Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
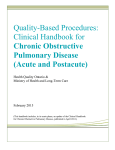
Management of stable chronic obstructive pulmonary disease(06) 1 Dr Mazen Qusaibaty MD, DIS / Head Pulmonary and Internist Department Ibnalnafisse Hospital Ministry of Syrian health Email: [email protected] General Approach 3 Diagnosis Of COPD Risk Factors Symptoms Spirometry COPD Assessment Obstruction Severity of Obstruction Post-Bronchodilator FEV1/FVC < 0.70 Gold IV FEV1 <30% Gold III FEV1 30%-50% Gold II FEV1 50%-80% Gold I FEV1 ≥80% mMRC CAT Frequent Exacerbation C D Severe Obstruction Less symptoms ++ exacerbations Very Severe Obstruction More symptoms ++ exacerbations ≥ 2 or more per year A B 1 per year Mild Obstruction Less symptoms Few exacerbations Moderate Obstruction More symptoms Few exacerbations None 0 1 < 10 2 Symptoms 3 > 10 4 Exacerbation Worse More Severe • High risk • Less symptoms • Low risk • Less symptoms • High risk • More symptoms C D A B • Low risk • More symptoms Global Initiative for Chronic Obstructive Lung Disease © Global Initiative for Chronic Obstructive Lung Disease The main TWO goals of the current management of COPD These goals should be reached with minimal side effects from treatment The main TWO goals of the current management of COPD Reduce the impact of COPD on daily activities Reduce risks of future events From the Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. Available from: http//www.goldcopd.org, © 2014 Global Initiative for Chronic Obstructive Lung Disease, all rights reserved. Relieve symptoms Reduce symptoms Improve exercise tolerance Improve health status Management of COPD Prevent disease progression Reduce risks Prevent and treat exacerbations Reduce From the Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014. Available from: http//www.goldcopd.org, © 2014 Global Initiative for Chronic Obstructive Lung Disease, all rights reserved. mortality ALL Categories of COPD C D A B Adapted from: Global Initiative for Chronic Obstructive Pulmonary Disease, Executive Summary: Global Strategy for the Diagnosis, Management, and Prevention of COPD (Accessed November 8, 2013) Avoidance of risk factor(s), such as smoking Adapted from: Global Initiative for Chronic Obstructive Pulmonary Disease, Executive Summary: Global Strategy for the Diagnosis, Management, and Prevention of COPD (Accessed November 8, 2013) Reduction of indoor pollution 12 Reduction Of Occupational Exposure 13 • Annual influenza vaccination • Pneumococcal vaccination Adapted from: Global Initiative for Chronic Obstructive Pulmonary Disease, Executive Summary: Global Strategy for the Diagnosis, Management, and Prevention of COPD (Accessed November 8, 2013) Regular physical activity Adapted from: Global Initiative for Chronic Obstructive Pulmonary Disease, Executive Summary: Global Strategy for the Diagnosis, Management, and Prevention of COPD (Accessed November 8, 2013) • Long-term oxygen therapy if chronic hypoxemia Bronchodilators 18 The Cornerstone of ..... COPD management 19 Bronchodilators Inhalers • It maximizes the bronchodilator's direct effect on the airways • While minimizing systemic effects 20 Bronchodilators Inhaled β 2 agonists Inhaled Anticholinergics Short-acting Short-acting Long-acting Long-acting Theophylline 21 Delivery of Inhaled Medication 1. Metered Dose Inhalers ( MDI) 2. Dry Powder Inhalers ( DPI) 3. Nebulizers Metered Dose Inhalers (MDI) 22 (A) AeroChamber (B) AeroChamber with mask (C) InspirEase Examples of various dry powder inhalers Panels A, B, E, F, and G: Courtesy of Dean Hess, RRT, PhD. Panel C: Image used with permission. Copyright © 2012 Novartis Pharmaceuticals Corporation. Panel24 D: Image used with permission. Copyright © 2013 Novartis Pharmaceuticals Corporation. A. B. C. D. Aerolizer HandiHaler Neohaler Tobi Podhaler E. F. G. H. Flexhaler Diskus Twisthaler Ellipta 26 Metered Dose Inhalers (MDI) Dry Powder Inhalers (DPI) • Improve compliance • Reduce extra medication usage and patient cost Nebulizers 27 28 29 The Effects of Bronchodilators Long-term improvements in symptoms Exercise Capacity Airflow Limitation (even when there is no spirometric improvement following a single test dose) Cooper CB, Tashkin DP. Recent developments in inhaled therapy in stable chronic obstructive pulmonary disease. BMJ 2005; 330:640/Sin DD, McAlister FA, Man SF, Anthonisen NR. Contemporary management of chronic obstructive pulmonary disease: scientific review. JAMA 2003; 290:2301/Man SF, McAlister FA, Anthonisen NR, Sin DD. Contemporary management of chronic obstructive pulmonary disease: clinical applications. JAMA 2003; 290:2313/Ferguson GT, Cherniack RM. Management of chronic obstructive pulmonary disease. N Engl J Med 1993; 328:1017/Hanania NA, Celli BR, Donohue JF, Martin UJ. Bronchodilator reversibility in COPD. Chest 2011; 