Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Chagas disease wikipedia , lookup
Toxoplasmosis wikipedia , lookup
Hookworm infection wikipedia , lookup
Anaerobic infection wikipedia , lookup
Onchocerciasis wikipedia , lookup
Herpes simplex virus wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Herpes simplex wikipedia , lookup
Clostridium difficile infection wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Leptospirosis wikipedia , lookup
Cross-species transmission wikipedia , lookup
Henipavirus wikipedia , lookup
West Nile fever wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Trichinosis wikipedia , lookup
Sarcocystis wikipedia , lookup
Dirofilaria immitis wikipedia , lookup
Marburg virus disease wikipedia , lookup
Gastroenteritis wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Schistosomiasis wikipedia , lookup
Rotaviral gastroenteritis wikipedia , lookup
Hepatitis C wikipedia , lookup
Neonatal infection wikipedia , lookup
Oesophagostomum wikipedia , lookup
Coccidioidomycosis wikipedia , lookup
Lymphocytic choriomeningitis wikipedia , lookup
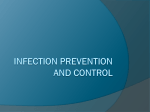
American Journal of Epidemiology © The Author 2016. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: [email protected]. Vol. 183, No. 6 DOI: 10.1093/aje/kwv234 Advance Access publication: March 2, 2016 Practice of Epidemiology Incorporating Transmission Into Causal Models of Infectious Diseases for Improved Understanding of the Effect and Impact of Risk Factors Stuart Paynter* * Correspondence to Dr. Stuart Paynter, Level 2 Public Health Building, School of Public Health, Curtin University, Kent Street, Bentley, WA 6102, Australia (e-mail: [email protected]). Initially submitted March 12, 2015; accepted for publication August 26, 2015. Conventional measures of causality (which compare risks between exposed and unexposed individuals) do not factor in the population-scale dynamics of infectious disease transmission. We used mathematical models of 2 childhood infections (respiratory syncytial virus and rotavirus) to illustrate this problem. These models incorporated 3 causal pathways whereby malnutrition could act to increase the incidence of severe infection: increasing the proportion of infected children who develop severe infection, increasing the children’s susceptibility to infection, and increasing infectiousness. For risk factors that increased the proportion of infected children who developed severe infection, the population attributable fraction (PAF) calculated conventionally was the same as the PAF calculated directly from the models. However, for risk factors that increased transmission (by either increasing susceptibility to infection or increasing infectiousness), the PAF calculated directly from the models was much larger than that predicted by the conventional PAF calculation. The models also showed that even when conventional studies find no association between a risk factor and an outcome, risk factors that increase transmission can still have a large impact on disease burden. For a complete picture of infectious disease causality, transmission effects must be incorporated into causal models. communicable diseases; epidemiologic measurements; epidemiologic methods Abbreviations: IR, incidence rate; PAF, population attributable fraction; RR, rate ratio; RSV, respiratory syncytial virus. epidemiologic studies compare risks between individuals, using the unexposed group as the reference. However, for infectious diseases that are transmitted from person to person, the incidence in the unexposed group depends on the incidence in the exposed group (2, 3). Thus, a population-level perspective is required to fully understand infectious disease causality. When considering infectious diseases, causal effects can be divided into individual-level effects (also called direct effects), which can be detected using conventional methods comparing individuals, and transmission effects (also called indirect effects), which require specific methods to detect. Risk factors that increase infectiousness will have transmission effects, leading to an increased incidence of infection in the whole population. A risk factor that increases the probability of having an infectious contact, or that increases susceptibility to infection following contact with an infectious case, will have both an individual-level effect (because persons Infectious diseases remain the most important cause of morbidity and mortality in the world’s most vulnerable populations, particularly children. Most child deaths due to infectious diseases occur in low- and middle-income settings, where children are particularly at risk because of exposure to environmental risk factors such as malnutrition, poor sanitation, overcrowding, and indoor smoke. (Throughout this article, the term “exposure” refers to exposure to risk factors such as these, as distinct from “contact,” which refers to exposure to the pathogen itself.) Maintaining the momentum of recent gains in child survival will require renewed focus on infectious disease control, which in turn must include interventions designed to address major risk factors (1). For noninfectious diseases, the risk of disease is only increased in persons exposed to a risk factor. For infectious diseases, risk factors that increase the amount of transmission in the population will also increase the risk of infection in persons who are not exposed to that risk factor. Conventional 574 Am J Epidemiol. 