Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Albuterol multidose dry powder inhaler and albuterol
hydrofluoroalkane versus placebo in children with
persistent asthma
Y
P
Paul Y. Qaqundah, M.D.,1 Herminia Taveras, Ph.D., M.P.H.,2 Harald Iverson, Ph.D.,3
and Paul Shore, M.D., M.S.4
ABSTRACT
Background: Many children struggle with albuterol hydrofluoroalkane (HFA) inhalers. Albuterol multidose dry powder
inhaler (MDPI) may simplify rescue bronchodilator use in children.
Objective: To demonstrate the comparability of albuterol MDPI and albuterol HFA in children with asthma.
Methods: This phase II, multicenter, double-blind, double-dummy, single-dose, five-period, crossover study randomized
patients (ages 4 –11 years) with persistent asthma and prestudy forced expiratory volume in 1 second (FEV1) of 60 –90% of
predicted to 1 of 10 treatment sequences that contained albuterol MDPI (90 and 180 g), albuterol HFA (90 and 180 g), and
placebo MDPI and placebo HFA. Efficacy was evaluated by measuring the area under the baseline-adjusted percent-predicted
FEV1–time curve over 6 hours (PPFEV1 AUC0 – 6) after dosing. Safety was evaluated by adverse events.
Results: The full analysis set included 61 patients. Albuterol MDPI and albuterol HFA significantly improved PPFEV1
AUC0 – 6 versus placebo (p ⱕ 0.0107). Mean improvement (⫾ standard error [SE]) in PPFEV1 AUC0 – 6 versus placebo with
albuterol MDPI at 90 and 180 g was similar (21.2 ⫾ 4.87 [95% confidence interval {CI}, 11.60 –30.81], and 22.6 ⫾ 4.87
[95% CI, 13.00 –32.20], %䡠hour, respectively). Mean improvement (⫾ SE) with albuterol HFA 180 g was significantly (p ⫽
0.0226) greater versus albuterol HFA 90 g (23.7 ⫾ 4.85 [95% CI, 14.13–33.23], and 12.5 ⫾ 4.85 [95% CI, 2.93–22.05],
%䡠hour, respectively). All doses of albuterol were well tolerated.
Conclusion: Albuterol MDPI 90 and 180 g and albuterol HFA 180 g provided similar and significant FEV1
improvements versus placebo; albuterol HFA 90 g was significant versus placebo but seemed less effective based on absolute
improvements in FEV1. ClinicalTrials.gov identifier: NCT01899144
(Allergy Asthma Proc 37:350 –358, 2016; doi: 10.2500/aap.2016.37.3986)
T
A
O
N
pproximately 6.8 million children in the United
States currently have asthma, a chronic respiratory disorder that causes chest tightness, shortness of
breath, wheezing, and cough as a result of inflammatory and hyperreactive airway obstruction.1–3 Albuterol, a short-acting 2 adrenergic agonist, has a bron-
O
D
From the 1Department of Pediatrics, Hoag Medical Group, Huntington Beach, California, 2Clinical Research and Development, Teva Pharmaceuticals, Miami, Florida,
3
Statistics Department, Teva Pharmaceuticals, Miami, Florida, and 4Clinical Research
and Development, Teva Pharmaceuticals, Frazer, Pennsylvania
This study was sponsored by Teva Branded Pharmaceutical Products R&D, Inc.
Medical writing assistance was provided by Lisa Feder, Ph.D., Peloton Advantage, and
was funded by Teva Branded Pharmaceutical Products R&D, Inc. Teva provided a full
review of the article
H. Taveras and H. Iverson are employees of Teva Pharmaceuticals, Miami, Florida.
P. Shore was an employee of Teva Pharmaceuticals, Frazer, Pennsylvania, at the time
of manuscript preparation. P.Y. Qaqundah has no conflicts of interest pertaining to
this article
Presented in poster format at the American Academy of Allergy, Asthma & Immunology annual scientific meeting, Los Angeles, California, March 4 –7, 2016. A subset
of the data was presented in poster format at the American Thoracic Society International Conference, San Francisco, California, May 13–18, 2016
Address correspondence to Paul Y. Qaqundah, M.D., Hoag Medical Group, 19582
Beach Blvd., Suite 350, Huntington Beach, CA 92648
E-mail address: [email protected]
Published online August 15, 2016
Copyright © 2016, OceanSide Publications, Inc., U.S.A.
350
O
C
chodilatory effect that rapidly reverses acute airflow
obstruction and alleviates the symptoms of an acute
asthma attack.3 The safety and efficacy of long-term
inhaled albuterol use is well documented.4
Until recently, the only available inhaler device for
delivery of albuterol was the metered-dose inhaler
(MDI), which delivers the drug in aerosolized form.
