fall in the cardiac output and pulse rate had
stabilized, 20 mg (0.0125 mmol) of hydrallazine was
given intravenously over 1-2 min. The effects of
300 mg (1.31 mmol) of intravenous diazoxide was
studied in a further twelve patients. The cardiovascular measurements were repeated before and
after d iazoxide but with these patients the cardiac
output was estimated by more standard isotopic
technique employing praecordial radioactivity
counting (Veal & Vetter, 1965).
Treattilent of hypertensioti
Patients were seen in the hypertension clinic
under standardized conditions. Blood pressures
were taken by a physician after the patient had
rested supine on a couch for 3 min. Readings were
Mean blood
pressure
Pulse
rote
repeated after standing for 1 min and again after 1
min of 8 in steps up and down at the rate of 1 cycle
in 2.5 s, i.e. 24 stepsimin. All blood pressures were
taken with the London School of Hygiene and
Tropical Medicine Sphygmomanometer (Rose,
Holland & Crowley, 1964). Calculations were based
on the average of three readings before and the
latest three during the administration of compound
AH 5158.
A large number of the patients in this study were
already under treatment with a variety of drugs
(see below). Although not a formal comparative
study this made it possible to obtain some idea of the
Comparative efficiency of compound A H 5158.
Full blood count, standard biochemical investigations and urine analysis were performed at
I , 3 and 6 months, at I year and thereafter at yearly
intervals. Dosage was commenced at 25 mg t.d.s.
Increments usually of 25 mg a dose were made up to
200 mg, of 50 mg a dose up to 400 mg and thereafter
of 100 mg a dose, up to a maximum of 3200 mg
daily.
Cardiac
outpur
Stroke
volume
Peripheral
resistance
T
I1
40
+
30
T
20
10
10
20
30
0 01
P < O O O l 0001
P 5158 P D
H
1
0 001
0001
P 5158 P D
H
001
0 01
P 5158 P D
a
H
P 5158 P
a
H
D
0001 0001
0 0 2 0 001
P 5158 P D
a
H
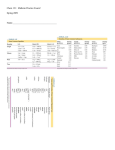
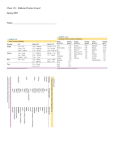
I . A comparison of the haernodynarnic response to intravenous propranolol (P), compound A H 5158,
propranol plus hydrallazine (P & H), and diazoxide (D). Vertical lines indicate SD.
FIG.
Haernodynamic effects of compound AH 51 58
Results
Haemodyrianiic studies (Fig. 1)
The hypotensive effect of compound AH 5158
( n = 12) developed over 15 min and was usually
maximal within 30 min. The average systolic pressure
fell from its initial value of 176 (SD 31) mmHg to
146 (SD 23) mmHg, with the diastolic pressure
falling from 1 13 (SD 19) mmHg to 92 (sD 18) mmHg.
The mean pressure fell by 26 (SD 9) mmHg which
represented a percentage fall of 18.5 (P<O.OOI).
There was no significant change in the heart rate and
cardiac output, but the peripheral resistance fell by
13.5% (SD 22) (Pt0.02).
Propranolol ( n = 12) had no acute hypotensive
action but reduced the pulse rate by 16.5 (SD 13)
(P<O.OOl) and the cardiac output by 22% (SEM
14.5) (P <0.001), peripheral resistance rising by
35.5% (SD 26.5) (P<O.OOI). The administration of
hydrallazine to these patients lowered the pressure
by 18% (SD 7.5) (P<O-Ol) and the peripheral
resistance by 33% (SD 19) (P<O.OOI), there being no
significant change in the pulse rate or cardiac output.
Diazoxide (n = 12) produced the greatest hypotensive effect with a fall of 27% (SD 7) (P<O.OOI).
This was associated with a rise in the pulse rate of
21.5% (SD 6.5) (P<O.OOl), an increased cardiac
output of 31.5% (P<O.Ol) and a fall in the peripheral
resistance of 39.5% (SD 19) (P<O.oOl).