2016;183(6):574–582 Incorporating Transmission Into Causal Models 575 exposed to the risk factor will have an increased risk of infection) and a transmission effect (because these additional cases will be infectious). Halloran and Struchiner (2) have demonstrated that individual and transmission effects can be examined in isolation by measuring the effect of a risk factor while conditioning on contact with an infectious source. This can be done by using data from household transmission studies, examining secondary attack rates following the occurrence of an index case of infection in the household. Susceptibility to infection can be assessed by focusing on secondary attack rates in family members who are exposed or unexposed to the risk factor, and the degree of infectiousness can be assessed by focusing on secondary attack rates according to whether the index case is exposed or unexposed to the risk factor. In this paper, I take their work a step further, exploring the impact of risk factors on infectious disease incidence at the population level, by incorporating both individual and transmission effects of a risk factor into mathematical models. The resulting dynamic causal models are referred to here as causal transmission models. Although mathematical models of infectious diseases are used regularly to assess the impact of interventions, they have only rarely been used to investigate the impact of environmental risk factors on infectious disease incidence (4). The models examined in this paper incorporate the effects of malnutrition on the incidence of childhood infection with respiratory syncytial virus (RSV) and rotavirus. Together these two infections are responsible for approximately 1 in 9 infant deaths worldwide (5). Malnourished children have poorer outcomes than well-nourished children following contact with an infectious case: Malnourished children have more symptomatic infections and have more severe infections, with longer duration and higher case fatality rates (6–10). Higher rates of symptomatic infections in malnourished children, exacerbated by longer infectious periods, will act to increase the force of infection acting on all children in the community. METHODS Model structure The same model structure can be used to describe the transmission of either RSV or rotavirus infection. Although these infections are spread by different routes (by respiratory droplets and fecal-oral transmission, respectively), they are both transmitted by close person-to-person contact, as well as by indirect contact through survival of virus on surfaces. To more clearly illustrate the concepts examined in this paper, I used a simplified model with only 2 categories of nutritional status—children are either well-nourished (W) or malnourished (M). The structure of the causal transmission model is outlined in Figure 1, which shows the model compartments for persons in the malnourished subgroup; the compartments for the well-nourished subgroup are equivalent. Individuals are born susceptible (compartments SM and SW) and have a risk of infectious contact of λ per day (the force of infection, which is dependent on the number of infectious individuals). Only a proportion (αM in malnourished children and αW in well-nourished children) of the children who have an infectious contact will become infected (comAm J Epidemiol. 2016;183(6):574–582 EM SM M M Scenario B RM VM Scenario C IM CM M Scenario A Figure 1. Structure of a causal model of childhood infection transmission. The model compartments of the malnourished subgroup are shown; the compartments of the well-nourished subgroup are equivalent. The parameters λα, σ, ν, and γ denote the rate of movement between model compartments. The causal mechanism of malnutrition in each scenario is shown by the open arrows. In scenario A, the proportion of infectious children who develop severe infection is increased among malnourished children (ρM > ρW). In scenario B, susceptibility to infection is increased among malnourished children (αM > αW). In scenario C, malnourished children are infectious for a longer period of time (νM < νW). Notation: C, severe infection (epidemiologic case); E, infected; I, infectious; R, recovered (temporarily immune); S, susceptible. partments EM and EW). After the latency period (the mean latency period is equal to 1/σ), these infected individuals become infectious (compartments IM and IW). The mean infectious period (time in compartment IM or IW) in malnourished children is equal to 1/νM, and in well-nourished children it is equal to 1/νW. Children in compartments RM and RW are temporarily resistant to reinfection, and they return to the susceptible state following a mean period equal to 1/γ. A proportion of infectious children (ρM in malnourished children and ρW in well-nourished children) progress to more severe infection and are identified as epidemiologic cases (subsets CM and CW — note that these are not separate model compartments but are subsets of IM and IW). For RSV, subset C represents severe acute lower respiratory infection, while for rotavirus, subset C represents severe diarrhea requiring hospital admission. For simplicity (and to better