Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Prescription costs wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Clinical trial wikipedia , lookup
Discovery and development of cyclooxygenase 2 inhibitors wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug discovery wikipedia , lookup
Drug interaction wikipedia , lookup
Plateau principle wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Dydrogesterone wikipedia , lookup
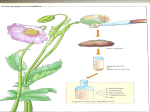
What data can a 14C clinical study deliver? A decade of innovative, integrated 14C study designs to understand drug behaviour in human subjects Iain Shaw Director, 14C Enabled Drug Development Quotient Clinical, Nottingham, UK IIS Conference, Princeton NJ, June 7-11th 2015 Scope • Brief introduction to Quotient Clinical • What’s it all about • Conventional human ADME • Integrated human ADME • Final deliverables 2 About Quotient Clinical 3 • Full service, early development provider founded in 1990 • Unique Translational Pharmaceutics platform • Expert formulation development • Real-time GMP manufacturing • 85 bed clinical pharmacology unit • Highly integrated operations in the UK • Approx. 250 employees – “full service” capability • International client base (approx. 55% US, 40% EU, 5% RoW) • Clients range from top pharma to emerging biotechs 3 What are we trying to achieve? Regulatory objectives Regulatory-driven clinical metabolism studies NDA/MAA/PMDA Submission requirements Mass balance Rates and routes of elimination Metabolite profiling & identification TGA Submission requirements As above + Absolute bioavailability Study requirements are many/varied and programs are often complex 5 What is required? • “Nonclinical characterization of a human metabolite(s) is only warranted when that metabolite(s) is observed at exposures greater than 10% of total drug-related exposure and at significantly greater levels in humans than the maximum exposure seen in the toxicity studies 6 The “regulatory package” plasma metabolites Pooled plasma Human Rat Dog 7 2h plasma pool across subjects Human 8h plasma pool across subjects Rat Dog “AUC”pool, Subject 1 Oral disposition dashboard Input Oral Fraction absorbed Drug in Portal Blood Drug in Intestine Betaglucuronidase Metabolism in Liver Phase 1 Phase 2 Bile First Pass Loss % Metabolites in Intestines Fraction unabsorbed Drug and metabolites in Blood % Exposure, F % Parent % MET1, MET2, etc. Mass balance recovery Total Recovery % dose 8 = Excretion in Feces % dose + Excretion In expired air % dose + Excretion In Urine % dose % Total Recovery % Parent % MET1, MET 2, etc. Conventional human ADME study An open-label, single period study in a cohort of 6-8 healthy male subjects SINGLE PERIOD Oral 14C drug product Overall residence period is dependent on radiochemical half-life, dictating residency period to achieve mass balance 9 Define oral mass balance and determine human metabolite profile and characterise key metabolites Standalone clinical study and metabolite investigation reports 9 Conventional ADME study • N=6 healthy volunteers • Single oral suspension dose of 300mg 14C-netupitant containing nmt 60µCi radioactivity • Residency period 14 days plus 2 return visits of 24 hours for further collections • Outcomes: • Mass balance established • Routes and rates of excretion determined • Key metabolites identified 10 Pharmacokinetics and Pharmacodynamics Netupitant PET Imaging and ADME Studies in Humans The Journal of Clinical Pharmacology XX(XX) 1–12 © 2013 The Authors. The Journal of Clinical Pharmacology Published by Wiley Periodicals, Inc. on behalf of The American College of Clinical Pharmacology DOI: 10.1002/jcph.198 Tulla Spinelli1, Selma Calcagnile1, Claudio Giuliano1, Giorgia Rossi1, Corinna Lanzarotti1, Stuart Mair2, Lloyd Stevens2, and Ian Nisbet2 Abstract Netupitant is a new, selective NK1 receptor antagonist under development for the prevention of chemotherapy‐induced nausea and vomiting. Two studies were conducted to evaluate the brain receptor occupancy (RO) and disposition (ADME) of netupitant in humans. Positron emission tomography (PET) imaging with the NK1 receptor‐binding–selective tracer [11C]‐GR205171 was used to evaluate the brain penetration of different doses of netupitant (100, 300, and 450 mg) and to determine the NK1‐RO duration. A NK1‐RO of 90% or higher was achieved with all doses in the majority of the tested brain regions at Cmax, with a long duration of RO. The netupitant minimal plasma concentration predicted to achieve a NK1‐RO of 90%, C90%, in the striatum was 225 ng/mL; after administration of netupitant 300 mg, concentrations exceeded the C90%. In the ADME study, a single nominal dose of [14C]‐netupitant 300 mg was used to assess its disposition. Absorption was rapid and netupitant was extensively metabolized via Phase I and II hepatic metabolism. Elimination of >90% was predicted at day 29 and was principally via hepatic/biliary route (>85%) with a minor contribution of the renal route (<5%). In conclusion, these studies demonstrate that netupitant is a potent agent targeting NK1 receptors with long lasting RO. In addition, netupitant is extensively metabolized and is mainly eliminated through the hepatic/biliary route and to a lesser extent via the kidneys. Keywords NEPA, netupitant, palonosetron, metabolism, receptor occupancy Nausea and vomiting represents one of the most feared side effects of chemotherapy.1,2 Chemotherapy‐induced nausea and vomiting, CINV, is described as acute, when it Integrated study designs • Single and multi-part study designs