140:1055. Short-acting Bronchodilators 31 Short-acting bronchodilators I. Short-Acting Beta Agonists (SABA) II. Short-Acting Muscarinic Antagonist (anticholinergics) (SAMA) Short-Acting Beta Agonists (SABA) β2-agonist out β2R Gs Gs AC cAMP PKA (active) in ATP PK (inactive) Relaxation Smooth muscle Adapted from Cazzola & Molimard. Pulm Pharmacol Ther 2010 34 Short-acting bronchodilators SABA / SAMA • Appropriate medication Mild intermittent symptoms . • The advantage of SABA Rapid onset of action 35 SABA or SAMA • Monotherapy is acceptable In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. COMBIVENT Inhalation Aerosol Study Group. Chest 1994; 105:1411 Change in FEV1 (%) Short-acting Bronchodilators: Onset and Duration of Action 40 35 30 25 20 15 10 5 0 -5 N=534 P<0.001 for the combination versus each agent alone Ipratropium + Albuterol (n=173) Ipratropium (n=176) Albuterol (n=165) 0 1 2 3 4 5 Post-dose (hours) 6 Adapted from COMBIVENT Inhalation Aerosol Study Group. Chest. 1994;105:1411-1419. Reproduced with permission from American College of Chest Physicians. 7 8 37 Combination therapy is often preferred SABA + SAMA • Achieves a greater bronchodilator response than either one alone In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. COMBIVENT Inhalation Aerosol Study Group. Chest 1994; 105:1411 38 Short-Acting Beta Agonists (SABA) • SABA Salbutamol A l b u te ro l L e va l b u te ro l Te r b u t a l i n e • They have been proven in randomized, controlled trials and meta -analyses to I m p ro ve sy m p t o m s I m p ro ve l u n g f u n c t i o n Ram FS, Sestini P. Regular inhaled short acting beta2 agonists for the management of stable chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. Thorax 2003; 58:580 39 Short-Acting Beta Agonists (SABA) • Prescribed on an as-needed basis • Patients A + C ( Less symptoms) Ram FS, Sestini P. Regular inhaled short acting beta2 agonists for the management of stable chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. Thorax 2003; 58:580 40 Short-Acting Beta Agonists (SABA) • Regularly scheduled use ? No clear benefits Cook D, Guyatt G, Wong E, et al. Regular versus as-needed short-acting inhaled beta-agonist therapy for chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2001; 163:85. 41 Short-Acting Beta Agonists (SABA) • Safe When used at the recommended doses Cook D, Guyatt G, Wong E, et al. Regular versus as-needed short-acting inhaled beta-agonist therapy for chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2001; 163:85. Overuse Risks of β 2 -agonist 42 43 β2 –agonist Peripheral arterial dilation Reflex tac hycardia 44 β2 –agonist Hypokalemia Extreme Cases 45 • A serum potassium level of less than 3.5 mEq/L (3.5 mmol/L) 46 • A serum potassium level of less than less than 2.5 mEq/L 48 • β2 agonists taken as tablets can cause more severe side effects such as: Ner vousness Palpitation Cramps in the muscles Drowsiness Tremors S. Ramaiah - Asthma - 2005 49 Risks of beta-agonist overuse • Oral beta-2 agonists are generally Not Prescribed because their incidence of side effects is particularly high Tachyphylaxis • An acute rapid decrease in response to a drug after its administration Bunnel, Craig A. Intensive Review of Internal Medicine, Harvard Medical School 2009 Tachyphylaxis It can occur after an Initial Dose Or After a series of Small Doses Bunnel, Craig A. Intensive Review of Internal Medicine, Harvard Medical School 2009 Tachyphylaxis • Increasing the dose of the drug May be able to restore the original response Lehne, Richard A. (2013). "Tachyphylaxis". Pharmacology for Nursing Care. Philadelphia: Saunders. p. 81. ISBN 978-14377-3582-6. 53 Tachyphylaxis • Polymorphisms of the beta-2 receptor play a role in tachyphylaxis • Glycine at position 16 (greater receptor downregulation by endogenous catecholamines) > Arg-16 Somme Studies Safety Short-Acting Beta Agonists (SABA) Wilchesky M, Ernst P, Brophy JM, et al. Bronchodilator use and the risk of arrhythmia in COPD: part 2: reassessment in the larger Quebec cohort. Chest 2012; 142:305 55 Safety : SABA • The rate of severe cardiac arrhythmia New use of oral or inhaled short acting beta agonist ( R R 1 . 2 7 , 9 5 % C I 1.03-1.57) Wilchesky M, Ernst P, Brophy JM, et al. Bronchodilator use and the risk of arrhythmia in COPD: part 2: reassessment in the larger Quebec cohort. Chest 2012; 142:305 56 Safety : SABA Cardiac arrests Atrial fibrillation /flutter was most common Wilchesky M, Ernst P, Brophy JM, et al. Bronchodilator use and the risk of arrhythmia in COPD: part 2: reassessment in the larger Quebec cohort. Chest 2012; 142:305 57 Sinus Rhythm Atrial fibrillation The purple arrow indicates a P wave, which is lost in atrial fibrillation https://commons.wikimedia.org/wiki/File:Afib_ecg.jpg 58 https://commons.wikimedia.org/wiki/File:Afib_ecg.jpg