demonstrate the difference between individual and transmission effects), persons in subset C are considered to be as infectious per day as any other individual within compartment I. The model equations and the process of model fitting are described in detail in Web Appendix 1 and Web Tables 1–3 (available at http://aje.oxfordjournals.org/). The model parameter assumptions are summarized in Web Tables 1 and 2. The RSV model was fitted to RSV hospital admissions data from the Philippines (11). The rotavirus model was fitted to rotavirus infection data from Guinea-Bissau (12) and again to rotavirus hospital admissions data from India (13). To ensure that the models realistically reflected the actual force of infection in these settings, the models were simultaneously fitted to estimates of the overall rate of infection and the mean force of infection in each setting (Web Table 3). 576 Paynter For each of the infections, 3 scenarios were modeled, each scenario making different assumptions about the mechanisms leading to an increased risk of incident acute lower respiratory infection in malnourished children. The scenarios were chosen to highlight the difference between individual and transmission effects. In reality, these scenarios are unlikely to occur in isolation (e.g., children with more severe disease generally have longer infectious periods). Scenario A: In this scenario, malnutrition increases the risk of progression to more serious infection; however, malnutrition does not alter the child’s susceptibility to infection upon contact with an infectious case or alter the infectiousness of cases. For the RSV model, the risk of progression to severe acute lower respiratory infection in malnourished children is 1.30 times higher than in well-nourished children (ρM = 0.065, ρW = 0.050), and for the rotavirus model the risk of progression to severe diarrhea in malnourished children is similarly 1.33 times higher than in well-nourished children (ρM = 1/45, ρW = 1/60). Cohort monitoring suggests that between 5% and 8% of children with RSV infection develop severe acute lower respiratory infection, while between 1/40 and 1/65 of children with rotavirus infection develop disease severe enough to be admitted to a hospital (14–17). The ratio between ρM and ρW in the models assumes that the association between malnutrition and RSV and diarrhea incidence seen in epidemiologic studies (8, 18–21) is due to an increase in disease progression in malnourished children (i.e., that scenario A is true). Scenario B: In this scenario, malnutrition increases susceptibility to infection, increasing the risk of infection in children who have had contact with an infectious case. However, malnutrition has no effect on the infectiousness of cases or on progression to severe infection. For the reasons described in the Introduction, it is difficult to directly measure how much malnutrition increases susceptibility to infection (i.e., the ratio αM/αW) using conventional epidemiologic studies. Thus, the ratio αM/αW was estimated from the model, by fitting the model while holding the incidence rate ratio (RRI) equal to 1.3 (RRI is the ratio of the incidence rate of infection in malnourished children to the incidence rate in well-nourished children). The value of RRI in the models assumes that the association between malnutrition and RSV and diarrhea incidence seen in epidemiologic studies (8, 18–21) is due to an increase in susceptibility to infection in malnourished children (i.e., that scenario B is true). Scenario C: In this scenario, malnourished children have a prolonged duration of infectiousness; however, malnutrition has no effect on susceptibility to infection or on the progression to severe infection. For both the RSV and rotavirus models, the duration of infectiousness is 1.3 times longer in malnourished children. For RSV, 1/νM = 6.5 days and 1/νW = 5 days. For rotavirus, 1/νM = 9 days and 1/νW = 7 days. These parameter assumptions are consistent with available data (9, 20, 22–24). For each of the 3 scenarios outlined above, the incidence rate (IR) of infection in the malnourished and well-nourished groups (IRIM and IRIW) and the incidence rates of severe infection in the malnourished and well-nourished groups (IRCM and IRCW) were calculated for the baseline situation (20% malnutrition), and then IRIW and IRCW were calculated for the counterfactual situation (no malnutrition). Several degrees of mixing between malnourished and well-nourished children were examined, where the degree of mixing (δ) is the proportion of the malnourished subgroup “allowed” to mix with the well-nourished subgroup, and vice versa. Calculation of relative risks and population attributable fractions Two incidence rate ratio measures were calculated. RRI is the incidence rate ratio for infection comparing malnourished and wellnourished children (using IRIM and IRIW from the baseline situation where 20% of children are malnourished). RRC is the equivalent incidence rate ratio for cases of severe infection (using IRCM and IRCW from the baseline situation where 20% of children are malnourished). RRC is the incidence rate ratio that would generally be calculated from a conventional epidemiologic study. RRI ¼ IRIMðbaselineÞ : IRIWðbaselineÞ RRC ¼ IRCMðbaselineÞ : IRCWðbaselineÞ Two variations of the population attributable fraction (PAF) of cases of severe infection due to malnutrition were calculated. The first of these uses the conventional method of calculating the PAF using RRC and the prevalence of malnutrition (P) in the baseline situation (25): PAFC1 ¼ PðRRC 1Þ : PðRRC 1Þ þ 1 The second is an alternative PAF calculated directly from the model, using the total incidence of severe infection in the baseline situation, and the incidence of severe infection from the counterfactual situation where no children are malnourished: PAFC2 ¼ ½P × IRCMðbaselineÞ þ ð1 PÞ × IRCWðbaselineÞ IRCWðcounterfactualÞ : ½P × IRCMðbaselineÞ þ ð1 PÞ × IRCWðbaselineÞ Am J Epidemiol. 