Usage errors with MDIs are common, especially in
children, because these inhalers require the coordination of actuation with inhalation.5,6 Good inhaler technique is an important aspect of asthma control.7 Proper
use of an MDI can be difficult for patients to learn, as
demonstrated by two studies, one of which found that
⬎65% of patients failed to use their MDI correctly even
after instruction8 and another that found that half of
the pediatric patients (55%) enrolled (ages 6 –10 years)
used MDIs improperly.9 The inability to coordinate
manual actuation with inhalation may compromise
drug delivery to the airways, which potentially results
in suboptimal efficacy.6
A novel, inhalation-driven, albuterol multidose dry
powder inhaler (MDPI) that does not require patient
coordination of device actuation with inhalation has
been developed with the goal of reducing administra-
September–October 2016, Vol. 37, No. 5
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
tion errors associated with conventional MDIs. An albuterol MDPI (ProAir RespiClick; Teva Pharmaceuticals, Inc., Frazer, PA), approved in March 2015 by the
U.S. Food and Drug Administration for adolescent and
adult patients with reversible bronchospasm, has been
shown to provide efficacy and safety comparable with
those of an available albuterol hydrofluoroalkane
(HFA) inhaler.10,11 Satisfaction with this device was
recently assessed in an open-label study that included
patients ⱖ4 years of age with asthma or chronic obstructive pulmonary disease: 83% of the patients reported being somewhat to very satisfied with the
MDPI with an integrated dose counter, 92% were satisfied with the ease of holding and handling the inhaler, and 85% were satisfied with the ease of learning
to use the inhaler.12 This article reports on a study that
was designed to demonstrate the comparability of albuterol MDPI and albuterol HFA in children with persistent asthma.
onate per day or equivalent), leukotriene modifiers,
or inhaled cromones, or on 2-agonists alone as
needed, for a minimum of 4 weeks before the screening
visit and with the expectation of maintenance for the
duration of the study. Patients were required to have a
forced expiratory volume in 1 second (FEV1) value of
60 –90% predicted for age, height, and sex, and to demonstrate at least 15% reversibility of FEV1 within 30
minutes after inhalation of 180 g of albuterol. In addition, patients were required to demonstrate an acceptable inhalation technique with both the MDPI and
the HFA, and be able to self-perform spirometry and
peak expiratory flow (PEF) measurements.
METHODS
Y
P
Study Description
This was a phase II, randomized, double-blind, double-dummy, placebo-controlled, single-dose, five-treatment, five-period, ten-sequence, five-way crossover
study of pediatric patients at 14 sites across the United
States (ClinicalTrials.gov identifier: NCT01899144;
study number: ABS-AS-201). The objective of the study
was to demonstrate the comparability of albuterol
MDPI and albuterol HFA for the treatment of persistent asthma in children ages 4 to 11 years.
Ethical Conduct
The study was conducted in accordance with the
International Council for Harmonisation Good Clinical
Practice Consolidation Guideline (E6), and applicable
regulations of the U.S. Code of Federal Regulations
Title 21, Parts 50, 54, 56, 312, and 314, and European
Union Directive 2001/20/EC.13 Before study initiation,
the study protocol was submitted to the appropriate
independent ethics committee or institutional review
board for review and approval. The parents or guardians of all enrolled patients provided written, informed
consent before any study-related procedures, and assent from the patients themselves was obtained when
applicable.
O
D
T
O
N
Inclusion Criteria
Patients who met the following criteria were eligible
for inclusion in the study: boys or premenarchal girls
between the ages of 4 and 11 years (inclusive) as of the
screening visit, in otherwise good health, with a
documented diagnosis of persistent asthma of at
least 6 months’ duration and on stable low-dose
inhaled corticosteroid (ⱕ200 g fluticasone propi-
O
C
Exclusion Criteria
Patients with a known hypersensitivity to albuterol
or any inactive agent in the inhaler formulations, a
history of respiratory infection or disorder that was not
resolved within 4 weeks before the screening visit, an
asthma exacerbation that required oral corticosteroids
within 3 months or hospitalization within 6 months of
the screening visit, an inability to tolerate or unwillingness to comply with the required washout periods,
and/or a history of life-threatening asthma were ineligible for participation in the study. Patients who used
prohibited concomitant medications, were treated with
systemic corticosteroids within 6 weeks of the screening visit, participated in a previous albuterol MDPI
trial at any time, or who received any investigational
drug as part of a trial within 30 days of the screening
visit were also ineligible. Study participants could not
have any nonasthmatic acute or chronic conditions.
Randomization Criteria
The patients were randomized at the first treatment
visit and were permitted to remain in the study if,
before dosing at each treatment visit, they continued to
be in good health, had not experienced any adverse
event (AE) that would prevent further participation,
had not used any prohibited concomitant medications,
had not used rescue albuterol for at least 6 hours before
each treatment visit, and were able to correctly use
each inhaler device. Patient’s FEV1 level had to remain
within 60 –90% of predicted value and ⫾20% of the
study qualifying value measured at the screening visit,
and patients could not have experienced an asthma
exacerbation or upper respiratory tract infection or
received any additional treatment for asthma.