Treatment of hypertension
Thirty-one patients were treated with compound
AH 5158 for periods between 3 and 36 months,
average 16 (SE 2.0) months. There were twenty-one
male and ten female patients. Fourteen patients had
electrocardiographic changes of left ventricular
hypertrophy, and five others had ischaemic changes
on the electrocardiogram. There were nine patients
with an enlarged heart on chest X-ray. Numbers
showing fundal changes were: grade IV, one patient;
grade 111, two; grade 11, ten; grade I, seven. Fundi
were normal in eleven patients.
Seven patients had been previously treated with
methyldopa, seven with debrisoquine or bethanidine,
four with other beta-adrenergic receptor-blocking
drugs, and two with reserpine. Eleven patients were
previously untreated.
Side-effects and withdrawals from treatment
Three patients stopped treatment because of
99s
side-effects. One patient felt ‘bloated‘; one patient
had postural dizziness; the third, who had experienced side-effects from small doses of a number of
hypotensive agents, had a feeling of ‘muzziness’.
There were five patients in whom compound AH
5158 was stopped for reasons unrelated to drug
treatment. Two of the remaining patients had sideeffects on compound AH 5 158, in one case tiredness,
in the other occasional nausea after taking the
tablet; in neither was it necessary to stop therapy.
Response of blood pressure
Patients previously on inethyldopa (IT = 7). The
average blood pressures on methyldopa (average
dose 1589 mg/day, range 375-4000 mg/day) were
173 (SE 12.5)/96 (SE 7.0) mrnHg supine, 157 (SE
9.2)/102(SE 5.0) mmHg standing and 155 (SE 10.9)/89
(SE 5.6) mmHg after exercise. Four of these patients
required a diuretic, and one bethanidine 50 mg daily
in addition. The pressures on compound AH 5158
were 156 (SE 8.0)/88 (SE 4.1) mmHg supine, 137
(SE 4.3)/91 (SE 2.6) mmHg standing and 135 (SE
47)/84 (SE 2.0) mmHg after exercise. The average
dose of compound AH 5 158 was 1 189 (SE 437) mg,
only one patient requiring a diuretic in addition.
The blood pressure of one patient while on 4000 mg
of methyldopa, bethanidine (50 mg) and hydrochlorothiazide (100 mg) daily averaged 226/109
mmHg supine, 150/97 mmHg standing and 106/65
mmHg after exercise. During treatment with compound AH 5158, 3200 mg a day, together with
hydrochlorothiazide (100 mg), the average pressures
were 190/107 mmHg supine, 131/90 mmHg standing
and 119/77 mmHg after exercise.
Patients previously on bethanidine or debrisoquine
(n = 7). The average blood pressures on bethanidine
or debrisoquine, together with a diuretic in four
patients, were 187 (SE 14.1)/102 (SE 8.2) mmHg
supine, 179 (SE 16.7)/105(SE 6.4) mmHg standing and
169 (SE 17.0)/94 (SE 4.7) mmHg after exercise. ,On
compound AH 5158, in an average dose of 1345
(SE 517) mg, pressures were 156 (SE 7.6)/89 (SE 3.6)
mmHg supine, 140 (SE 6.1)/94 (SE 3.7) mmHg standing, and 141 (SE 7.6)/85 (SE 4.2) mmHg after exercise.
Patients previously on other beta-adrenoceptorblocking drugs ( n = 4). The four patients in this
group had an average supine blood pressure 163
(SE 20.0)/101 (SE 14.6) mmHg, an average standing
pressure 157 (SE 14.9)/107 (SE 6.1) mmHg and 158
(SE 13.0)/101 (SE 5.1) mmHg after exercise, whilst on
100s
B. N. C. Prichard et at.
propranolol o r sotalol. During treatment with
compound AH 5158, average dose 1808 mg (SE
692), pressures were 157 (SE 6.6)/91 (SE 2.8) mmHg
supine, 133 (SE 6.7)/94 (SE 4.3) mmHg standing and
127 (SE 13.2)/83 (SE 8.4) mmHg after exercise.
Patients previously treated with reserpine ( n = 2).