2016;183(6):574–582 Incorporating Transmission Into Causal Models 577 No. of Severe Cases A) 30 25 20 15 10 5 0 Date No. of Severe Cases B) 40 35 30 25 20 15 10 5 0 Date No. of Severe Cases C) 40 35 30 25 20 15 10 5 0 Date Figure 2. Fitted models for scenario A in 3 childhood infection settings at baseline. Circular markers show the observed number of cases each month. A) Hospital admissions for acute lower respiratory infection associated with respiratory syncytial virus in the Philippines (11); B) rotavirus infections in Guinea-Bissau (12); C) hospital admissions for rotavirus diarrhea in India (13). The solid lines show the monthly number of severe infections (in malnourished and well-nourished children) calculated from the fitted models. RESULTS Figure 2 shows the scenario A models fitted to the observed case numbers in each setting, assuming homogenous mixing. The fit for the scenario B and C models was similar. Tables 1 and 2 show the results from the models assuming Am J Epidemiol. 2016;183(6):574–582 homogenous mixing. For scenario A, there was no difference in the incidence of infection between malnourished and wellnourished children (RRI = 1.00); however, the increased risk of progressing to severe infection in malnourished children meant that the incidence of cases of severe infection was 578 Paynter Table 1. Incidence Rates (per 1,000 Child-Years) of 2 Childhood Infections Calculated From Models Assuming Homogenous Mixinga Scenario and Prevalence of Malnutrition, % IR Measureb IRIM IRIW IRCM Table 2. Risk Measures for 2 Childhood Infections From Models Assuming Homogenous Mixinga RRI IRCW 0 — c 650 650 0 PAFC2 1.00 1.30 0.06 0.06 32.5 B 1.30 1.30 0.06 42.3 0.48 32.5 C 1.00 1.00 0.00 — 0.39 Rotavirus in Guinea-Bissau Scenario B 20 PAFC1 A Scenario A 650 RRC RSV in the Philippines RSV in the Philippines 20 Risk Measureb Scenario 797 — 613 336 39.9 — 30.7 A 1.00 1.33 0.06 0.06 16.8 B 1.30 1.30 0.06 0.39 C 1.00 1.00 0.00 0.31 Scenario C 20 648 650 32.4 32.5 0 — 395 — 19.8 Rotavirus in Guinea-Bissau Scenario A 20 600 600 13.3 10.0 0 — 600 — 10.0 Scenario B 20 736 566 12.3 9.4 0 — 363 — 6.1 Scenario C 20 598 600 10.0 10.0 0 — 417 — 6.9 Rotavirus in India A 1.00 1.33 0.06 0.06 B 1.30 1.30 0.06 0.21 C 1.00 1.00 0.00 0.12 Abbreviations: PAF, population attributable fraction; RR, rate ratio; RSV, respiratory syncytial virus. a The RSV model was fitted to RSV hospital admissions data from the Philippines (11). The rotavirus model was fitted to rotavirus infection data from Guinea-Bissau (12) and rotavirus hospital admissions data from India (13). b RRI, incidence RR for infection; RRC, incidence RR for severe infection; PAFC1, conventional PAF; PAFC2, PAF calculated from the causal transmission models. Rotavirus in India Scenario A 20 1,000 1,000 22.2 16.7 0 — 1,000 — 16.7 Scenario B 20 1,226 943 20.4 15.7 0 — 789 — 13.1 16.6 16.7 — 14.7 Scenario C 20 995 0 — 1,001 881 Abbreviations: IR, incidence rate; RSV, respiratory syncytial virus. a The RSV model was fitted to RSV hospital admissions data from the Philippines (11). The rotavirus model was fitted to rotavirus infection data from Guinea-Bissau (12) and rotavirus hospital admissions data from India (13). b IRIM , IR of infection in malnourished children; IRIW, IR of infection in well-nourished children; IRCM , IR of severe infection in malnourished children; IRCW, IR of severe infection in well-nourished children. c IR could not be calculated. higher in malnourished children than in well-nourished children (RRC = 1.30 for RSV and RRC = 1.33 for rotavirus). Removing malnutrition from the population had no impact on the incidence of severe infection in well-nourished children; thus, PAFC1 and PAFC2 were the same (0.06). For scenario B, malnourished children had a higher incidence of infection than well-nourished children (RRI was set at 1.3), which led to a higher incidence of severe infection in malnourished children (RRC = 1.3). Upon removing malnutrition from the population, the incidence of severe infection in wellnourished children dropped considerably in all 3 settings. This is because the higher incidence of infection in the malnourished children was driving the incidence of infection in the well-nourished children, and removing malnutrition from the population removed this transmission effect. Thus, PAFC2 was considerably larger than PAFC1 in all 3 settings. For scenario C, there was no difference in the incidence of infection or severe infection between malnourished and wellnourished children (RRI and RRC = 1.00); however, despite this, the models found moderate-to-large values for PAFC2, while the conventional PAF calculation predicted no