Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Cardiovascular disease wikipedia , lookup
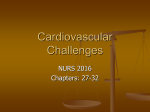
Cardiac surgery wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
History of invasive and interventional cardiology wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Antihypertensive drug wikipedia , lookup
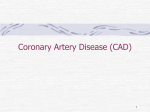
Coronary Artery Disease Dr. Belal Hijji, RN, PhD September 28, 2011 Learning Outcomes At the end of this lecture, students will be able to: • Provide brief description of CAD and its etiology. • Discuss the risk factors for the development of CAD and describe its pathophysiology. • Define unstable angina, recognise its medical and nursing management.. • Define MI and describe its pathophysiology in brief. • Discuss the medical and nursing management of patient with acute MI. 2 Description and Etiology • CAD is the biggest contributor to cardiovascular-related morbidity and mortality. Atherosclerosis is a progressive disease that affect arteries throughout the body. • There is a strong association between specific risk factors and the development of CAD. These are discussed next. 3 Risk Factors for CAD • These factors are: – Nonmodifiable such as age (middle & old), race (people of color & multiracial population than white people), family history (close blood relatives who had MI or stroke before the age of sixty). – Modifiable such as elevated serum lipids (cholesterol, triglycerides, HDL, LDL, VLDL). Refer to the last slide for these abbreviations. Other factors are high-fat diet, obesity, physical inactivity, hypertension (SBP > 140 mm Hg or DBP > 90 mm Hg), cigarette smoking, and chronic kidney disease. 4 Pathophysiology of CAD • CAD is a progressive atherosclerotic disorder of the coronary arteries that results in narrowing or complete obstruction (See picture on next slide). • Atherosclerosis affects the medium-size arteries that perfuse the heart and other organs. 5 6 Acute Coronary Syndromes (ACS) • ACS is used to describe the array of clinical presentations of CAD that range from unstable angina to acute MI (myocardial infarction). Both cases will be dealt with next. 7 Unstable Angina • Unstable angina is defined as a change in a previously established stable pattern of angina (which is predictable, exercise induced, and results from fixed blockages of > 75% of the coronary artery lumen). • Unstable angina is more intense than stable angina, may interrupt sleep, or may require than nitrates for pain relief. • Severe angina that lasts for more than 5 minutes, is worsening in intensity, and is not relieved by nitroglycerin tablet is a medical emergency. Activate Emergency Medical Services to take the patient to hospital. • Unstable angina may indicate atherosclerotic plaque rupture and thrombus formation that can lead to MI. Patient reporting to emergency dept. with recent onset of unstable angina who has nonspecific or nonelevated ST segment should be admitted to the CCU. 8 Medical Management • If there is ST segment elevation on 12-lead ECG, the patient should be treated for acute MI. Normal ECG 9 An ECG showing ST-segment elevation (orange) in I, aVL and V1-V5 with reciprocal changes (blue) in the inferior leads, indicative of an anterior wall myocardial infarction 10 Medical Management (Continued..) • If there is no ST segment elevation but chest pain continues, the patient should receive aspirin, nitroglycerin for vasodilation, intravenous antiplatelet agents such as glycoprotein inhibitors, and unfractionated heparin. 11 Nursing Management • Nursing interventions of a patient with angina focus on: • Early identification of myocardial ischemia. • Assess immediately any complaints of chest pain using a pain scale of 0 – 10, as pain (or pressure or heaviness) is an indicator of myocardial ischemia. Immediate assessment is important for early identification and treatment. • Document vital signs, ECG, skin color, peripheral pulses, level of consciousness, and overall tissue perfusion. • Control of chest pain. • Administer oxygen, nitrates, and analgesia as ordered. • Use pulse oximetry to guide therapy and maintain oxygen saturation above 90%. 