Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
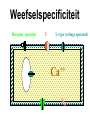
hartfalen Mortaliteit door chronisch hartfalen > 70% op 8 jaar. Harttransplant is de enige mogelijke genezing, maar < 5% van deze patiënten komen daarvoor in aanmerking. Palliatieve zorgen wordt bij end-stage hartfalen erg belangrijk. Symptomen/klachten van deze patiënten in eindfase (laatste weken): angst, pijn, dyspnoe, oedemen, vermoeidheid, depressie, anorexie, incontinentie, constipatie Farmacotherapie van palliatieve zorgen in deze fase omvat O2, anxiolytica, morfine of andere narcotica, en antidepressiva, diuretica, digoxin, ACE inhibitoren, ARBs, en ß-blockers. • Small doses of morphine sulfate, such as 2-3 mg taken orally, may relieve dyspnea and pain. Doses may be titrated upwards as needed. Drug Therapy Recommendations for Chronic HF from the 2005 ACC/AHA Guidelines Summary • the importance of – risk factor modification – early detection – therapies proven to prevent and/or reduce morbidity and mortality. • HF cannot be cured with drug therapy lifelong follow-up and patient education are needed to promote adherence to diet and medications. digoxin • Sinusritme en HF: -geen impact op mortaliteit -minder HF hospitalisaties 30% (p < 0.001) • goede keuze bij VKF en HF (CCB en BB in voldoende dosis vaak niet verdragen) • Cave hypokaliëmie • Cave nauw therapeutisch venster en interacties Incidence of Death or Severe Congestive Heart Failure during Six Weeks of Treatment with Zofenopril or Placebo in Patients with Acute Myocardial Infarction Ambrosioni E et al. N Engl J Med 1995;332:80-85 Cumulative Mortality during One Year of Follow-up among Patients with Acute Myocardial Infarction Treated for Six Weeks with Zofenopril or Placebo Ambrosioni E et al. N Engl J Med 1995;332:80-85 Cumulative Incidence of Death from All Causes after Six Weeks of Treatment with Zofenopril or Placebo, Regardless of Whether There Was Prior Congestive Heart Failure Ambrosioni E et al. N Engl J Med 1995;332:80-85 β blockers in heart failure Potential mechanisms and benefits of β blockers: improved left ventricular function; reduced sympathetic tone; improved autonomic nervous system balance; up regulation of β adrenergic receptors; reduction in arrhythmias, ischaemia, further infarction, myocardial fibrosis, and apoptosis Antithrombotic treatment • In patients with chronic heart failure the incidence of stroke and thromboembolism is significantly higher in the presence of atrial and left ventricular dilatation, particularly in severe left ventricular dysfunction. Nevertheless, there is conflicting evidence of benefit from routine treatment of patients with heart failure who are in sinus rhythm with antithrombotic treatment, although anticoagulation should be considered in the presence of mobile ventricular thrombus, atrial fibrillation, and severe cardiac impairment. Large scale, prospective RCT of antithrombotic treatment in heart failure are in progress, such as the WATCH study (a trial of warfarin and antiplatelet therapy); the full results are awaited with interest. • The combination of atrial fibrillation and heart failure (or evidence of left ventricular systolic dysfunction on echocardiography) is associated with a particularly high risk of thromboembolism, which is reduced by long term treatment with warfarin. Chronic heart failure and atrial fibrillation • Restoration and long term maintenance of sinus rhythm is less successful in the presence of severe structural heart disease, particularly when the atrial fibrillation is longstanding. In patients with a deterioration in symptoms that is associated with recent onset atrial fibrillation, treatment with amiodarone increases the long term success rate of cardioversion. Digoxin is otherwise appropriate for controlling ventricular rate in most patients with heart failure and chronic atrial fibrillation, with the addition of amiodarone in resistant cases. diuretica • • The guidelines note that periodic weight and symptom assessment should direct diuretic dosage adjustment, based on the patient's fluid status. In a nurse-driven telephone follow-up program, recently discharged HF patients were contacted at least weekly. Nurses assessed patients for symptoms of HF exacerbation and adjusted diuretic doses as appropriate. After one year, this intervention resulted in a 30% reduction in emergency department visits (p = 0.029) and readmissions (p = 0.045).[45] In another study, a patient-driven sliding-scale diuretic protocol in patients with NYHA Class II-IV HF resulted in a 90% reduction in emergency department visits (p = 0.015).