impact (PAFC1 = 0.00). In scenario C, PAFC2 was large despite there being no difference in the incidence of severe infection between malnourished and well-nourished children, because the higher infectiousness of the malnourished children was driving the incidence of infection equally in both the wellnourished and malnourished children. Removing malnutrition from the population removed this transmission effect. In both scenario B and scenario C, the discrepancy between PAFC1 and PAFC2 was greatest in the RSV model and smallest in the India rotavirus model. Figures 3 and 4 show the results for scenario B as the degree of mixing between malnourished and well-nourished children decreases (as δ moves from 1 to 0). Figure 3 shows that as the degree of mixing between the malnourished and well-nourished subgroups decreases, PAFC1 and PAFC2 converge; however, PAFC2 remains in excess of PAFC1 until there is no mixing between the malnourished and well-nourished Am J Epidemiol. 2016;183(6):574–582 Incorporating Transmission Into Causal Models 579 1.6 0.5 0.4 1.4 PAF Rate Ratio 0.3 0.2 1.2 0.1 0 1 1 0.8 0.6 0.4 0.2 0 Degree of Mixing, δ Figure 3. Estimates of the population attributable fraction (PAF) for scenario B in 3 childhood infection settings, according to the degree of mixing between malnourished and well-nourished children. The solid line shows the conventional PAF estimate (PAFC1), which is the same for all 3 settings. The broken lines show the PAF calculated directly from the causal transmission model (PAFC2) for each setting: respiratory syncytial virus in the Philippines (11) (dotted line), rotavirus in Guinea-Bissau (12) (dashed line), and rotavirus in India (13) (dotteddashed line). subgroups, at which point PAFC1 = PAFC2. Figure 4 compares the incidence rate ratio that would be found by a conventional epidemiologic study (RRC) with the true increase in susceptibility to infection among malnourished children (αM/αW). Figure 4 demonstrates that at higher levels of mixing, conventional studies will underestimate the true effect, while at lower levels of mixing, conventional studies will overestimate the true effect. The degree of underestimation of the true effect is largest in the India rotavirus model and smallest in the RSV model. Figures 5 and 6 show the results for scenario C as the degree of mixing between malnourished and well-nourished children decreases. Figure 5 shows that (as with scenario B) in scenario C, PAFC1 and PAFC2 converge as the degree of mixing decreases, until PAFC1 = PAFC2, when there is no mixing between malnourished and well-nourished children. Figure 6 demonstrates that for scenario C, RRC remains close to 1 until there are low levels of mixing between malnourished and well-nourished children, at which point RRC increases rapidly. DISCUSSION These causal transmission models have demonstrated that conventional epidemiologic methods are unable to detect the impact of the transmission effects of risk factors. Scenario A incorporated purely individual-level effects (malnourished children were neither more susceptible to infection nor more Am J Epidemiol. 2016;183(6):574–582 1 0.8 0.6 0.4 0.2 0 Degree of Mixing, δ Figure 4. Comparison of the conventional rate ratio (RRC) with the actual increase in susceptibility to infection among malnourished children (αM /αW) for scenario B in 3 childhood infection settings, according to the degree of mixing between malnourished and well-nourished children. The solid line shows the RRC, which is the same for all 3 settings. The broken lines show αM /αW for each setting: respiratory syncytial virus in the Philippines (11) (dotted line), rotavirus in Guinea-Bissau (12) (dashed line), and rotavirus in India (13) (dotted-dashed line). infectious). Thus, in this scenario the relative risk from a conventional epidemiologic study (RRC) could be used to accurately predict the PAF using the conventional formula. Scenario B incorporated both individual and transmission effects, and scenario C incorporated purely transmission effects. Thus, in both of these latter scenarios, the total amount of transmission in the population was increased when malnutrition was present in the population, and removing malnutrition from the population resulted in a larger benefit than would be predicted by the conventional PAF calculation. This difference remained substantial even with low degrees of mixing between the malnourished and well-nourished subgroups. While transmission effects occurred in scenarios B and C in all 3 settings, the impact of these effects differed between settings. Two factors appear to determine the impact of the transmission effects: the overall force of infection and the duration of immunity following infection. The mean force of infection was 0.0021 per day in the RSV model, 0.0022 per day in the Guinea-Bissau rotavirus model, and 0.0044 per day in the India rotavirus model. In the RSV model the mean duration of immunity following infection was 63 days, while in the rotavirus models this was 102 days. Settings with a higher force of infection have a higher incidence of infection, but they also have a higher prevalence of immune persons; thus, additional infectiousness has a progressively smaller impact on incidence, and conversely, there is reduced benefit in 580 Paynter PAF A) 3 0.4 0.2 0 1 0.8 0.6 0.4 