Study Design
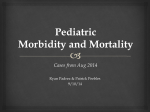
The study design is shown in Fig. 1. Eligible patients
were randomized to 1 of 10 treatment sequences based
on Latin squares that contained single doses of albuterol MDPI 90 g, albuterol MDPI 180 g, albuterol
HFA 90 g, albuterol HFA 180 g, or placebo MDPI
Allergy and Asthma Proceedings
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
351
Figure 1. Study design. FEV1 ⫽
Forced expiratory volume in 1 second;
HFA ⫽ hydrofluoroalkane; MDI ⫽ metered-dose inhaler; MDPI ⫽ multidose
dry powder inhaler.
and placebo HFA (0 g albuterol). The 90 and 180 g
doses of albuterol HFA were chosen because they are
the approved doses in pediatric patients.14 The 90 and
180 g doses of albuterol MDPI were chosen based on
the approved doses of inhaled albuterol HFA in pediatric patients. The intent of the study was to demonstrate the comparability of albuterol MDPI and albuterol HFA inhalers. All the patients received
inhalations from two separate MDPIs (active or placebo) and two separate HFAs (active or placebo) to
deliver the appropriate doses while maintaining
blinding.
After the initial screening visit, each patient received
one of the five treatments at five treatment visits over
the study duration; each treatment visit was separated
by a washout period of between 2 and 7 days. At each
treatment visit, an initial FEV1 was measured at 30
minutes and again just before dispensation of the study
treatment. Additional FEV1 measurements were taken
at 5, 15, 30, 45, 60, 120, 180, 240, 300, and 360 minutes
after treatment. Blood pressure and pulse rate measurements were recorded within 5 minutes before each
FEV1 measurement for up to 4 hours to determine
treatment effects. Patients received paper diaries to
record morning PEF values between treatment visits,
AEs, and the use of rescue medication. Albuterol HFA
inhalers (ProAir HFA; Teva Respiratory, LLC, Horsham, PA) were provided as rescue medication.
O
D
T
O
N
Efficacy
Spirometry was the primary measurement to evaluate study end points. Each center was provided with a
standard spirometer, and site personnel received standardized training. Predicted FEV1 values were computed and adjusted for age, height, and sex for patients
ages 4 to 5 years15 and for patients ages 6 to 11 years16
by using the American Thoracic Society/European
Thoracic Society criteria applicable to pediatric patients.17 Serial FEV1 measurements (the highest of three
acceptable maneuvers) were obtained at 5, 15, 30, 45,
60, 120, 180, 240, 300, and 360 minutes after the
completion of study drug administration at each
treatment visit. The primary efficacy end point was
the baseline-adjusted area under the percentpredicted FEV1-versus-time curve over 6 hours
(PPFEV1 AUC0 – 6 [%䡠hour]) after treatment.
352
Y
P
The baseline-adjusted area under the FEV1-versustime curve over 6 hours (FEV1 AUC0 – 6 [L䡠hour]) after
treatment was the secondary efficacy end point. Additional efficacy end points included baseline-adjusted
maximum FEV1 and maximum PPFEV1 values within
6 hours after treatment; time, in minutes, to increases
of at least 15% and 12% in baseline PPFEV1 in patients
within 30 minutes after treatment; duration, in hours,
of 15% and 12% responses for those patients who responded within 30 minutes; response rate based on
ⱖ15% and ⱖ12% increases in baseline PPFEV1 within
30 minutes after treatment; and time, in minutes, to
maximum PPFEV1.
O
C
Safety
Safety assessments included tabulation of AEs and
serious AEs (SAEs), including severity and relationship to study drug; SAEs were defined as AEs that
resulted in death, life-threatening events, events that
required or prolonged hospitalization, persistent or
significant disability or incapacity, or congenital abnormality or birth defect. Other safety assessments included laboratory evaluations, physical examination
findings, and a 12-lead electrocardiogram result. Vital
signs were documented, which coincided with FEV1
measurement intervals for up to 4 hours after dosing at
each treatment visit.
Statistics
The intent-to-treat (ITT) population included all randomized patients based on the treatment initially assigned, regardless of the treatment received. All patients in the ITT population who had a baseline
assessment at the screening visit and received at least
one dose of the study medication with at least one
postbaseline assessment were included in the full analysis set, which was the primary analysis set for efficacy
parameters. The per-protocol population consisted of
all randomized patients who had no major protocol
violations determined before unblinding and served as
the supportive population. The safety population included all patients in the ITT population who received
at least one dose of the study medication.