can now provide a full and complete metabolism and pharmacokinetic data package for regulatory submission • Combinations of extravascular (oral, inhaled etc.) and iv administration with therapeutic and/or tracer dosing can deliver an understanding of • • • • • • • 11 Fraction absorbed Absolute bioavailability Intravenous pharmacokinetics Mass balance Routes and rates of elimination Metabolic fate All of the above are molecule specific and data driven 11 Integrated 14C ivMicrotracer/ ADME study An open-label, 2-way crossover study in a single cohort of 6-8 healthy male subjects PART 1 PART 2 Oral drug product with an intravenous microtracer dose of 14C drug product Oral 14C drug product Overall duration is dependent on halflife, dictating wash-out period between Parts 1 and 2 and residency period to achieve mass balance 12 Defines intravenous pharmacokinetics, mass balance and absolute bioavailability Defines oral mass balance, human metabolite profile and chemical structure of key metabolites Standalone clinical study and metabolite investigation reports 1 2 12 Combination of 14C IVMT and 14C oral dosing • N=6 healthy volunteers • 2 period study • • Period 1 IVMT collecting plasma urine faeces and bile to 72/26hr post dose Period 2 ADME collecting blood plasma urine and faeces to 178hr post dose • Sample analysis: • • • AMS (total radioactivity & C-14 parent compound) LSC (Total radioactivity) LC/MS/MS (parent compound) • Outcomes: • • • • 13 • IV and oral mass balance Routes and rates of excretion Absolute bioavailability Fraction absorbed Assessment of biliary excretion Combination of 13C IVMT and 14C oral dosing • • 14 13C-Tofogliflozin IV microtracer 0.1mg dose 14C-Tofogliflozin Oral 20mg therapeutic dose 14 Radiolabelled intravenous and oral ADME study An open-label, 2 period study in 2 cohorts of 6-8 healthy male subjects COHORT 1 COHORT 2 14C Intravenous drug product Oral 14C drug product Define IV mass balance, IVPK, determine human IV metabolite profile and characterise key metabolites Define oral mass balance, Fa, determine human oral metabolite profile and characterise key metabolites Current unpublished example IV and oral toxicology plus IV and oral dosimetry required to support study design 15 Standalone clinical study and metabolite investigation reports 15 Integrated human ADME options Study options Data Analysis Requirements Data required for NDA submission 16 ADME IV:PO cross/ ADME IV ADME/Oral ADME 13C ivMT/ ADME 14C ivMT/ ADME Mass balance – oral dose Y Oral routes/rates of elimination Y Met profiling Y Met ID Y (Y) X X IV PK and clearance N X Mass balance – IV dose N X X X Fraction absorbed N X X X IV routes/rates of elimination N X X X Absolute bioavailability Study Delivery Complexity Study design is driven by drug & client data requirements 16 The final deliverable Completed dashboard % Exposure 0.5% Parent 2.2% Metab 1 57% Total Recovery 18 30% Total Recovery Opportunity from an ADME dashboard • N=6 healthy volunteers http://informahealthcare.com/xen ISSN: 0049-8254 (print), 1366-5928 (electronic) Xenobiotica, Early Online: 1–9 • Mass balance established • Routes and rates of excretion determined • Key metabolites identified • Review results alongside corresponding in vitro investigations • Understanding of dominant CYP enzyme involved in the metabolism and DDI liability 19 ! 2013 Informa UK Ltd. DOI: 10.3109/00498254.2013.865856 RESEARCH A RTICL E Absorption, metabolism and excretion of [14C]gemigliptin, a novel dipeptidyl peptidase 4 inhibitor, in humans Namtae Kim1, Lorna Patrick2, Stuart Mair2, Lloyd Stevens2, Gill Ford3, Vicky Birks3, and Sung-Hack Lee1 1 LG Life Sciences, Drug Metabolism and Pharmacokinetics, Daejeon, Republic of Korea, 2Quotient Clinical, Nottingham, UK, and 3Quotient Bioresearch, Rushden, UK Abstract Keywords 1. Gemigliptin (formerly known as LC15-0444) is a newly developed dipeptidyl peptidase 4 inhibitor for the treatment of type 2 diabetes. Following oral administration of 50 mg (5.4 MBq) [14C]gemigliptin to healthy male subjects, absorption, metabolism and excretion were investigated. 2. A total of 90.5% of administered dose was recovered over 192 hr postdose, with 63.4% from urine and 27.1% from feces. Based on urinary recovery of radioactivity, a minimum 63.4% absorption from gastrointestinal tract could be confirmed. 3. Twenty-three metabolites were identified in plasma, urine and feces. In plasma, gemigliptin was the most abundant component accounting for 67.2% rv 100% of plasma radioactivity. LC15-0636, a hydroxylated metabolite of gemigliptin, was the only human metabolite with systemic exposure more than 10% of total drug-related exposure. Unchanged gemigliptin accounted for 44.8% rv 67.2% of urinary radioactivity and 27.7% rv 51.8% of fecal radioactivity. The elimination of gemigliptin was balanced between metabolism and excretion through urine and feces. CYP3A4 was identified as the dominant CYP isozyme converting gemigliptin to LC15-0636 in recombinant CYP/FMO enzymes. DPP-4 inhibitor, human mass balance, pharmacokinetics History Received 25 September 2013 Revised 8 November 2013 Accepted 11 November 2013 Published online 4 December 2013 Summary • Requirements for NDA and MAA submission are addressed by the conventional human ADME study • Integrated studies can enhance the data generated depending on the needs of the drug candidate • Linking the human ADME and in vitro metabolism outcomes is key to help understanding of DDI liability 20 To transform drug development with science and innovation Speed Quality Passion [email protected] 21