0.2 0 PAF B) Rate Ratio Degree of Mixing, δ 0.4 0.2 2 0 1 0.8 0.6 0.4 0.2 0 Degree of Mixing, δ C) PAF 0.4 1 0.2 1 0.8 0.6 0.4 0.2 0 Degree of Mixing, δ 0 1 0.8 0.6 0.4 0.2 0 Degree of Mixing, δ Figure 5. Estimates of the population attributable fraction (PAF) for scenario C in 3 childhood infection settings, according to the degree of mixing between malnourished and well-nourished children. The solid lines denote the conventional PAF estimate (PAFC1) for each setting. The broken lines denote the PAF calculated directly from the causal transmission model (PAFC2) for each setting. A) Respiratory syncytial virus in the Philippines (11); B) rotavirus in Guinea-Bissau (12); C) rotavirus in India (13). reducing the amount of infectiousness from very high levels. This mechanism will be exacerbated if the duration of immunity is longer following infection. The RSV model has the lowest force of infection (however, in absolute terms this is still high—most children have been infected by RSV by their second birthday) and the shorter duration of immunity following infection, so the impact of transmission effects is largest in this model (Table 2, Figures 3 and 5). The causal transmission models have also demonstrated that conventional epidemiologic methods give biased effect estimates for risk factors that act at least partially through transmission effects. Figure 4 shows that in scenario B, conventional studies will tend to underestimate the true effect (i.e., RRC < αM /αW) when the degree of mixing is high (because the transmission effects are shared between the malnourished and well-nourished children, reducing the difference in incidence between these groups), and they will tend to overestimate the true effect (i.e., RRC > αM /αW) when the degree of mixing is low (because the transmission effects are confined to the malnourished children, increasing the difference in incidence between the malnourished and wellnourished groups). The difference between the India rotavirus model and the Guinea-Bissau rotavirus model in Figure 4 also indicates that if the force of infection is higher, conventional studies will tend to underestimate the true effect more. Figure 6. Variation in the conventional rate ratio (RRC) in scenario C in 3 childhood infection settings, according to the degree of mixing between malnourished and well-nourished children. The mean duration of infection is 1.3 times longer in malnourished children than in wellnourished children in all 3 settings. The broken lines show RRC for each setting: respiratory syncytial virus in the Philippines (11) (dotted line), rotavirus in Guinea-Bissau (12) (dashed line), and rotavirus in India (13) (dotted-dashed line). Conventional studies examining the RRC for malnutrition have found inconsistent results (6, 8, 24). One possible explanation for at least part of this inconsistency may be the variation in the force of infection and the degree of mixing between study settings. Mathematical modeling may provide a way of comparing these study results to gain a better estimate of the underlying true effect, αM /αW (although accurate parameter values for the force of infection and the degree of mixing would be required). Figure 6 shows that for moderate-to-high degrees of mixing, the RRC in scenario C was too small to be detected by anything other than the largest of conventional epidemiologic studies, despite the fact that the increased infectiousness in malnourished children had a large impact on the risk of infection in the entire population, as seen by the high values of PAFC2 in Figure 5. The concern here is that risk factors that act predominantly via increasing infectiousness may be missed by conventional studies comparing incidence between exposed and unexposed subjects. An example of this phenomenon could be the effect of vitamin C deficiency/ insufficiency on acute respiratory infections. In a recent Cochrane review (26), vitamin C supplementation did not appear to reduce the incidence of colds among persons taking supplements compared with persons not taking them (relative risk = 0.97, 95%confidenceinterval: 0.94,1.00).However, the review also found that vitamin C supplementation reduced the duration of colds in supplemented children by 14% Am J Epidemiol. 2016;183(6):574–582 Incorporating Transmission Into Causal Models 581 (95% confidence interval: 7, 21). The review’s authors, Hemila and Chalker, concluded that vitamin C supplementation fails to reduce the incidence of colds in the general population (26); however, if we consider the impact of transmission effects as illustrated in scenario C, it is likely that vitamin C insufficiency, even in only a subgroup of the population, will influence the total incidence of colds at the population level, by increasing the amount of transmission from persons with vitamin C insufficiency. The models showed that the impact of transmission effects is dependent on the level of mixing between exposed and unexposed children. It is reasonable to assume that there will be some degree of associative mixing within the different exposure groups, because children sharing a common environmental exposure are more likely to share socioeconomic circumstances. Previous studies have demonstrated that social contact patterns can be quantified and incorporated into transmission models (27, 