The primary statistical tool was the mixed-effect
analysis of variance with fixed effects of sequence,
September–October 2016, Vol. 37, No. 5
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
treatment group, and period; and the random effect for
the patient within sequence. An appropriate contrast
was derived from this model for the following comparison of interest with respect to the primary efficacy
variable, PPFEV1 AUC0 – 6 (%䡠hour): the mean difference between each active group and placebo at each
dose level, tested in a sequential manner. The sequential order of comparisons was albuterol MDPI 180 g
with placebo, albuterol MDPI 90 g with placebo, albuterol HFA 180 g with placebo, and albuterol HFA
90 g with placebo. Each test was two-sided and done
at the 0.05 level of significance. However, if a test was
not significant at this level, no further tests were done.
This sequential manner of performing the tests ensured
that the overall alpha level for the entire series was not
⬎0.05.
Table 1 Patient demographics and baseline clinical
characteristics (ITT population) (N ⴝ 61)
RESULTS
Sex, no. (%)
Boys
Girls
Age, mean ⫾ SD, y
Race, no. (%)
White
Black
Other
Height, mean ⫾ SD, cm
Weight, mean ⫾ SD, kg
BMI, mean ⫾ SD, kg/m2
Duration of asthma, no. (%)
6 mo to ⬍1 y
1 to ⬍5 y
5 to ⬍10 y
10 to ⬍15 y
Airway reversibility, mean ⫾ SD, %
Baseline PPFEV1, mean ⫾ SD, %
Patients
Of the 102 patients, ages 4 to 11 years, who were
screened for inclusion in the study, 33 did not meet
inclusion criteria, 3 were lost to follow-up, 1 withdrew
consent, and 4 did not pass the screening for other
causes, which resulted in 61 patients who met the
eligibility criteria and were randomized into the study.
All 61 enrolled patients were assessable for efficacy
and safety. The per-protocol analysis included 56 patients, and 57 of the 61 enrolled patients completed the
study. A total of four patients (7%) withdrew from the
study, all for other reasons (erroneously randomized at
treatment visit 1; did not meet FEV1 criteria; package
insert discretion; did not meet ⬍20% change in FEV1
from qualifying value at screening at treatment visit 2
after 3 attempts). No patients died or discontinued due
to AEs. Patient demographics and baseline clinical
characteristics are summarized in Table 1. All patients
had asthma that was diagnosed at least 6 months before participation in the study, and eight patients had a
ⱖ10-year history of asthma. Most of the patients had
no previous experience with a dry powder inhaler, and
only one patient had no experience with an MDI.
O
D
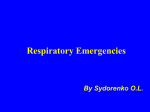
Efficacy
Baseline-adjusted PPFEV1 AUC0 – 6 was significantly
greater in all active treatment groups compared with
patients who received placebo (p ⱕ 0.0107) (Table 2
and Fig. 2). The patients treated with albuterol MDPI
90 g and 180 g had similar increases in PPFEV1
AUC0 – 6 (Table 2), whereas patients treated with albuterol HFA 180 g had significantly greater PPFEV1
AUC0 – 6 than those treated with albuterol HFA 90 g
(p ⫽ 0.0226) (Table 2). Similar patterns were seen in
baseline-adjusted FEV1 AUC0 – 6, maximum FEV1 value
over 6 hours, and maximum PPFEV1 over 6 hours after
treatment (Table 3). The mean and median times to
O
C
Y
P
28 (46)
29 (48)
4 (7)
138.7 ⫾ 10.2
38.2 ⫾ 12.8
19.5 ⫾ 4.35
1 (2)
22 (36)
30 (49)
8 (13)
24.1 ⫾ 10.2
72.9 ⫾ 7.2
ITT ⫽ Intent-to-treat; SD ⫽ standard deviation; BMI ⫽
body mass index; PPFEV1 ⫽ percent-predicted forced expiratory volume in 1 second.
T
O
N
38 (62)
23 (38)
9 ⫾ 1.6
12% and 15% response onset among patients who had
such responses were comparable between patients
treated with albuterol MDPI and those who received
albuterol HFA (Table 4).
All active treatments resulted in a shorter time to
maximum PPFEV1 (⬃45 to 50 minutes) compared with
patients who received placebo; no difference was noted
between the 90 and 180 g doses for either albuterol
MDPI or albuterol HFA (Table 4). Based on a ⱖ15%
increase in FEV1 over baseline within 30 minutes after
dosing, all active groups had significantly higher response rates than placebo (response rate, 17%; p ⱕ
0.0119), although the response rate with albuterol
MDPI (45– 46%) was somewhat greater than the rate
for albuterol HFA 90 g (37%) or albuterol HFA 180 g
(41%) (Table 4). Using a threshold of ⱖ12% increase in
FEV1 value from baseline within 30 minutes of dosing,
the response rate was greater than for placebo in all
active groups but highest for albuterol MDPI (57–58%
for albuterol MDPI; 54% for albuterol HFA 90 g; 47%
for albuterol HFA 180 g versus 20% for placebo; p ⱕ
0.0007) (Table 4).