The pressures on reserpine were 168172 mmHg
supine, 170/90 mmHg standing, and 171/77 mmHg
after exercise. During the administration of compound AH 5158 (average dose 1020 mg) pressures
were I61 /77 mmHg supine, 101187 mmHg standing,
and 152/74 mmHg after exercise.
Patients not on treatment bejore cot?iporirid A H
5158 ( n = 11). The mean supine blood pressure in
this group was 168 (SE 5.0)/103 (SE 3.9) mmHg,
standing was 168 (SE 5.1)/116 (SE 3.5) mmHg, and
184 (SE 6.3)/113 (SE 5.4) mmHg after exercise. On
treatment with compound AH 5158, average dose
467 (SE 150) mg, the supine blood pressure was 148
(SE 4.8)/85 (SE 2.3) mmHg, standing was 137 (SE
5.9)/93 (SE 3.3) mmHg and after exercise was 147
(SE 6.9)/90 (SE 2.9) mmHg.
Discussion
The absence of an acute hypotensive effect with a
fall of heart rate and cardiac output and an increase
in peripheral resistance confirms earlier findings
with propranolol. This is in contrast to the pronounced peripheral vasodilatation produced by
intravenous diazoxide, where the resulting fall in
blood pressure led to a reflex tachycardia and an
increase in the cardiac output. The combination of
beta-adrenoreceptor blockade with peripheral
dilatation from hydrallazine reduced the secondary
reflex changes. Compound AH 5158 produced a
significant fall of blood pressure, and the haemo-
dynamic effects were comparable with those produced by propranolol plus hydrallazine. It is an
effective hypotensive agent that appears capable of
controlling the blood pressure in patients that previously needed large doses of drugs such as
methyldopa. Since compound A H 51 58 possesses
alpha-adrenergic receptor-blocking properties in
addition t o its beta-adrenoceptor-blockingaction,
as would be expected, some postural and exercise
hypotension sometimes occurs when large doses are
used.
References
BEILEN.L.J. & JUEL-JENSEN,
B.E. (1972) Alpha and beta
adrenergic blockade in hypertension. Lancet, i, 979-982.
BOAKES,A.J., KNIGHT.E.J. & PRICHARD,B.N.C. (1971)
Preliminary studies of the pharmacological effects of
5-{1-hydroxy-2-[(l-methyl-3-phenylpropyl) amino]-ethyl)salicylamide (AH 5158) in man. Clinirnl Science, 40, 1 8 ~ .
F.O. (1975)A comparison of a
H I L L ,D.W. & THOMPSON,
non-invasive impedance method and a standard isotopic
method for measuring cardiac output. Eiontedical €ngiiieerinK (in press).
KUBICEK,
W.G., PATTERSON,
R.P. & WITSOE,D.A. (1970)
Impedance cardiography as a non-invasive method of
monitoring cardiac function and other parameters of the
cardiovascular system. Annals of’ the Ncw York Acarleiny
of Sciences,
170, 724-732.
PRICHAKD.
B.N.C. & GILLAM,P.M.S. (1969)Treatment of
hypertension with propranolol. British Meclicnl Joicrnol, i,
7-16.
PRICHARD,
B.N.C., GILLAM,P.M.S. & G R A H A MB.R.
,
(1970)
Beta receptor antagonism in hypertension. Comparison
with the effect of adrenergic neurone inhibition on cardiovascular responses. Internationnl Joiirnol of Clinical
Pharntacology,
4, 131-140.
SIMPSON,F.O. (1974) Beta-adrenergic receptor blocking
drugs in hypertension. Driips, 7, 85-105.
VEAL,N. & VETTER,H. (1965) Rndioisotopc Techniqitcs in
Clinical Research and Diagnosis, p. 350. But terworths,
London.
ZACHARIAS.
F.J., COWEN,K.J., VICKERS.
J. & WALL, B.G.
(1972)Propranolol in hypertension. A study of long term
t hcrapy 1964-1 970. Amcvk-nn Heart Jorirnol, 83, 755-76 I.