12 • Nursing interventions of a patient with angina focus on (Continued…): • Patient and family education • Educate your patient when his/ her condition has stabilised (pain controlled). • Teach the patient about the importance of avoiding the Valsalva maneuver (bearing down when going to bath room). This maneuver increases intrathoracic pressure that decreases venous return to the right side of the heart which is associated with hypotension and bradycardia. • Teach the patient about risk factor modifications such as decreasing fat intake, stopping smoking, reducing salt intake, controlling hypertension, increasing physical activity as tolerated, and achieving normal body weight. • Provide information about medications; indications and side effects. • Teach the patient about the importance of follow up after discharge and how to handle emotional stress and anger. 13 Myocardial Infarction • Definition: MI is a description of an irreversible myocardial necrosis (cell death) that results from abrupt decrease or complete cessation of coronary blood flow to the myocardium. • Pathophysiology (See next slide): – Ischemia: The outer region of infarcted myocardial area known as zone of ischemia. It is composed of viable cells. – Injury: The infarcted zone is surrounded by injured but still potentially viable tissue known as zone of injury. – Infarction: The area of dead muscle in the myocardium. 14 15 A myocardial infarction (2) of the tip of the anterior wall of the heart (an apical infarct) after occlusion (1) of a branch of the left coronary artery (LCA), right coronary artery = RCA. 16 Medical Management of MI • Using the research-based guidelines developed by the American College of Cardiology and the American Heart Association decreases in-hospital mortality rate post MI from 15.3% to 8.3%. Emergency treatment of acute STEMI includes: – Fibrinolytic therapy (Streptokinase, or alteplase, or reteplase) are used to stimulate lysis of the clot or through mechanical opening the occluded artery. – Anticoagulants: Heparin co-administration with fibrinolytic therapy. The initial dose of heparin is 60 International Units (IU)/ kg (Maximum 4000 IU) IV, followed by continuous heparin drip at 12 IU/kg/hr (Max 1000 IU/hr). – Beta-blockers (metoprolol or atenolol) to prevent dysrhythmias. 17 Medical Management of MI (Continued…) – Anti-diabetic agents for tight glucose control to improve survival rate. – Angiotensin-Converting Enzyme (ACE) Inhibitors: These include lisinopril and captopril and are helpful in prevention of heart failure. 18 Nursing Management of MI • Nursing interventions for a patient with acute MI focus on: – Achieving a balance between myocardial oxygen supply and demand: This means that in the acute phase, there is a need to increase myocardial oxygen supply by oxygen administration to prevent tissue hypoxia. Myocardial oxygen supply can be enhanced by the administration of coronary artery vasodilators (nitroglycerin). – Prevention of complications: Nurses need to apply cardiac monitoring of patient to detect early ventricular dysrhythmias. In addition, nurses should continue to assess for signs of ischemic pain. 19 Nursing Management of MI (Continued…) – Health education: Nurses should focus on: • Pathophysiology of acute MI. • Description of signs and symptoms such as pain. pressure, or heaviness in chest. • Notification of nurses of any changes in chest pain intensity. • Avoidance of the Valsalva maneuver. • Risk factors modification, including: – – – – – – – Daily fat intake < 30% of total calories. Maintain serum cholesterol level < 200 mg/dL. Maintain LDL cholesterol to < 70 mg/dL. Stop smoking and reduce daily salt intake. Control hypertension and diabetes mellitus. Increase physical activity and reduce weight 20 Nursing Management of MI (Continued…) – Health education (Continued…): Nurses should focus on: • Medication teaching: indications and side effects. • Follow-up care after discharge. 21 Abbreviations • HDL cholesterol: High-density lipoprotein cholesterol. It is described as good cholesterol because it has protective effect against acute atherosclerosis. • LDL cholesterol: Low-density lipoprotein cholesterol. It is described as the bad cholesterol because high levels are associated with an increased risk of CAD, stroke, and peripheral arterial disease. • VLDL cholesterol: Very-low-density lipoprotein cholesterol. When the triglyceride levels are high, the VLDL level is also high. 22