Safety
There were no deaths or SAEs, and no withdrawals
due to AEs. There were two reported AEs after treatment with albuterol MDPI 180 g (otitis media and
urticaria), and there were no AEs associated with albuterol MDPI 90 g. Six AEs were reported by five
patients after treatment with albuterol HFA 90 g,
Allergy and Asthma Proceedings
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
353
Table 2 Primary efficacy end point, baseline-adjusted PPFEV1 AUC0 – 6 (%䡠hr) (full analysis set)
n
Mean ⫾ SE
95% CI
Active–placebo
Mean ⫾ SE
95% CI
p Value
90 g–180 g
Mean ⫾ SE
95% CI
p Value
Placebo
(N ⴝ 61)
Albuterol MDPI
90 g (N ⴝ 61)
Albuterol MDPI
180 g (N ⴝ 61)
Albuterol HFA
90 g (N ⴝ 61)
Albuterol HFA
180 g (N ⴝ 61)
59
25.4 ⫾ 6.25
12.94–37.81
58
46.6 ⫾ 6.27
34.13–59.07
59
48.0 ⫾ 6.24
35.56–60.39
59
37.9 ⫾ 6.25
25.43–50.30
59
49.1 ⫾ 6.26
36.61–61.50
21.2 ⫾ 4.87
11.62–30.81
⬍0.0001
22.6 ⫾ 4.87
13.00–32.20
⬍0.0001
12.5 ⫾ 4.85
2.93–22.05
0.0107
⫺1.4 ⫾ 4.88
⫺11.00 to 8.23
0.7772
O
C
Y
P
23.7 ⫾ 4.85
14.13–33.23
⬍0.0001
⫺11.2 ⫾ 4.87
⫺20.80 to ⫺1.59
0.0226
PPFEV1 ⫽ Percent-predicted forced expiratory volume in 1 second; AUC0 – 6 ⫽ area under the curve over 6 hr; MDPI ⫽
multidose dry powder inhaler; HFA ⫽ hydrofluoroalkane; SE ⫽ standard error; CI ⫽ confidence interval.
including headache, constipation, diarrhea, and pyrexia. One patient reported upper abdominal pain after
treatment with albuterol HFA 180 g, and one case of
viral gastritis was reported in a patient who received
placebo. There were no clinically significant effects on
vital signs or other safety parameter findings.
O
D
T
O
N
DISCUSSION
In this phase II, single-dose, five-way crossover
study, children with asthma treated with albuterol
MDPI and with albuterol HFA, each at dosages of 90
and 180 g, experienced significant improvements in
baseline-adjusted PPFEV1 AUC0 – 6 (the primary efficacy end point) compared with the patients who
received placebo. The magnitude of effect was similar in patients treated with albuterol MDPI 90 g
and 180 g, whereas improvement from baseline
was greater in patients treated with albuterol HFA
180 g compared with albuterol HFA 90 g; PPFEV1
AUC0 – 6 in the albuterol HFA 180 g group was
similar to that observed in both the albuterol MDPI
90 g and 180 g groups. This pattern was repeated
for most of the secondary end points as well. Time to
onset and duration of effect, whether measured by
ⱖ12% or ⱖ15% response, were similarly greater than
placebo with all active treatments. Both albuterol
MDPI and albuterol HFA were generally well tolerated, with no SAEs or study withdrawals due to
AEs.
In a similar randomized, double-blind, placebo-controlled, single-dose, five-way crossover study, 71 adult
patients were treated with albuterol MDPI 90 g, albuterol MDPI 180 g, albuterol HFA 90 g, albuterol
HFA 180 g, or placebo.11 Although similar to the
present study in that patients in all active treatment
groups experienced significant (p ⬍ 0.0001) improvements from baseline in PPFEV1 AUC0 – 6, the adult
study differed from the pediatric study in that there
was no difference between the response of the adult
patients treated with albuterol HFA 90 g and albu-
Figure 2. Mean percent-predicted FEV1 by treatment
and time point (full analysis set). FEV1 ⫽ Forced expiratory volume in 1 second; HFA ⫽ hydrofluoroalkane;
MDPI ⫽ multidose dry powder inhaler.