28). The use of similar methods to quantify the level of mixing between exposed and unexposed groups would enable a more accurate interpretation of conventional epidemiologic measures. The findings from the RSV and rotavirus models may not necessarily be applicable to all infections. In particular, for infections with a large environmental reservoir (including zoonoses), the infectiousness of humans will have a relatively smaller impact on ongoing transmission. In addition, the source of infection in both the RSV and rotavirus models is cases with acute infection (be this symptomatic or asymptomatic). In contrast, many infections (including streptococcal infections, typhoid, and hepatitis B) are spread by chronic carriers. For these infections, risk factors that increase the acquisition or duration of carriage, or increase pathogen shedding from persons with carriage, will have an important impact on transmission. The models presented here have a number of potential limitations. First, the models only incorporate a single risk factor. In reality, a number of risk factors will be present in the population, and each risk factor that increases transmission will be responsible for a proportion of the force of infection acting on the population at baseline (or alternatively, each risk factor that increases transmission is responsible for a proportion of the basic reproductive number (R0) in that population). The interplay between these risk factors at the population level will depend on the interaction of multiple risk factors in the same individual. Second, malnutrition is modeled as a binary variable. In reality, the effect of malnutrition progressively increases as malnutrition worsens (29). Methods have been developed to include both multiple risk factors and continuous exposure variables in conventional PAF calculations (30), and similar solutions can be incorporated into causal transmission models. A third potential limitation is the simplified model structure. For example, resistance to infection with both RSV and rotavirus increases with age during early childhood, a phenomenon that has not been incorporated into the model structure (an acceptable simplification, as the models are not being fitted to age-specific data). In addition, modeling the 3 separate scenarios is somewhat artificial, and in reality all 3 scenarios may occur to some degree. A fourth limitation is that other mechanisms, not modeled here, may also contribute to increased transmission in children with malnutrition. Children with more severe respiratory Am J Epidemiol. 2016;183(6):574–582 infection may excrete more virus, although this has not been examined specifically for malnutrition. Conversely, children with more severe disease may have fewer contacts than those with milder illness. It is also plausible that malnourished children have shorter incubation periods, which would also affect transmission. A final limitation is the requirement to determine parameters from the literature. While some parameters, such as the duration of infectiousness, are relatively straightforward to estimate from existing studies, others, such the rate of loss of immunity following infection (γ), are more difficult to estimate (the method used to estimate the value of γ for each infection is described in Web Appendix 1). Inaccuracy in this latter parameter is particularly problematic, because the model results suggest that the impact of transmission effects is dependent on the duration of immunity following infection, as well as the force of infection. Because of these limitations, the estimates presented here are best considered approximations of the impact of transmission effects, showing the direction and approximate magnitude of the biases inherent in using conventional epidemiologic methods to investigate the causality of infectious disease. More accurate estimates will require models incorporating new data from studies directly examining transmission effects and population mixing levels. For the present, however, several practical points of advice can be taken from the model findings (see text Appendix). To fully understand infectious disease causality, we need to understand the dynamics of causality at the population level. Infectious diseases remain the biggest killer of children globally, and new infectious threats are emerging or reemerging regularly. Increased efforts are warranted to refine epidemiologic methods to more accurately assess the causality of infectious diseases and to more accurately measure the disease burden attributable to infectious disease risk factors. ACKNOWLEDGMENTS Author affiliations: School of Public Health, University of Queensland, Brisbane, Queensland, Australia (Stuart Paynter); and School of Public Health, Curtin University, Perth, Western Australia, Australia (Stuart Paynter). Conflict of interest: none declared. REFERENCES 1. Samarasekera U, Horton R. Continuing the child survival revival. Lancet. 2013;381(9875):1335–1336. 2. Halloran ME, Struchiner CJ. Causal inference in infectious diseases. Epidemiology. 1995;6(2):142–151. 3. Koopman JS, Longini IM Jr. The ecological effects of individual exposures and nonlinear disease dynamics in populations. Am J Public Health. 1994;84(5):836–842. 