Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Idiopathic intracranial hypertension wikipedia , lookup
Contact lens wikipedia , lookup
Keratoconus wikipedia , lookup
Vision therapy wikipedia , lookup
Visual impairment wikipedia , lookup
Eyeglass prescription wikipedia , lookup
Cataract surgery wikipedia , lookup
Blast-related ocular trauma wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
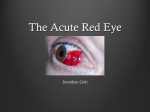
Grace Wong GPST1 Assessment of the red eye Common causes of red eye Painful and Non Painful Signs and symptoms Management of each condition Common presentation in primary care and in A+E Most cases due to relatively trivial problems Most common is conjunctivitis Small proportion are serious and need urgeny treatment Sometimes difficulty in discerning between causes Most practical way is; Pain or not Visual acuity Onset Pain Visual Changes Photophobia Foreign body sensation Trauma Discharge, clear or colored Bilateral or unilateral Social history Nursery school teacher Co-morbid condition Collagen vascular disorders Rheumatoid, gout TB, sarcoidosis HTN Past Ocular History E.g. Similar episodes Surgery Lazy eye Contact lenses Visual acuity Extra ocular movements Pen light examination (reactivity, corneal opacity, pupil shape, discharge, infection) Test for direct and consensual photophobia Slit lamp examination – with and without fluorescein Anterior chamber evaluation – depth, cells IOP meaurements Think systemically about the structures within the eye to common to differential diagnosis Inflammation of orbit? Lid Disease Scleral inflammation Corneal disease Uveal/iris inflammation Other e.g. glaucoma Most common cause of red eye Inflammation of the conjunctiva Sore red eye (gritty or itchy discomfort) Discharge (clear, mucoid or muco-purulent) Sticky eyelids No visual changes Unilateral or bilateral Examination - enlarged papillae under upper eye lid or pre auricular lymph nodes Allergic, viral or bacterial Difficult to distinguish between types Both bacterial and viral can occur after a viral URTI Bacterial Viral Allergy Enlarge pre auricular nodes Enlarged tender preauricular nodes Pruritus Atopic Mucopurulent discharge Watery discharge Watery or mild mucus discharge Staph, Strep, Haem Adenovirus Allergen Unilateral or bilateral Bilateral Bilateral Sore Sore Sore and Itchy eyes Conjunctival infection Chemosis Conjunctival infection Chemosis Follicles in the lower tarsal conjunctiva Conjunctival infection Follicles in the lower tarsal conjunctiva Cobblestone under the upper lid 85% of cases clear in <7 days with or without tx Advise patients to bathe the affected eye with boiled cooled water am and pm If symptoms not improve in >5 days Swab for MC+S Treat empirically with chloramphenicol QDS consider alternative diagnosis e.g. allergy, dry eyes, Consider referral >7-10 days or if suspicion of herpetic infection Topic or systemic anti histamines e.g. sodium cromoglicate eye drops Avoid topical steroids – long term complications e.g. cataract, glaucoma, fungal infection Consider cold compress and wash out with cold water during acute exacerbation Refer if symptoms are persistent despite treatment or if vision is affected Spontaneous painless localised haemorrhage under the conjunctiva Common in the elderly Spontaneous or traumatic Looks alarming but generally painless (may cause some aching) Clear spontaneously in 1-2 weeks but may recur Hypertension Clotting disorders Leukaemia Increased venous pressure Check BP If severe/recurrent Check FBC and clotting screen Blood under conjunctiva covering part or all of eye Normal Visual Acuity Consider referral if; Follows trauma More than a slight discomfort Fails to settle spontaneously over 1 week Chronic low grade inflammation of meibomian glands and lid margins Both eyes usually affected Often associated with Dry eye syndrome, seborrhoeic dermatitis, rosacea Staphylococcal Seborrhoeic – associated with seborrhoeic dermatitis. Yeast is involved and can trigger inflammatory reaction Meibomain – gland dysfunction unable to lubricate eye Presents with long history of irritable burning dry red eyes Eyelids have red margins Look inflamed and greasy Tiny flakes or scales on eyelids Sticky with discharge Meibomian glands may block an fill with oily fluid Symptoms come and go Regular eyelid hygiene – warm, massage and cleansing Remove scales and crusts from lid margins Treat dry eye symptoms with preservative free tear supplements e.g. liquifilm Antibiotic eye treatment if eyelid becomes infection e.g. fusidic acid (topical on eyelid). Can be up to 3 month course Inflammation of the cornea Bacterial, viral or fungal infections Can be non infective e.g. trauma or auto-immune, dry eyes, entropion History of contact lens wear Previous episodes e.g. HSV infection Very painful red eye Photophobia Foreign body sensation Reduced visual acuity depends on nature of problem Circumcorneal injection Conjunctiva is also inflamed – keratoconjuncivitis Discharge – water, mucoid or purulent Pupil may be small Fluorescin readily demonstrates any ulceration Significant loss of vision secondary to scarring or astigmastism Complications can lead to blindness; Corneal perforation Choroidal detachment Endopthalmitis CORNEAL ULCERATION IS AN OPTHALMOLOGIC EMERGENCY The cause must be identified prior to treatment - some therapies benefit whilst others can harm Refer the same day for urgent ophthalmological review Delay may result in loss of sight If caused by Herpes simplex infection and dendritic ulcer AVOID topical steroids as can cause massive amoebic ulceration and blindness Typical dendritic ulcer – delicate branching pattern Severe inflammation that occurs throughout the entire thickness of the sclera Rare Average age 52 yrs Can be unilateral or bilateral Affects more women than men Can affect anterior or posterior segment Either nodular, diffuse or necrotizing The sclera is an avascular structure 50% is associated with systemic illness; Herpes Zoster Rheumatoid arthritis SLE Polyarteritis nodosum Wegner’s granulomatosis Trauma Infection Surgery Red eye Severe boring eye pain – may radiate to forehead, brow or jaw Key symptom; gradual onset (days or weeks) Pain worse with movement of eye and at night Watering Photophobia Decreased visual acuity Eye is tender to touch and may have deep purple hue There may be accompanying uveitis and keratitis Urgent referral to ophthalmology Treated with steroids Complications include Cataract Glaucoma Retinal detachment Most common in young/middle aged adults Acute onset of pain Increasing pain as eye converges and pupil constrict Photophobia Blurred vision Decreased visual acuity Watering Circumcorneal rednress Small or irregular pupil + hypopyon (pus causing white fluid level line) Secondary to corneal graft rejection Eye infections e.g. toxoplasmosis, herpes virus keratitis 30% are associated with seronegative arthropathies e.g. AS Refer urgently to ophthalmology Complications include; Posterior synechiae (irregular pupil shape) Glaucoma Cataract Relapses are common Decreased visual acuity Pain deep in the eye – not surface irritation Photophobia Absent or sluggish pupil response Corneal Damage on fluorsecein staining or opacification History of trauma These need same day referral http://www.patient.co.uk/doctor/The-Red-Eye.htm