354
September–October 2016, Vol. 37, No. 5
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
Table 3 Additional efficacy end points (full analysis set)
Allergy and Asthma Proceedings
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
59
0.48 ⫾ 0.14
0.20–0.76
0.40 ⫾ 0.10
0.21–0.59
⬍0.0001
58
0.88 ⫾ 0.14
0.60–1.16
Albuterol MDPI 90
g (N ⴝ 61)
59
9.83 ⫾ 1.15
7.53–12.12
59
0.19 ⫾ 0.02
0.14–0.24
0.09 ⫾ 0.02
0.05–0.12
⬍0.0001
58
0.27 ⫾ 0.02
0.23–0.32
⫺0.01 ⫾ 0.02
⫺0.04 to 0.02
0.5421
0.10 ⫾ 0.02
0.06–0.13
⬍0.0001
59
0.28 ⫾ 0.02
0.24–0.33
⫺0.05 ⫾ 0.10
⫺0.23 to 0.14
0.6342
4.88 ⫾ 0.85
3.20–6.57
⬍0.0001
4.38 ⫾ 0.85
2.70–6.06
⬍0.0001
⫺0.50 ⫾ 0.86
⫺2.19 to 1.18
0.5578
59
14.71 ⫾ 1.15
12.42–17.00
58
14.21 ⫾ 1.16
11.91–16.51
3.38 ⫾ 0.85
1.70–5.06
⬍0.0001
59
13.21 ⫾ 1.15
10.91–15.50
0.07 ⫾ 0.02
0.04–0.10
⬍0.0001
59
0.26 ⫾ 0.02
0.21–0.31
0.26 ⫾ 0.10
0.08–0.45
0.0062
⫺1.76 ⫾ 0.85
⫺3.44 to ⫺0.08
0.0407
5.14 ⫾ 0.85
3.47–6.81
⬍0.0001
59
14.97 ⫾ 1.15
12.67–17.26
⫺0.03 ⫾ 0.02
⫺0.06 to 0.00
0.0688
0.10 ⫾ 0.02
0.07–0.14
⬍0.0001
59
0.29 ⫾ 0.02
0.24–0.34
⫺0.19 ⫾ 0.10
⫺0.38 to 0.00
0.0488
0.45 ⫾ 0.10
0.26–0.64
⬍0.0001
59
0.93 ⫾ 0.14
0.65–1.21
59
0.74 ⫾ 0.14
0.46–1.02
59
0.93 ⫾ 0.14
0.65–1.20
0.45 ⫾ 0.10
0.26–0.64
⬍0.0001
Albuterol HFA 180
g (N ⴝ 61)
Albuterol HFA 90
g (N ⴝ 61)
Albuterol MDPI 180
g (N ⴝ 61)
MDPI ⫽ Multidose dry powder inhaler; HFA ⫽ hydrofluoroalkane; FEV1 ⫽ forced expiratory volume in 1 second; AUC0 – 6 ⫽ area under the curve over 6 hours;
SE ⫽ standard error; CI ⫽ confidence interval.
Baseline-adjusted FEV1 AUC0–6 (L䡠hr):
secondary efficacy end point
No. patients
Mean ⫾ SE
95% CI
Active–placebo
Mean ⫾ SE
95% CI
p Value
90 g–180 g
Mean ⫾ SE
95% CI
p Value
Baseline-adjusted maximum FEV1 over 6 hr, L
No. patients
Mean ⫾ SE
95% CI
Active–placebo
Mean ⫾ SE
95% CI
p Value
90 g–180 g
Mean ⫾ SE
95% CI
p Value
Baseline-adjusted maximum percent-predicted
FEV1 over 6 hr, %
No. patients
Mean ⫾ SE
95% CI
Active–placebo
Mean ⫾ SE
95% CI
p Value
90 g–180 g
Mean ⫾ SE
95% CI
p Value
Placebo
(N ⴝ 61)
O
D
O
N
T
O
C
Y
P
355
356
Response rate based on 15% increase in baseline
PPFEV1 within 30 min
Responders, no. (%)
Model estimated rate ⫾ SE
95% CI
Difference from placebo ⫾ SE
95% CI
p Value
Response rate based on 12% increase in baseline
PPFEV1 within 30 min
Responders, no. (%)
Model estimated rate ⫾ SE
95% CI
Difference from placebo ⫾ SE
95% CI
p Value
Time (min) to 15% response among responders
within 30 min
No. patients
Mean ⫾ SD
Median
Min, max
Time (min) to 12% response among responders
within 30 min
No. patients
Mean ⫾ SD
Median
Min, max
Time (min) to maximum PPFEV1 over 6 hr
No. patients
Mean
p Value vs placebo
p Value 90 g vs 180 g
Duration (hr) of 15% response among
responders within 30 min
No. patients
Mean ⫾ SD
10 (17.0)
0.10 ⫾ 0.04
0.01–0.18
Placebo
(N ⴝ 61)
26 (44.8)
0.43 ⫾ 0.09
0.24–0.61
0.33 ⫾ 0.09
0.15–0.51
0.0006
Albuterol MDPI
90 g (N ⴝ 61)
33 (56.9)
0.59 ⫾ 0.09
0.43–0.76
0.45 ⫾ 0.09
0.27–0.64
⬍0.0001
26
10.7 ⫾ 4.79
8.8
4.8, 18.5
33