[46] Diuretic dose adjustment was based on a 6 point questionnaire that evaluated signs (daily weights) and symptoms (dyspnea, peripheral edema) of HF. These data suggest that a flexible dosing strategy could enhance diuretic effectiveness.The relationship between diuretic use and the efficacy and safety of other HF therapies is also important. Symptoms of volume overload can arise upon initiation or dose escalation of a ß-blocker. Some ß-blocker clinical trials managed this complication by increasing the diuretic dose to regain a euvolemic state and improve tolerance of the increased ß-blocker dose.[40,43] Diureticinduced volume depletion can negatively impact titration of both ACE inhibitors and ß-blockers by increasing the risk of hypotension. In the absence of fluid overload, diuretic dosage reduction should be considered. Cox-inhibitoren en HF • Cyclooxygenase (COX) inhibitors (both COX-2 selective and nonselective) can cause fluid retention and congestive symptoms, which may attenuate diuretic efficacy. • Thus, these agents should be used cautiously or avoided entirely in HF patients. The renal effects of COX inhibitors, along with diuretic-associated volume depletion, may result in additive risks of renal dysfunction. diuretica en HF Diuretic resistance may develop in -patients taking COX inhibitors -in those with significant renal impairment or excess sodium intake Angor Met dank aan Professor Dr. Luc Hondeghem Definitie Behoefte > Toevoer = Angor accumulatie metabolieten zuurstof tekort Behandeling Behoefte > Toevoer = Angor Behoefte Stress=wandspanning • volume van ventrikel R2 • druk in ventrikel • wanddikte Hartfrequentie Contractiliteit Toevoer Bloeddruk (perfusiedruk) Diastoleduur Diameter (weerstand) Gladde spier Ca++ i Ca++-calmodulin b-receptor c-AMP NO c-GMP MLCK.PO 4 Myosin-LC-PO4 actin Contractie Myosin-LC MLCK * actin Relaxatie 200 ml 100 ml 100 ml 110 ml 10 ml 100 ml 200 ml 110 ml Dilatatie 10 ml 100 ml 5 ml 195 ml STEAL 200 ml 110 ml Dilatatie 10 ml 100 ml 5 ml 195 ml Angor klassieke (atherosclerose) .... behoefte vasospastische (variant, Prinz-metal). vasodilatatie onstabiele (dreigend infarct) Behandeling Nitraten b-blokkers Calciumkanaalblokkers Behoefte ( ) Toevoer Nitraten nitroglycerine (sublinguaal, oraal, pleister/zalf) relaxatie (vooral veneus) ... verminderde input ... output kleiner hart, lagere druk maar, tachycardie (reflex) b-blokkers verhoogde contractiliteit Opgepast vers, in glazen flesje en alleen! orthostatische hypotensie pulserende hoofdpijn Monday disease (verminderde tolerantie) Sunday disease (afhankelijkheid) Amylnitriet inhalatie • Arteriële vasodilatie • Venoconstriction (reflex) •Corpus cavernosum ++ Ca -kanaal blokkers Phenylalkylamines (Verapamil) Dihydropyridines (Nifedipine) Benzothiazepines (Diltiazem) Selectivity ++ Ca -Kanaal + + + + + N + + + + + + + + + + + + + + + Inactivation Activation H2N HOOC D+ V- Weefselspecificiteit Receptor operated T- L-type (voltage operated) ++ Ca N Relaxatie bloedvaten (N,D,V) • vooral arteriolen (oedeem vnl. door extravasatie) • minder venen (geen orthostatische hypotensie) hart (D,V) (N heeft al perifere effecten bij dosis die nog geen cardiaal effect heeft) • SA, AVB, CHF skeletspieren 0 bronchi, GI (constipatie) Angor vasodilatatie ... verlaagde bloeddruk contractiliteit hartfrequentie ( N, ~ D, V) coronaire spasmen (vasosp. angor) angor acute aanval Organische nitraten CCB β-blockers onderhoudstherapie + + (+) + - + Eerste (thuis)behandeling bij klinisch vermoeden van acuut myocardinfarct: • 300 mg (snel resorbeerbaar) ASA po • nitraten SL (niet teveel) • morfine iv of sc (niet im) ALLHAT Cumulative Event Rates for All-Cause Mortality by ALLHAT Treatment Group .3 Cumulative Mortality Rate .25 HR (95% CI) p value A/C 0.96 (0.89-1.02) 0.20 L/C 1.00 (0.94-1.08) 0.90 .2 Chlorthalidone Amlodipine Lisinopril .15 .1 .05 0 0 Number at risk: Chlor 15,255 Amlo 9,048 Lisin 9,054 1 14,933 8,847 8,853 2 14,564 8,654 8,612 3 4 Years to Death 14,077 8,391 8,318 12,480 7,442 7,382 5 7.185 4,312 4,304 6 3,523 2,101 2,121 7 4288 217 144 ALLHAT Cumulative Event Rates for All-Cause Mortality by ALLHAT Treatment Group .3 Cumulative Mortality Rate .25 HR (95% CI) p value A/C 0.96 (0.89-1.02) 0.20 L/C 1.00 (0.94-1.08) 0.90 .2 Chlorthalidone Amlodipine Lisinopril .15 .1 .05 0 0 Number at risk: Chlor 15,255 Amlo 9,048 Lisin 9,054 1 14,933 8,847 8,853 2 14,564 8,654 8,612 3 4 Years to Death 14,077 8,391 8,318 12,480 7,442 7,382 5 7.185 4,312 4,304 6 3,523 2,101 2,121 7 4288 217 144