4. Lin H-H, Murray M, Cohen T, et al. Effects of smoking and solid-fuel use on COPD, lung cancer, and tuberculosis in China: a time-based, multiple risk factor, modelling study. Lancet. 2008;372(9648):1473–1483. 582 Paynter 5. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859): 2095–2128. 6. Victora CG, Barros FC, Kirkwood BR, et al. Pneumonia, diarrhea, and growth in the first 4 y of life: a longitudinal study of 5914 urban Brazilian children. Am J Clin Nutr. 1990;52(2): 391–396. 7. Tupasi TE, Mangubat NV, Sunico MES, et al. Malnutrition and acute respiratory tract infections in Filipino children. Rev Infect Dis. 1990;12(suppl 8):S1047–S1054. 8. Guerrant RL, Schorling JB, McAuliffe JF, et al. Diarrhea as a cause and an effect of malnutrition: diarrhea prevents catch-up growth and malnutrition increases diarrhea frequency and duration. Am J Trop Med Hyg. 1992;47(1):28–35. 9. James JW. Longitudinal study of the morbidity of diarrheal and respiratory infections in malnourished children. Am J Clin Nutr. 1972;25(7):690–694. 10. Olofin I, McDonald CM, Ezzati M, et al. Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: a pooled analysis of ten prospective studies. PLoS One. 2013;8(5):e64636. 11. Paynter S, Yakob L, Simões EA, et al. Using mathematical transmission modelling to investigate drivers of respiratory syncytial virus seasonality in children in the Philippines. PLoS One. 2014;9(2):e90094. 12. Fischer TK, Valentiner-Branth P, Steinsland H, et al. Protective immunity after natural rotavirus infection: a community cohort study of newborn children in Guinea-Bissau, West Africa. J Infect Dis. 2002;186(5):593–597. 13. Purohit SG, Kelkar SD, Simha V. Time series analysis of patients with rotavirus diarrhoea in Pune, India. J Diarrhoeal Dis Res. 1998;16(2):74–83. 14. Nokes DJ, Okiro EA, Ngama M, et al. Respiratory syncytial virus infection and disease in infants and young children observed from birth in Kilifi District, Kenya. Clin Infect Dis. 2008;46(1):50–57. 15. Henderson FW, Collier AM, Clyde WA Jr, et al. Respiratory-syncytial-virus infections, reinfections and immunity. A prospective, longitudinal study in young children. N Engl J Med. 1979;300(10):530–534. 16. Parashar UD, Hummelman EG, Bresee JS, et al. Global illness and deaths caused by rotavirus disease in children. Emerg Infect Dis. 2003;9(5):565–572. 17. Gladstone BP, Ramani S, Mukhopadhya I, et al. Protective effect of natural rotavirus infection in an Indian birth cohort. N Engl J Med. 2011;365(4):337–346. 18. Okiro EA, Ngama M, Bett A, et al. Factors associated with increased risk of progression to respiratory syncytial virus-associated pneumonia in young Kenyan children. Trop Med Int Health. 2008;13(7):914–926. 19. Paynter S, Ware RS, Lucero MG, et al. Malnutrition: a risk factor for severe respiratory syncytial virus infection and hospitalization. Pediatr Infect Dis J. 2014;33(3):267–271. 20. Tomkins A. Nutritional status and severity of diarrhoea among pre-school children in rural Nigeria. Lancet. 1981;317(8225): 860–862. 21. Sepúlveda J, Willett W, Muñoz A. Malnutrition and diarrhea: a longitudinal study among urban Mexican children. Am J Epidemiol. 1988;127(2):365–376. 22. Heymann DL. Control of Communicable Diseases Manual. Washington, DC: American Public Health Association; 2008. 23. Okiro EA, White LJ, Ngama M, et al. Duration of shedding of respiratory syncytial virus in a community study of Kenyan children. BMC Infect Dis. 2010;10:15. 24. Black RE, Brown KH, Becker S. Malnutrition is a determining factor in diarrheal duration, but not incidence, among young children in a longitudinal study in rural Bangladesh. Am J Clin Nutr. 1984;39(1):87–94. 25. Murray CJ, Ezzati M, Lopez AD, et al. Comparative quantification of health risks: conceptual framework and methodological issues. Popul Health Metr. 2003;1(1):1. 26. Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev. 2013;(1):CD000980. 27. Wallinga J, Teunis P, Kretzschmar M. Using data on social contacts to estimate age-specific transmission parameters for respiratory-spread infectious agents. Am J Epidemiol. 2006; 164(10):936–944. 28. Mossong J, Hens N, Jit M, et al. Social contacts and mixing patterns relevant to the spread of infectious diseases. PLoS Med. 2008;5(3):e74. 29. Caulfield LE, de Onis M, Blössner M, et al. Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumonia, malaria, and measles. Am J Clin Nutr. 2004;80(1): 193–198. 30. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. APPENDIX Practical Advice From the Model Findings 1. Accurate estimation of the effect and impact of a risk factor on infectious disease incidence requires an understanding of the underlying mechanism of action of the risk factor and the resulting transmission dynamics. 2. Risk factors that act at least partially through transmission effects will be responsible for a larger proportion of the total disease burden than would be estimated using conventional epidemiologic methods. 3. The effect of risk factors that act predominantly via increasing the infectiousness of exposed persons may be missed by conventional studies comparing incidence between exposed and unexposed subjects. 4. Conventional measures of effect for the same risk factor can vary from setting to setting, depending on the underlying risk of infection and the degree of mixing between exposed and unexposed individuals. Am J Epidemiol. 2016;183(6):574–582