11.9 ⫾ 7.20
8.9
3.1, 29.9
58
47.6
0.0130
—
26
2.8 ⫾ 2.37
—
—
—
—
—
—
—
—
59
75.9
—
—
—
—
12 (20.3)
0.14 ⫾ 0.05
0.04–0.24
27
10.4 ⫾ 6.96
8.0
4.7, 29.7
27
3.0 ⫾ 2.29
59
45.0
0.0054
0.7667
34
9.9 ⫾ 6.10
8.1
4.7, 29.7
22
2.4 ⫾ 2.21
59
50.1
0.0265
—
32
9.1 ⫾ 5.28
8.1
4.0, 29.4
22
9.4 ⫾ 5.41
8.4
4.0, 26.6
32 (54.2)
0.55 ⫾ 0.09
0.37–0.72
0.41 ⫾ 0.09
0.22–0.59
⬍0.0001
24
2.8 ⫾ 2.48
59
44.7
0.0048
0.5363
28
9.7 ⫾ 5.70
8.3
4.1, 27.2
24
12.8 ⫾ 7.88
8.4
4.2, 28.7
28 (47.5)
0.47 ⫾ 0.09
0.29–0.64
0.33 ⫾ 0.09
0.14–0.51
0.0007
24 (40.7)
0.37 ⫾ 0.09
0.19–0.54
0.27 ⫾ 0.09
0.10–0.45
0.0027
22 (37.3)
0.30 ⫾ 0.08
0.14–0.47
0.21 ⫾ 0.08
0.05–0.37
0.0119
27 (45.8)
0.43 ⫾ 0.09
0.25–0.62
0.34 ⫾ 0.09
0.15–0.52
0.0005
34 (57.6)
0.60 ⫾ 0.08
0.43–0.77
0.46 ⫾ 0.09
0.28–0.64
⬍0.0001
Albuterol HFA 180
g (N ⴝ 61)
Albuterol HFA
90 g (N ⴝ 61)
Albuterol MDPI 180
g (N ⴝ 61)
Table 4 Response rates, time to response, and duration of response of albuterol MDPI versus albuterol HFA (full analysis set)
O
D
O
N
T
O
C
Y
P
September–October 2016, Vol. 37, No. 5
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
MDPI ⫽ Multidose dry powder inhaler; HFA ⫽ hydrofluoroalkane; PPFEV1 ⫽ percent-predicted forced expiratory volume in 1 second; SE ⫽ standard error; CI ⫽
confidence interval; SD ⫽ standard deviation; min ⫽ minimum; max ⫽ maximum.
28
3.0 ⫾ 2.49
3.5
0.2, 5.9
32
2.7 ⫾ 2.35
2.3
0.2, 5.9
34
3.3 ⫾ 2.18
3.8
0.1, 5.9
33
3.2 ⫾ 2.24
3.7
0.1, 5.9
—
—
—
—
2.3
0.2, 5.9
1.9
0.2, 5.9
2.9
0.1, 5.9
2.8
0.2, 5.9
—
—
Albuterol HFA 180
g (N ⴝ 61)
Albuterol HFA
90 g (N ⴝ 61)
Albuterol MDPI 180
g (N ⴝ 61)
Albuterol MDPI
90 g (N ⴝ 61)
Placebo
(N ⴝ 61)
Y
P
O
C
CONCLUSION
In this study in children ages 4 to 11 years, albuterol
MDPI was significantly more effective than placebo
across all study end points and had similar safety and
efficacy compared with albuterol HFA. Significant improvements in baseline-adjusted PPFEV1 AUC0 – 6 were
observed with albuterol MDPI 90 g and 180 g in
pediatric patients compared with patients who received placebo. Data from this clinical trial were reviewed by the U.S. Food and Drug Administration in
their evaluation and, in April 2016, approval of the
expanded indication for treatment of patients 4 years
of age and older.
T
O
N
Median
Min, max
Duration (hr) of 12% response among
responders within 30 min
No. patients
Mean ⫾ SD
Median
Min, max
Table 4 Continued
O
D
terol HFA 180 g. In addition, an exploratory analysis
indicated that improvements in mean FEV1 AUC0 – 6 in
patients treated with albuterol MDPI and albuterol
HFA were not significantly different at both the 90and 180-g dosages.
Similar to the present study, albuterol dry powder
inhalers have been demonstrated to be safe, effective, and easy to use for children with persistent
asthma.18 –20 Kemp et al.18 performed dose-ranging and
12-week efficacy and safety studies that compared
aerosol and powder albuterol with placebo, and both
studies showed similar efficacy and safety profiles between the two formulations.
Limitations of this study included the single-dose
design, the small patient numbers, and the lack of
patient-preference questionnaires to assess inhaler
preferences. The strengths of this study included the
crossover design, the double-blind, double-dummy
dosing, and the high rate of study completion achieved
(57 of the 61 enrolled patients completed the study).
REFERENCES
1.
2.
3.
4.
5.
6.
7.
FastStats—Asthma. Updated: May 14, 2015. Centers for Disease
Control and Prevention. Available online at http://www.cdc.
gov/nchs/fastats/asthma.htm; accessed August 13, 2015.
Albuterol oral inhalation. Updated: September 1, 2010.
MedlinePlus. Available online at http://www.nlm.nih.gov/
medlineplus/druginfo/meds/a682145.html; accessed January 29, 2016.
Expert Panel Report 3 (EPR3): Guidelines for the Diagnosis and
Management of Asthma. Bethesda, MD: National Heart, Lung,
and Blood Institute, U.S. Department of Health and Human
Services, 2007.
Ramsdell JW, Klinger NM, Ekholm BP, and Colice GL. Safety of
long-term treatment with HFA albuterol. Chest 115:945–951, 1999.
Burkhart PV, Rayens MK, and Bowman RK. An evaluation of
children’s metered-dose inhaler technique for asthma medications. Nurs Clin North Am 40:167–182, 2005.
Levy ML, Hardwell A, McKnight E, and Holmes J. Asthma
patients’ inability to use a pressurised metered-dose inhaler
(pMDI) correctly correlates with poor asthma control as defined
by the Global Initiative for Asthma (GINA) strategy: A retrospective analysis. Prim Care Respir J 22:406 – 411, 2013.
Baddar S, Jayakrishnan B, and Al-Rawas OA. Asthma control:
Importance of compliance and inhaler technique assessments.
J Asthma 51:429 – 434, 2014.
Allergy and Asthma Proceedings
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm
357
8.
9.
10.
11.
12.
13.
14.
Hardwell A, Barber V, Hargadon T, et al. Technique training does
not improve the ability of most patients to use pressurised metered-dose inhalers (pMDIs). Prim Care Respir J 20:92–96, 2011.
Scarfone RJ, Capraro GA, Zorc JJ, and Zhao H. Demonstrated
use of metered-dose inhalers and peak flow meters by children
and adolescents with acute asthma exacerbations. Arch Pediatr
Adolesc Med 156:378 –383, 2002.
ProAir RespiClick [package insert]. Horsham, PA: Teva Respiratory, 2016.
Kerwin EM, Taveras H, Iverson H, et al. Pharmacokinetics, pharmacodynamics, efficacy, and safety of albuterol (salbuterol) multidose dry-powder inhaler and ProAir® hydrofluoroalkane for the
treatment of persistent asthma: Results of two randomized double-blind studies. Clin Drug Investig 36:55– 65, 2016.
Given J, Taveras H, and Iverson H. Prospective, open-label evaluation of a new albuterol multidose dry powder inhaler with
integrated dose counter. Allergy Asthma Proc 37:199 –206, 2016.
Guidance for Industry E6 Good Clinical Practice: Consolidated
Guidance. Rockville, MD: U.S. Department of Health and Human Services, Food and Drug Administration, 1996.
ProAir HFA [package insert]. Horsham, PA: Teva Respiratory,
LLC, 2012.
15.
16.
17.
18.
19.
20.
Eigen H, Bieler H, Grant D, et al. Spirometric pulmonary function in healthy preschool children. Am J Respir Crit Care Med
163:619 – 623, 2001.
Quanjer PH, Borsboom GJ, Brunekreef B, et al. Spirometric
reference values for white European children and adolescents: Polgar revisited. Pediatr Pulmonol 19:135–142, 1995.
Beydon N, Davis SD, Lombardi E, et al. An official American
Thoracic Society/European Respiratory Society statement: Pulmonary function testing in preschool children. Am J Respir Crit
Care Med 175:1304 –1345, 2007.
Kemp JP, Furukawa CT, Bronsky EA, et al. Albuterol treatment for children with asthma: A comparison of inhaled
powder and aerosol. J Allergy Clin Immunol 83:697–702,
1989.
Goren A, Noviski N, Avital A, et al. Assessment of the ability of
young children to use a powder inhaler device (Turbuhaler).
Pediatr Pulmonol 18:77– 80, 1994.
Hagmolen of ten Have W, van de Berg NJ, Bindels PJ, et al.
Assessment of inhalation technique in children in general practice: Increased risk of incorrect performance with new device.
J Asthma 45:67–71, 2008.
e
T
O
D
358
Y
P
O
C
O
N
September–October 2016, Vol. 37, No. 5
Delivered by Ingenta to: ? IP: 5.10.31.211 On: Sun, 18 Jun 2017 07:54:11
Copyright (c) Oceanside Publications, Inc. All rights reserved.
For permission to copy go to https://www.oceansidepubl.com/permission.htm